The prevalence of internet addiction and its association with quality of life among inflight security officers based on a national survey: a network analysis perspective
Zhen Gui, He-Li Sun, Yuan Feng, Qinge Zhang, Zhaohui Su, Teris Cheung, Gabor S. Ungvari, Erliang Zhang, Minzhi Chen, Jie Zhang, Lin Zhang, Bin Ren, Qingqing Jin, Chee H. Ng, Mi Xiang, Yu-Tao Xiang

TL;DR
This study finds that internet addiction is common among flight security officers in China and is linked to lower quality of life, suggesting targeted interventions could help.
Contribution
The study introduces a network analysis approach to identify central symptoms of internet addiction and their impact on quality of life in a specific occupational group.
Findings
Internet addiction prevalence among IFSO was 13.1%, with lower income and mental health issues linked to higher risk.
Network analysis identified key symptoms like job performance decline and preoccupation with the internet as central to internet addiction.
Symptoms like sleep loss and social withdrawal were most harmful to quality of life, while forming online relationships was beneficial.
Abstract
Given the heavy responsibilities placed on inflight security officers (IFSO) to ensure passenger safety and eliminate inflight hazards, they often turn to Internet use to cope with their work pressure. This study examined the prevalence of internet addiction (IA) among IFSO in China, and its associated factors, relationship with quality of life (QOL), and network structure. This was a cross-sectional study based on a national survey. Expected influence (EI) was used to identify the most central nodes within the network model. Among 3,475 IFSO included in this study across 10 airlines, the prevalence of IA (IAT-20 total score of ≥ 50) was 13.1% (n = 454; 95% CI: 11.9–14.2%). Further, there was an association between lower annual income, more severe depressive symptoms and anxiety symptoms with IA among IFSOs. Network analysis found that “Job performance or productivity suffer because…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
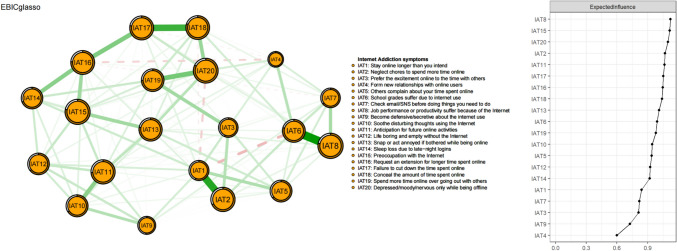 Figure 1
Figure 1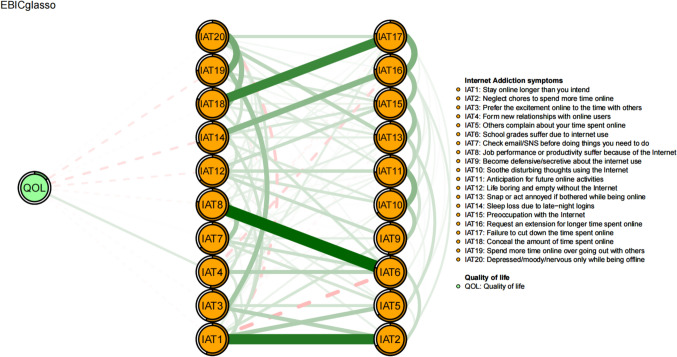 Figure 2
Figure 2- —http://dx.doi.org/10.13039/501100001809National Natural Science Foundation of China
- —Shanghai Science and Technology Development Funds
- —Science Foundation of Ministry of Education of China
- —Civil aviation safety capacity building project
- —University of Macau
- —University of Melbourne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMental Health Research Topics · Impact of Technology on Adolescents · Complex Network Analysis Techniques
Introduction
In China alone, the air industry reported that passenger aircrafts completed 4.92 million flights, totaling 12.21 million flight hours, and transported 620 million passengers, representing year-on-year increases of 94.5%, 91.8%, and 146.1%, respectively in 2023 [1]. Given that aviation security and safety has become a high priority worldwide, the Chinese government has therefore highlighted the important role of inflight security officers (IFSO) [2].
IFSO refer to aircrew who are deployed on aircraft to perform air safety and security tasks authorized by the government of the operator's country of registration. Their primary work responsibility is to protect the aircraft and their occupants from unlawful interference [3], ensure the safety of passengers and eliminate safety hazards. Furthermore, they need to have specialized work skills, strong psychological qualities and keen ability to identify risks [4]. Although the work environment of IFSO can be stressful and complex, the routine work content is usually monotonous, which makes IFSO prone to work fatigue. Due to frequent time zone changes, long-distance flights and shift work patterns with a lack of regular work and rest schedules, IFSO usually experience high levels of work intensity, pressure and fatigue [5]. As a result, they often turn to Internet resources for relaxation and communication [6].
Over the past decades, excessive use of the Internet has become a common problem [7, 8], and the risk of Internet addiction (IA) has been increasing across many populations [9]. IA refers to a range of problems due to a lack of control over Internet use, withdrawal symptoms and tolerance characteristics [10, 11]. Notably, IA is not classified as a psychiatric diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [12], whereas Internet Gaming Disorder (IGD) is listed in the International Classification of Diseases 11 th Revision (ICD-11) [13], and may also be referred to as “Gaming Addiction,” or “Internet Use Disorder,” or “Internet Addiction” [14]. A meta-analysis of data from 31 countries worldwide revealed that the prevalence of IA varied widely ranging from 0.5% to 40%, with the overall prevalence of 7.02% (95% confidence interval (CI): 6.09–8.08%) [15]. In addition, the risk factors of IA commonly reported included young age, male gender, low self-esteem, loneliness and social isolation [16, 17]. Due to high work pressure and irregular schedules, the Internet is often the main source of social interaction, leisure activities, and stress relief for IFSO [6, 18]. However, IA is also related to a host of negative psychological health problems (such as depression and harmful alcohol use), poor cognitive performance, increased hostility/aggression, interpersonal difficulties and decreased quality of life (QOL) [19–21]. From an aetiological view point, IA is closely associated with functional and structural changes in the prefrontal cortex and striatum, which may impair impulse control [22, 23]. Furthermore, extensive use of the Internet and digital devices, family dysfunction, and social pressures are factors that can increase the risk of IA [23, 24]. Since IA involves biopsychosocial factors, effective intervention to prevent and treat IA requires a multidisciplinary approach such as cognitive behavioral therapy (CBT) [25], pharmacological treatment (such as selective serotonin reuptake inhibitors, SSRIs) [26], digital literacy education, and lifestyle modifications [27]. To facilitate the evaluation of IA in both research and clinical practice, various questionnaires to measure IA have been developed. Of them, the Internet Addiction Test (IAT) is the most commonly used and reliable instrument globally [28].
Network analysis is a data-driven statistical method for assessing and visualizing the structure and interconnections of psychiatric symptoms [29, 30]. Compared to traditional statistical methods, network analysis identifies central symptoms and elucidates the complex relationships between symptoms within a network model [31, 32]. Targeting central symptoms can improve treatment efficacy by addressing the mechanisms involved in the aetiology and maintenance of psychiatric problems [29]. Network analysis has been widely used among psychiatric disorders, including major psychiatric disorders [33], anxiety [34], suicidality [35], problematic smartphone use symptoms [36] and IA [37]. For example, a network analysis of major depressive disorder (MDD) patients revealed that the “Preoccupation with the Internet” was the most influential (central) symptom in IA [38]. However, to date, most network analysis researches of IA mainly paid close attention to children and adolescents as well as those with psychiatric problems [33, 39–42]. Due to the different characteristics of such study samples, previous results could not be generalized to other groups such as IFSO in which there is a paucity of research.
To address this research gap, this study explored the prevalence and associated factors of IA, and its relationship with QOL and network structure among IFSO in China, using the nationally representative data from the Civil Aviation Health Cohort of China (CAHCC). As QOL is a widely used indicator of health outcomes, understanding its associations with IA symptoms is crucial for mitigating the negative impacts of IA on QOL [43].
Methods
Study design and participants
Following previous studies [44, 45], a convenience sampling method was adopted for this study due to logistical reasons. A questionnaire link was sent to all IFSO working in the participating airline companies through the Short Message Service (SMS) function of the Questionnaire Star online questionnaire platform. Recipients could access the survey by clicking the provided link and then completing it online. In addition, the baseline assessment data was collected from December 2022 to March 2023 in a national survey, the study included IFSO from 10 airline companies nationwide in China. To achieve a satisfactory response rate, a supervision group consisting of team leaders of IFSO from each participating company was set up to monitor the response rate daily. To increase the participation rate of IFSO, the team leaders in the participating airline company encouraged the IFSO to complete the assessment during the study period. The participants were: 1) working as IFSO during the survey period; 2) older than 18 years; 3) able to provide electronic written informed consent. Those with a history of psychiatric disorders including substance and alcohol dependence were excluded. In addition, The Ethics Committee of Civil Aviation Shanghai Hospital has approved this research protocol.
Measures
The sociodemographic information including age, gender, education level, marital status, annual income level, and working duration were collected. The validated Chinese version of the self-reported 20-item Internet Addiction Test (IAT-20) was used to evaluate the IA symptoms over the past month [46, 47]. The IAT-20 contains 20 items across six domains: Excessive use, Salience, Neglect work, Anticipation, Lack of control, and Neglect social life. Each item is rated on a 5-point Likert scale from"1"(rarely) to"5"(always), with the total score ranging from 20 to 100 points. The IAT has been validated in Chinese populations [35].Following previous studies [33, 48], participants with a IAT total score of ≥ 50 was defined as “having Internet addiction” [28, 49, 50]. Such dichotomization could enable the application of binary logistic regression to examine the associated factors of IA in a clinically relevant manner.
The validated Chinese version of the nine-item Patient Health Questionnaire (PHQ-9) was used to assess the severity of depressive symptoms [51, 52]. The PHQ-9 consists of 9 items, with each item scoring from 0 to 3 (from “not at all” to “nearly every day”) and the total score ranging from 0 to 27. A higher total score indicates more severe depressive symptoms [53]. The validated Chinese version of the seven-item Generalized Anxiety Disorder scale (GAD-7) was used to assess anxiety symptoms. The GAD-7 consists of seven items, with each scoring from 0 (“not at all”) to 3 (“nearly every day”) [54, 55]. The GAD-7 total score ranges from 0 to 21, with a higher total score indicating the more severe anxiety symptoms [56].
Global quality of life (QOL) was measured using the Chinese version of the World Health Organization Quality of Life-brief version (WHOQOL-BREF) [57]. Specifically, QoL was measured as the sum of the first two items: “How would you rate your quality of life?” and “How satisfied are you with your health?”. The validity of such QoL measure has been well established and widely used across Chinese populations [58, 59]. Each item is scored from 1 (extremely dissatisfied) to 5 (extremely satisfied) and the total score ranges from 2 to 10 points. [60].
Statistical analysis
Univariate and multivariate analyses
In this study, univariate and multivariate analyses were used the SPSS 27.0 (SPSS Inc., Chicago, Illinois, USA). The characteristic data between subgroups with and without IA symptoms were compared using independent sample t-tests for continuous variables and Chi-square tests for categorical variables. After controlling for variables with significant group differences in univariate analyses, analysis of covariance (ANCOVA) was used to compare QOL between IFSO with and those without IA. Binary logistic regression analysis was used to test the independent associated factors of IA, and variables with significant differences between groups in the univariate analysis were entered as independent variables. P < 0.05 was set as statistically significant (two-tailed).
Network analysis
R program (Version 4.3.1) [61] was used for the network analysis to examine the interconnections between IA symptoms in IFSO. Network analysis is an innovative statistical method that visualizes the relationships between different symptoms in a network model, where node represents IA symptoms, and the edge between the two nodes represents the correlation between both symptoms. A thicker edge signifies a stronger correlations, while the color denotes the direction: green edge indicating positive correlations, while red edge indicating a negative correlation [62].
The estimateNetwork function in the “networktools” package (Version 1.5.1) [63] with the “EBICglasso” method was used to estimate the network model of IA symptoms. The “qgraph” package (Version 1.9.8) [62] and the “ggplot2” package (Version 3.4.4) [64] were used for network visualization and optimizing network visualization, respectively. To accurately evaluate the association between different IA symptoms in the network model, we used the Extended Bayesian Information Criterion (EBIC) [62] and Graphical Gaussian Model (GGM) with the least absolute shrinkage and selection operator (LASSO) [62] to simplify the network model and improve its interpretability [65].
In the network model where individual symptoms are treated as nodes, a greater centrality index of nodes indicates a higher importance of symptoms within the network model. Following previous research [66, 67], to identify the most central (influential) symptoms in the network model, we calculated the centrality measure to quantify the importance of network nodes. Among the various centrality indices, expected influence (EI) was adopted because it could indicate both positive and negative edge weights, providing a more comprehensive measure of the overall impact of symptoms. The EI centrality was calculated by summarizing the sum of positive and negative edges connected to a specific node, which could identify the most influential nodes within the network model [68]. In contrast, other measures of centrality, such as strength centrality, could only calculate the absolute value of the connection but ignore the directional effects of symptoms. A larger EI value indicates the greater the node's influence within the network model. Since the central (influential) symptoms are more closely related to other symptoms in the network model, treatment that target the most central symptoms could be more effective in improving the psychiatric disorder or syndrome [69].
Moreover, “mgm” (Version 1.2–14) [70] was used to calculate the predictability for IA symptoms, thereby quantify the degree to which each symptom could be explained by its direct connections within the network. In addition, the flow function in the “qgraph” package (Version 1.9.8) [62] was used to identify specific IA symptoms that were directly and indirectly related to QOL.
R-package “bootnet” (Version 1.5.6) [71] was used to evaluate the EI centrality stability and edge accuracy. Bootstring difference tests were used to evaluate the robustness of edges and nodes EI in the network model, in which correlation stability coefficient (CS coefficient) was used to evaluate the robustness of EI centrality. When CS coefficient was greater than 0.25, the results of the network model were stable and reliable. The network with CS-coefficient greater than 0.5 had better robustness [72]. The accuracy of the edge was estimated using the bootstrap 95% confidence interval (CI), and the narrower the estimated 95%CI, the higher the reliability of the network [72]. When 1,000-bootstrap 95% confidence interval (CI) value range did not contain zero, the difference between two nodes or two edges was significant.
Results
Study sample and descriptive statistics
Of a total of 3,755 in-service IFSO from 10 airlines invited to participate in the survey, 3,475 met the inclusion criteria and completed the assessment, with a participation rate of 92.54%. The demographic characteristics are presented in Table 2. The mean age of the study sample was 31.4 (standard deviation (SD) = 5.76) years, and the majority were male, accounting for 97.9% of the sample. In addition, 41.9% of the participants had a college degree or above, and the mean working duration was 8.13 (SD = 6.02) years. The mean PHQ-9 and GAD-7 total scores were 4.35 (SD = 5.86) and 2.89 (SD = 4.67), respectively, while the score of global quality of life was 6.64 (SD = 1.71).
Prevalence and correlates of internet addition
The prevalence of IA (IAT-20 total score of ≥ 50) was 13.1% (n = 454; 95% CI: 11.9–14.2%). Details of the IAT-20 item scores are shown in Table 1. As shown in Table 2, IFSO with IA were positively associated with having a bachelor or higher education (P = 0.044), married status (P = 0.047), an annual income of less than 100,000 RMB (P = 0.004) and longer work duration (years) (P = 0.008) when compared to those without IA. Additionally, compared with IFSO without IA, those with IA had higher PHQ-9 (P < 0.001) and GAD-7 (P < 0.001) total scores, but had lower global QOL (P < 0.001). After controlling for variables with significant inter-group differences in univariate analyses, the QOL in IFSO with IA (F_(1, 3,475)_ = 15.298, P < 0.001) remained lower than those without IA. A binary logistic regression analysis revealed independent associations between more severe depressive symptoms (OR = 1.105; P < 0.001) and anxiety symptoms (OR = 1.102; P < 0.001) with a higher risk of IA. In addition, participants with an annual income of more than 100,000RMB (OR = 0.728; P = 0.027) exhibited a lower risk of IA (Table 3).Table 1. Item statistics of the internet addiction testItemsAbbreviationsMean (SD)EI^a^Predictability1Stay online longer than you intendIAT12.09 (1.22)0.830.562Neglect chores to spend more time onlineIAT21.77 (1.05)1.070.683Prefer the excitement online to the time with othersIAT31.76 (1.08)0.810.564Form new relationships with online usersIAT41.55 (0.93)0.590.515Others complain about your time spent onlineIAT51.67 (0.99)0.930.646School grades suffer due to internet useIAT61.41 (0.84)0.990.797Check email/SNS before doing things you need to doIAT71.50 (0.91)0.810.648Job performance or productivity suffer because of the InternetIAT81.44 (0.86)1.120.789Become defensive/secretive about the internet useIAT91.77 (1.10)0.720.5110Soothe disturbing thoughts using the InternetIAT101.65 (1.01)0.940.6611Anticipation for future online activitiesIAT111.55 (0.95)1.060.7312Life boring and empty without the InternetIAT121.63 (1.01)0.920.6413Snap or act annoyed if bothered while being onlineIAT131.48 (0.88)1.010.7814Sleep loss due to late-night loginsIAT141.63 (1.00)0.920.6915Preoccupation with the InternetIAT151.54 (0.91)1.110.7816Request an extension for longer time spent onlineIAT161.59 (0.96)1.040.7517Failure to cut down the time spent onlineIAT171.50 (0.91)1.050.7818Conceal the amount of time spent onlineIAT181.44 (0.87)1.040.8019Spend more time online over going out with othersIAT191.48 (0.91)0.970.7420Depressed/moody/nervous only while being offlineIAT201.42 (0.86)1.090.82EI expected influence, IAT Internet Addiction Test, SD standard deviation^a^The value of EI is shown as raw dataTable 2Characteristics of Inflight security officers with and without Internet addictionVariablesTotal (N = 3,475)Without Internet Addiction(N = 3,021)With Internet Addiction(N = 454)Univariable analysisN%N%N% \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi^{2}$$\end{document} df**pMale3,40297.92,95697.844698.20.29110.589Bachelor or above education1,45641.91,24641.221046.34.07110.044Married status2,18963.01,88462.430567.23.92910.047Yearly income ≤ RMB^b^ 100,0002,62075.42,25374.636780.88.33510.004MeanSDMeanSDMeanSDZdf**pAge (years)31.405.7631.345.7131.796.05− 1.550–0.121Work duration (years)8.136.028.035.938.836.59− 2.662–0.008PHQ9-total4.355.863.384.8210.787.79− 27.688–* < 0.001GAD7-total2.894.672.123.788.056.42− 27.913–* < 0.001Global quality of life6.641.716.811.635.471.8016.082–* < 0.001Bolded values: < 0.05df degree of freedom, GAD-7 the 7-item Generalized Anxiety Disorder, IAT-20 the 20-item Internet Addiction Test, PHQ-9 the 9-item Patient Health Questionnaire, SD standard deviation^^Mann–Whitney U test^b^1 RMB = 0.155 USDTable 3Binary logistic regression analysis of Internet addiction in Inflight security officers (N = 3,475)VariablesBinary logistic regression analysispOR95% CIBachelor or above education0.9230.9890.788–1.241Married status0.0600.7920.621–1.009Yearly income ≤ RMB^b^ 100,0000.0270.7280.549–0.965Work duration (years)0.3660.9910.972–1.010PHQ9-total** < 0.0011.1051.068–1.144GAD7-total < 0.001**1.1021.058–1.149Bolded values: < 0.05CI* confidence interval, OR odds ratio^b^1 RMB = 0.155 USD
Network structure and centrality
Figure 1 displays the network structure of IA symptoms. Of the 190 edges estimated, 128 were non-zero edges, with the mean weight of 0.05. “School grades suffer due to internet use” (IAT6)—“Job performance or productivity suffer because of the Internet” (IAT8) were the strongest edge (weight:0.60), followed by “Stay online longer than you intend” (IAT1)—“Neglect chores to spend more time online” (IAT2) (weight: 0.52), and “Failure to cut down the time spent online” (IAT17)—“Conceal the amount of time spent online” (IAT18) (weight: 0.46).Fig. 1. Network structure of internet addiction symptoms in inflight security officers
The EI values in the IAT network are plotted in the right panel of Fig. 1. Table 1 shows the raw data of EI values. “Job performance or productivity suffer because of the Internet” (IAT8) was the most central symptom with the highest EI value (EI: 1.12), followed by “Preoccupation with the Internet” (IAT15) (EI:1.11) and “Depressed/moody/nervous only while being offline” (IAT20) (EI: 1.09). In addition, the average predictability values of nodes in the network model was 0.69 (SD = 0.09), indicating that on average 69% of the variance of each node could be potentially explained by neighboring nodes.
Figure 2 shows the flow network of connections between QOL and the symptoms of IA. Among the IA symptoms directly related to QOL, the strongest negative edges were observed in “Sleep loss due to late-night logins” (IAT14) (average edge weight = −0.08), followed by “Spend more time online over going out with others” (IAT19) (average edge weight = −0.06). Additionally, “Form new relationships with online users” (IAT4) exhibited the strongest positive correlation with QOL (average edge weight = 0.08).Fig. 2. Flow network of quality of life and Internet addiction symptoms. Note: items in the middle of the figure indicate the direct connection to quality of life and items located on the right represent the indirect connection
Network stability and accuracy
The stability of the network model is shown in Figure S1 based on the case-dropping bootstrap method. The CS-coefficients value for EI was 0.75, indicating that the network could still maintain stability after 75% of the samples were dropped. Moreover, Figure S2 shows the accuracy of the network model. The value range of the estimation of edge weights by Bootstrap 95% CIs were narrow, indicating that the primary results were reliable.
As shown in Figure S3, the bootstrapped difference test results indicated that the most central symptoms in the network model were significantly different from most of other nodes, indicating that the EI results were robust. In addition, the bootstrapped difference test results of edge weights showed that the difference between the strongest edges and most edges were statistically significant, which supported the accuracy and reliability of the network model (Figure S4).
Discussion
This was the first study to examine the prevalence of IA as well as its associated factors, relationship with QOL and network structure among IFSO working in commercial airlines in China. Due the specific requirements needed for recruiting IFSO, most of the participants were male (97.9%) in this study. We found that IA was common among IFSO, particularly in those who had more severe anxiety and depression symptoms, and poor economic status. Network analysis identified that “Job performance or productivity suffer because of the Internet” (IAT8), “Preoccupation with the Internet” (IAT15) and “Depressed/moody/nervous only while being offline” (IAT20)"were the most central nodes. In addition, in IA-QOL network models of IFSO, “Sleep loss due to late-night logins” (IAT14) and “Spend more time online over going out with others” (IAT19) had the most negative correlation, while “Form new relationships with online users” (IAT4) had the strongest positive correlation with QOL.
We found that the prevalence of IA (IAT-20 ≥ 50) was 13.1% (95% CI: 11.9–14.2%) among IFSO, which is significantly higher than the prevalence reported in a previous systematic review [7], which ranged from 1.2% (Internet users in the UK) [73] to 9.7% (college students in Turkey) [74], as well as from 8.0% among airline pilots (95% CI: 7.3–8.6%) [75] to 11.3% among the general population (95% CI: 10.1%–12.5%) [76]. Although IA was measured using the IAT in all the studies, the reasons for the differences in prevalence might be due to the differences sample selection as well as Internet usage behaviors between various geographic locations [47, 77, 78]. However, the IA prevalence in our study was lower than the prevalence among adolescents (20.3%) and children (13.8%) in Korea [39], which might be related to several factors in children and adolescents such as the lack of self-control, perceived parental monitoring stress [42], reduced emotional stability [79], and low adaptability and conscientiousness [41].
Past studies [78, 80] found that IA was positively related to both depressive and anxiety symptoms, which was supported by our study findings. A bidirectional relationship between IA and other psychiatric disorders (e.g., depression and anxiety) has been previously demonstrated [6, 81, 82]. On the one hand, those with mental health problems might have less willingness to seek help in-person due to stigma or discrimination [83], and might be more willing to seek online help using e-mental health resources [84], thereby increasing their Internet use and the risk of IA. On the other hand, IA might also directly increase the risk of depression and anxiety [85]. For example, the survey in Korean adults found that IA group had a higher risk of depression and anxiety compared to the control group [86]. The results of this study showed that participants with lower-income levels have a higher risk of IA, which is consistent with previous findings that low-income was a predictor of IA [24, 87]. Financial difficulties have been reported as a risk factor associated with IA in adults [88]. Compared to other social activities, Internet use is a cheaper and more convenient activity for low-income IFSO with limited social support [89]. Hence, although increased Internet use could compensate for their perceived stress and isolation, turning to the Internet for social support might also increase the risk of IA [89].
“Job performance or productivity suffer because of the Internet” (IAT8) was the most influential node of the IA network, which as similar to the network model of IA among younger (aged 14–24 years) [90] and MDD patients [38]. Our results are also consistent with past research that Internet overuse might negatively influence daily work performance and reduce employee productivity [91]. Due to the work requirements of IFSO, IA may affect their work ability by interfering with their sleep patterns [92]. Frequent time zone changes, long-distance flights and changing shift work for IFSO will likely disrupt their work and rest schedules, which can result in higher risk of sleep problems than the general population [93]. Hence, excessive Internet use coupled with chronic irregular work and rest patterns may aggravate their sleep problems and negatively affect their work performance [94]. However, our findings might be unique to the occupational characteristics IFSO, which might limit the generalizability of our findings to other populations such as unemployed individuals or other non-working populations.
“Preoccupation with the Internet” (IAT15), defined as “a preoccupation with the Internet while offline or fantasizing about being online” [28], was also the key influential node in the network model. The finding is similar to past researches reported among adolescents (aged 12–20 years), young adults (aged 14–24 years) [90], pregnant and postpartum women [65] and depressed patients [95]. “Preoccupation with the Internet” (IAT15) has also been found in Previous research [40] to be a key node in activating other IA symptoms. IA patients usually start with excessive attention to the Internet and when they are offline, they often miss the use of the Internet, being unable to control their own behavior, all of which can influence their daily work and life [96, 97]. In the virtual environment of the Internet, people do not need to be seen, they can freely define their identity and self-image in any way [98]. Moreover, as IFSO often work in a closed, high-pressure, and constantly changing environment, such conditions may limit their opportunities for social interaction, increase their feelings of loneliness, and lead to a decline in social skills [3, 5, 6]. Additionally, the frequently changing work environment and time zones contribute to a sense of detachment from the real world, making them more inclined to seek social fulfillment within virtual online spaces [75, 99].
“Depressed/moody/nervous only while being offline” (IAT20) was another central symptom, which is consistent with the findings of AI network models among nursing students [34] and adolescents with autism spectrum disorder [37]. This finding may be attributed to possible withdrawal symptoms of IA while being offline which may include depressive and anxiety symptoms [100]. Further, as IFSO often use the Internet to cope with their depressive and anxious emotions resulting from their work pressure, there may be an increased tendency for anxiety and depressive symptoms when they are offline [101, 102].
Similar to our study findings, as previously reported, individuals with IA tend to experience more physical pain, cognitive impairment and psychological problems [23], poor sleep quality, financial difficulties [88], poor interpersonal relationships [81, 103], and decreased social adjustment [104], all of which may lower QOL.
In addition, our study found that “Sleep loss due to late-night logins” (IAT14) and “Spend more time online over going out with others” (IAT19) were directly and most negatively associated with QOL, which aligns with past studies showing that poorer QOL was significantly related to various IA domains [38, 65]. IA may lead to sleep problems and neglect of real-life social interactions, thereby reducing QOL. Although online gaming can create short term positive emotions for IA patients, they are often followed by a strong sense of emptiness and loneliness [87]. Previous studies have found that staying up late to use mobile devices, such as being addicted to online games, could lead to poor sleep quality, insomnia, sleep disorders and other sleep problems [105, 106], all of which could have a negative impact on daily work and QOL. Furthermore, when individuals are addicted to using the Internet to participate in social media or play online games, they are likely to socially disconnect from their friends and family in the real world and have impairment in their activities of daily life and work [91, 107, 108], which may in turn lower their QOL.
In the flow network model, “form new relationships with online users” (IAT4) showed the strongest positive correlation with QOL, which is consistent with the IA-QOL network model among patients with MDD [38]. In the immediate aftermath of the COVID-19 pandemic, during which airlines in China had maintained strict public health measures, including social distancing and conducted this study. These measures led to reduced offline social activities but increased online social interactions to enhance social contacts [109, 110], which might improve QOL, particularly in social domains.
This study has some strengths. First, we have a large sample size and high participation rate. Second, we have nationally representative sample of the IFSO across China. Third, we used the network analysis to explore the central node of IA. However, several limitations should be noted. First, due to the cross-sectional study design, causality between IA symptoms and other variables, such as depression, anxiety and QOL, could not be examined. Future longitudinal studies on the causal relationship between IA and anxiety, depression and QOL are needed to clarify whether IA leads to poor mental health or vice versa. Second, since the IAT-20 questionnaire was a self-report assessment, there might be recall bias. Third, certain relevant variables, such as substance use disorders (e.g., tobacco and alcohol use), primary online activities and behavior patterns, should be included in further research. Finally, convenience samples and the high proportion of male participants (97.9%) in this study limit the representativeness of the study sample.
In conclusion, our network study found that IA was common among IFSO, particularly among those with lower annual income and depressive and anxiety symptoms. To address IA in clinical practice, certain psychosocial interventions, such as CBT, have been widely used effectively [111]. “Job performance or productivity suffer because of the Internet” (IAT8), “Preoccupation with the Internet” (IAT15) and “Depressed/moody/nervous only while being offline” (IAT20) were identified as the most central IA symptoms. To reduce the negative outcomes associated with IA in IFSO and to improve their QOL, such symptoms should be prioritized in both treatment and preventive strategies.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 1024 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jinyu Pan (2024) The National Civil Aviation Safety Work Conference was held in Beijing (in Chinese). Available from: http://www.caacnews.com.cn/1/1/202401/t 20240105_1373726.html, China Civil Aviation News, Beijing. Accessed 22 Feb 2025
- 2Min Xiao (2024) The National Civil Aviation Work Conference was held in Beijing (in Chinese). Available from: http://www.caacnews.com.cn/tt/202401/t 20240104_1373688.html. China Civil Aviation News Accessed 22 Feb 2025
- 3Liu X, Gui Z, Chen Z M, Feng Y, Wu X D, Su Z, Cheung T, Ungvari GS, Liu X C, Yan Y R (2025) Global prevalence of internet addiction among university students: a systematic review and meta-analysis. Curr Opin Psychiatr, 38(3): 182-199. DOI: 10.1097/YCO.000000000000099410.1097/YCO.000000000000099440009750 · doi ↗ · pubmed ↗
- 4R Development Core Team (2022) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available from: https://www.R-project.org/ (Accessed 22 Feb 2025).
- 5Roderick A (2023) The impact of flight on cabin crew wellness: a literature review. Senior Honors Theses. 1-41. Available from: https://digitalcommons.liberty.edu/honors/1330/(Accessed 22 Feb 2025).