Differences in symptoms and problems experienced by patients with a life-threatening disease in specialized palliative care and basic palliative care—a nationwide cross-sectional study
Maiken Bang Hansen, Mogens Groenvold, Mette Raunkiær, Tina Broby Mikkelsen, Leslye Rojas-Concha, Cecilie Lindström Egholm

TL;DR
Patients in specialized palliative care experience more severe symptoms and problems than those in basic care, especially non-cancer patients.
Contribution
This study compares palliative care needs between specialized and basic care patients using nationwide data.
Findings
Specialized palliative care patients had higher odds of symptoms like fatigue and impaired physical functioning.
Non-cancer patients in specialized care showed more pronounced symptom severity.
The study highlights the need for better referral strategies to specialized palliative care.
Abstract
Patients with a life-threatening disease often experience palliative care needs (symptoms and problems) before death, and those with the most complex needs should be those who get access to specialized palliative care. To examine if that is the case, studies are needed comparing palliative care needs of patients with life-threatening cancer and non-cancer diseases admitted to specialized palliative care to patients receiving basic palliative care. To compare palliative care needs among patients with a life-threatening disease admitted to specialized palliative care and patients receiving basic palliative care. A secondary data analysis of symptoms/problems reported by patients in basic palliative care or at admittance to specialized palliative care in Denmark. Ordinal logistic regression was performed to study differences in the probability of experiencing each symptom/problem among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
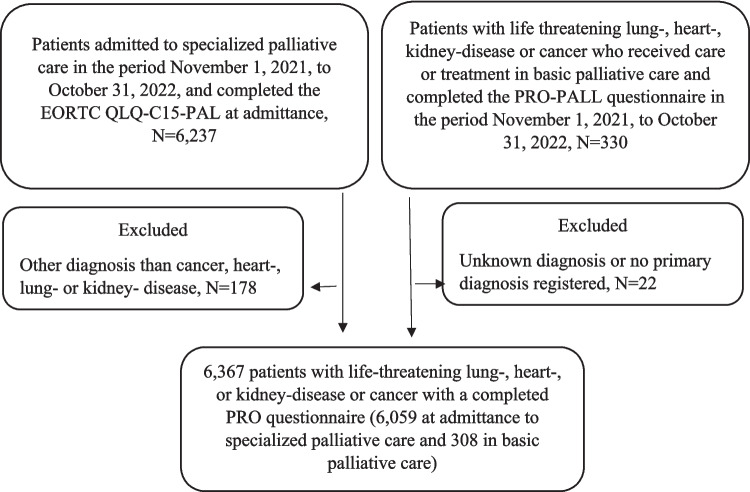 Figure 1
Figure 1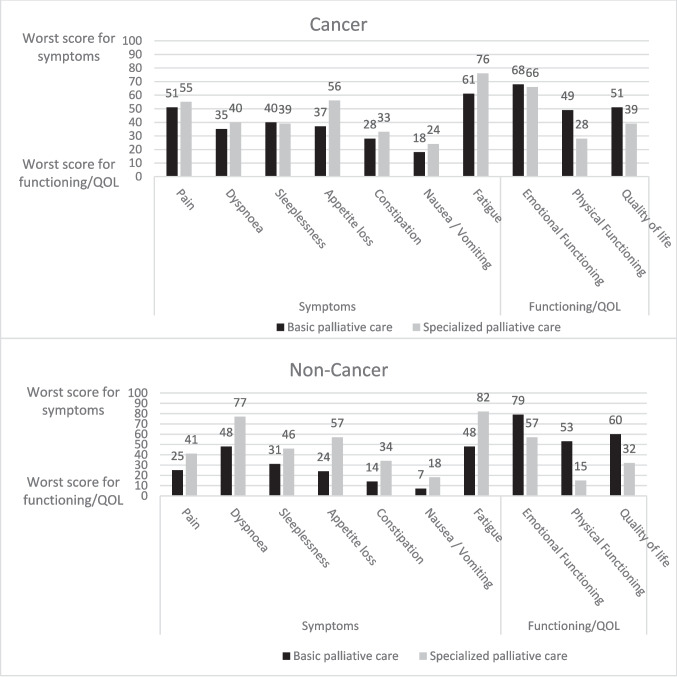 Figure 2
Figure 2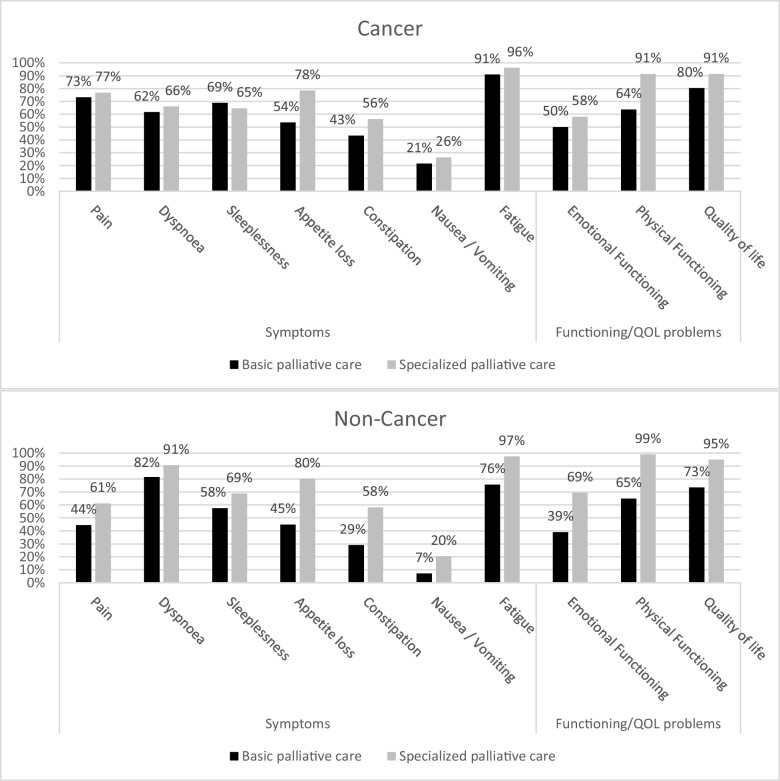 Figure 3
Figure 3- —REPHA and the Danish Health Data Authority
- —Copenhagen University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Pain Management and Opioid Use · Cancer survivorship and care
Introduction
Patients with a life-threatening disease may receive palliative care to relieve their symptoms and problems [1]. It may be general/basic palliative care provided by professionals who do not have palliative care as their main function or specialized palliative care provided by professionals with palliative care as their main function [2, 3].
In high-income countries, it is estimated that around 75% would benefit from palliative care before they die [4, 5]. Due to limited capacity, not all patients in need of specialized palliative care receive it, and this problem is expected to increase in the future due to aging populations [6–10]. Nationwide data from different countries show that only 17–19% receive specialized palliative care before they die in Denmark and Sweden [7, 11], whereas 46% receive specialized palliative care in the last year of life in Australia [9]. Patients with a non-cancer disease are less likely to receive specialized palliative care than cancer patients [6–10].
Because the capacity of specialized palliative care is limited, it is very important to provide high-quality basic palliative care for patients with life-threatening diseases and that the patients who get referred to specialized palliative care are those with the most complex palliative care needs (high levels of and/or several symptoms/problems). To identify palliative care needs and to improve the quality of palliative care, the European Association for Palliative Care (EAPC) has recommended the use of validated patient-reported outcome (PRO) tools [12, 13]. PRO tools are important to use to obtain a comprehensive needs assessment, as clinicians tend to underestimate the frequency [14, 15] and severity [16–18] of their patients’ symptoms and problems.
We have not been able to identify any studies looking at how palliative care needs differ for patients with life-threatening diseases who do and do not receive specialized palliative care in the same country or region. Therefore, the aim of this study was to compare palliative care needs (symptoms, problems, and quality of life) among patients with life-threatening diseases admitted to specialized palliative care and patients receiving basic palliative care.
Methods
Study design
This study was a secondary data analysis of cross-sectional symptom/problem data reported by patients with life-threatening diseases in basic palliative care and specialized palliative care, respectively, in a 1-year period (November 1, 2021, to October 31, 2022). The collection of PRO data is elaborated later in the “Methods” section.
Setting
In Denmark, specialized palliative care is provided by 42 palliative care teams in hospitals and by hospices [7]. Fifteen are hospital-based palliative care teams providing palliative care in their own hospital department, delivering specialized consultations in other hospital departments and providing home-based palliative care; eight additional teams also have inpatients; 15 hospices only have inpatients, whereas the remaining four hospices have inpatients and provide home-based palliative care. Basic (also called generalist) palliative care is provided in the rest of the healthcare system. Compared to non-cancer patients, cancer patients are more often referred (65% vs. 4%) and more often receive (50% vs. 2%) specialized palliative care before their death in Denmark [19].
PRO-data at admittance to specialized palliative care
In Denmark, it is mandatory for all specialized palliative care services to report information on patients referred to them to the Danish Palliative Care Database [20]. The database includes sociodemographic and clinical information and symptoms and problems reported by patients who completed the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative Care (EORTC QLQ-C15-PAL). Patients whom the healthcare professionals believe are physically and cognitively able to complete the EORTC QLQ-C15-PAL questionnaire are asked to do so at admittance to specialized palliative care (i.e., 1–3 days prior to the start date of specialized palliative care or at the start date of specialized palliative care).
The EORTC QLQ-C15-PAL is a shortened version of the EORTC QLQ-C30 adapted to cancer patients in palliative care [21], but has also been used among non-cancer patients in specialized palliative care in Denmark since 2010 [20]. EORTC QLQ-C15-PAL has been validated in several studies in patients with advanced cancer [21–28]. The EORTC QLQ-C15-PAL questionnaire assesses the severity of nine symptoms/problems by two multi-item function scales (physical and emotional functioning), two multi-item symptom scales (fatigue and pain), and five single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, and nausea) together with a single item on overall quality of life. Patients answer to which degree they have experienced each symptom and problem on a 4-point scale from “not at all” to “very much.” A 7-point scale is used to assess overall quality of life, where 1 corresponds to “very poor” and 7 to “excellent.” All questions refer to the past week, except for physical functioning, where no time frame is specified.
PRO-data from basic palliative care
In 2019, the Danish Health Data Authority established a national Clinical Coordination Group, which included healthcare professionals from different specialties from hospital departments and professionals from municipalities. With input from patients, the group developed a PRO-tool with the main purpose of identifying palliative care needs in the healthcare system outside specialized palliative care, i.e., in basic palliative care [29, 30]. The development of the new tool (the “PRO-Pall”) was completed in 2021 [31].
This study included the PRO-data collected in a feasibility test of PRO-PALL among adult patients with chronic and/or progressive life-threatening cancer or lung, kidney, or heart diseases. The PRO-data were collected in three municipalities, a research clinic, and in eight hospital departments: one cardiology department, three pulmonary medicine departments, one nephrology department, one oncology department, and two surgical departments [32]. The sites volunteered to participate in the feasibility test, and the PRO-PALL was incorporated into usual care processes.
The first part of the PRO-PALL is the EORTC QLQ-C15-PAL [21, 31]. PRO-PALL also includes two items on physical symptoms and six items on social and existential problems as well as WISP (Write In three Symptoms/Problems), allowing the patient to add up to three additional symptoms/problems using open-ended questions [32, 33]. In this study, only answers on the 15 EORTC QLQ-C15-PAL items were included since the purpose was to compare them with symptoms and problems reported at the start of specialized palliative care, where only the EORTC QLQ-C15-PAL is available.
Population
Inclusion criteria were as follows:
- 18 + years of age
- Life-threatening cancer or lung, heart, or kidney diseases
- Physically and cognitively able to complete the EORTC-QLQ-C15-PAL/PRO-Pall
- Completed the EORTC QLQ-C15-PAL at admission to specialized palliative care or the PRO-PALL questionnaire while receiving care or treatment from the municipality or at a hospital department not specialized in palliative care
Variables
Outcomes in the studies were overall quality of life and nine symptoms/problems (pain, dyspnea, sleeplessness, appetite loss, constipation, nausea, fatigue, emotional functioning, physical functioning).
The exposure variable was the setting, i.e., basic compared to specialized palliative care.
Covariates controlled for in the ordinal regression analyses were diagnosis (cancer, heart disease, lung disease, kidney disease), sex, and age.
Statistics
The 15 EORTC QLQ-C15-PAL items were converted into ten 0–100 scales according to the scoring manual [21, 34]. Higher function scale scores represent better physical or emotional functioning, or better quality of life, whereas higher symptom scale scores represent worse symptoms. Symptom/problem mean scores were computed.
The ten symptom/problem/quality of life scales were dichotomized into a new variable for experiencing a symptom/problem at least “a little” (symptom scores ≥ 33, functional scores ≤ 67) or not (symptom score < 33, function score > 67). The prevalence of each symptom/problem was calculated as the proportion of patients experiencing the symptom/problem according to setting (specialized vs. basic palliative care) and diagnosis (cancer vs. non-cancer).
Ordinal logistic regression analyses were performed to study the associations between setting (specialized vs. basic palliative care) and each outcome while controlling for the effect of diagnosis, sex, and age. If the patient had EORTC data from admittance to more than one palliative care service, only data from the first admittance was included.
The analyses were performed using SAS Enterprise Guide 8.3.
Results
Characteristics of the study population
This study included 308 patients from 12 sites providing basic palliative care and 6059 patients admitted to specialized palliative care (Fig. 1).Fig. 1. Flowchart of patients included in the study
The study included 49.1% women with a median age of 72 years (Table 1). The median age and gender distribution were similar between settings, whereas the distribution of diagnostic groups differed, with a higher proportion of cancer patients in specialized palliative care (Table 1). Table 1. Characteristics of the study populationTotal, N (%)AllBasic palliative careSpecialized palliative care63671003081006059100Sex Female, N (%)312949.115249.3297749.1 Male, N (%)323850.915650.7308250.9Age Range (N, years)636718–10230831–97605918–102 Median (N, years)63677230872605972Diagnosis Cancer, N (%)581791.411236.4570594.2 Cardiovascular disease, N (%)1221.94113.3811.3 Respiratory disease, N (%)3675.813042.22373.9 Kidney disease, N (%)611.0258.1360.6Patients reporting the highest level (“very much”) of symptoms and functioning problems on PRO-PALLPain items Had pain, N (%)176427.75116.6171328.3 Pain interfered with daily activities, N (%)163825.73912.7159926.4Short of breath (dyspnea), N (%)121419.15216.9116219.2Trouble sleeping (sleeplessness), N (%)97015.23310.793715.5Lacked appetite (appetite loss), N (%)203732.03812.3199933.0Been constipated (constipation), N (%)76912.1206.574912.4Felt nauseated (nausea/vomiting), N (%)68610.8144.567211.1Fatigue items Felt weak, N (%)267842.14915.9262943.4 Were tired, N (%)309748.67725.0302049.8Emotional functioning items Felt tense, N (%)88013.8185.886214.2 Felt depressed, N (%)5348.4237.55118.4Physical functioning items Trouble taking short walk outside of the house, N (%)302647.56922.4295748.8 Need to stay in bed or a chair during the day, N (%)305348.06420.8298949.3 Need help with eating, dressing, washing yourself or using the toilet, N (%)127520.0113.6126420.9
Mean symptom/problem and quality of life scores
Worse levels of symptoms, functioning, and quality of life were found for patients in specialized palliative care compared to patients in basic palliative care, especially among non-cancer patients (Fig. 2). Only sleeplessness among cancer patients had a slightly better (lower) score in specialized palliative care.Fig. 2. Mean symptom, functioning and overall quality of life scores according to setting and for cancer compared to non-cancer patients. The worst symptom score is 100, whereas the worst functioning and quality of life score is 0
Proportions experiencing symptoms and problems
More than 50% of cancer and non-cancer patients experienced fatigue, dyspnea, sleeplessness, impaired physical functioning, and poor quality of life at least a little in basic and specialized palliative care, respectively (Fig. 3). Except for sleeplessness among cancer patients, the prevalence of all symptoms/problems was higher in specialized palliative care compared to basic palliative care (Fig. 3).Fig. 3. Proportions of patients experiencing symptoms and problems at least “a little” according to setting and for cancer and non-cancer patients
Regression analyses
Patients in specialized palliative care had significantly higher odds of experiencing symptoms and problems compared to patients in basic palliative care (Table 2), especially higher odds of experiencing poor physical functioning (OR 8.3, 95% CI 6.6–10.5), fatigue (OR 5.1, 95% CI 4.1–6.5), and poor quality of life (OR 4.3, 95% CI 3.4–5.4). Gender, age, and diagnosis were in many cases significantly associated with the odds of experiencing symptoms/problems (Table 2). Diagnoses were strongly associated with dyspnea and the odds of dyspnea were higher among patients with lung disease (OR 9.9, 95% CI 7.8–12.5) and heart disease (OR 2.4, 95% CI 1.7–3.4), respectively, compared to cancer patients. Table 2. Odds ratios and 95% CI for higher levels of symptoms, lower functioning and lower QOL, respectively, for patients in specialized palliative care compared to patients outside specialized palliative care from ordinal logistic regressionPain (N = 6331)Dyspnea (N = 6287)Sleeplessness (N = 6261)Appetite (N = 6267)Constipation (N = 6242)OR95% CIOR95% CIOR95% CIOR95% CIOR95% CISpecialized palliative care (yes vs. no)1.81.42.22.62.03.31.41.11.83.72.94.72.31.83.0Age (10-year increase)0.90.90.91.11.11.20.80.80.91.21.21.31.01.01.1Men (vs. women)0.90.80.91.00.91.11.21.11.31.00.91.11.11.01.2Diagnosis Heart (vs. cancer)0.30.20.42.41.7****3.41.20.91.70.80.61.20.70.51.1 Respiratory (vs. cancer)0.40.40.59.97.812.51.31.01.60.90.71.11.00.81.2 Renal (vs. cancer)0.80.51.30.70.41.11.10.71.81.20.71.91.00.61.6Fatigue (N = 6180)Nausea (N = 6271)Poor emotional (N = 6020)Poor physical (N = 6216)Poor QOL (N = 5635)OR95% CIOR95% CIOR95% CIOR95% CIOR95% CISpecialized palliative care (yes vs. no)5.14.16.52.31.72.92.31.82.98.36.610.54.33.45.4Age (10-year increase)1.21.11.20.90.91.00.90.91.01.31.21.31.01.01.1Gender (men vs. women)0.80.80.90.70.60.80.90.80.90.90.8****0.91.00.91.1Diagnosis^a^^a^^a^^a^ Heart (vs. cancer)1.00.71.50.80.61.21.00.71.41.31.01.90.90.61.3 Respiratory (vs. cancer)1.31.11.60.60.50.81.91.52.32.11.72.61.51.21.9 Renal (vs. cancer)1.00.61.61.00.61.70.70.51.21.40.92.21.30.82.1Significant (P < 0.05) odds ratios in bold^a^Overall significant association between diagnosis and outcomeOdds ratios > 1 indicate more severe symptoms, lower (worse) functioning, or lower quality of life compared to the reference group
Discussion
Main findings
In basic and specialized palliative care, more than half of cancer and non-cancer patients experienced fatigue, dyspnea, sleeplessness, impaired physical functioning, and poor quality of life. Patients in specialized palliative care had significantly higher odds of experiencing symptoms and problems compared to patients in basic palliative care. Differences in the risk of symptoms/problems between settings (basic vs. specialized palliative care) were more pronounced among non-cancer patients than cancer patients.
What this study adds
Using nationwide patient-reported symptoms and problems, this study found that patients with life-threatening diseases admitted to specialized palliative care had higher odds of symptoms/problems compared to patients in basic palliative care, especially for impaired physical functioning. This is expected since patients with the most complex symptoms/problems should be those who get access to specialized palliative care. Also, patients admitted to specialized palliative care in Denmark are often admitted close to death (median survival time is 39 days after admittance) [7]; and as death approaches, the risk of symptoms and problems increases. This has been documented in systematic reviews including cancer patients with an expected survival of a maximum of 3 months, where dyspnea, appetite loss, fatigue, and poor physical function were associated with shorter survival time [35–37]. Among cancer patients referred to specialized palliative care, studies have also found impaired physical function/wellbeing [38–51], problems related to eating/weight loss [38, 39, 41–48, 50–57], dyspnea [38, 41, 42, 44–49, 51, 54, 55, 57–60], and fatigue [38, 39, 42–44, 48, 51, 53, 56] to be associated with shorter survival time. In heart failure patients, a study from the USA found that among patients who were followed in the last 6 months of their life, functional impairments, median depression scores, and the proportion reporting severe pain or dyspnea increased as death approached [61].
In our study, the difference in the prevalence of symptoms/problems between basic and specialized palliative care was larger among non-cancer patients than among cancer patients. Previous studies comparing symptoms and problems among cancer and non-cancer patients with life-threatening diseases outside specialized palliative care have also found nausea/vomiting [62, 63], constipation [62, 64], and emotional problems (sadness/depression and anxiety) [62, 64, 65] to be more prevalent among cancer patients. We found dyspnea to be more prevalent among non-cancer patients in basic palliative care, which was also found in previous studies comparing cancer patients to non-cancer patients overall [62], patients with COPD [63, 65, 66] and kidney disease [64], respectively. Fatigue and impaired physical function were experienced by the majority of patients in basic palliative care in our study. Previous studies also found that fatigue/lack of energy and impaired physical function were frequently experienced by both cancer and non-cancer patients outside specialized palliative care [62–65, 67].
In our study, non-cancer patients often had similar or higher risk of symptoms/problems in specialized palliative care compared to cancer patients. The reason for this may be that non-cancer patients are less likely to be referred to specialized palliative care before death in Denmark compared to cancer patients, and therefore, perhaps only the highly complex non-cancer patients are referred [19].
In our study, more than half of the patients in specialized palliative care experienced each of the measured symptoms/problems, except for nausea/vomiting. Symptom/problem prevalence in specialized palliative care has varied across previous studies among cancer and non-cancer patients, respectively, but many studies have also found a high prevalence of pain, fatigue, appetite loss/anorexia, and dyspnea, respectively [44, 68–88].
We found dyspnea, fatigue, and impaired physical functioning among more than half of the patients in basic palliative care. In previous studies including cancer and/or non-cancer patients with life-threatening diseases who did not receive specialized palliative care, some symptoms and problems were also experienced frequently: at least 40% experienced fatigue [62–65, 67, 89–97], drowsiness [62, 65, 67, 90], cough [62, 64, 65, 67, 89–92], and worries [62, 64, 90, 94], respectively. The dyspnea prevalence has also often been at least 50% [64, 65, 67, 89–92, 95], although it was reported to be lower in some studies [61, 66, 94, 96, 97]. Most previous studies also found physical functioning problems among a minimum of 50% of the included patients [63, 89, 94, 97] but not all [96].
Across studies (including our study), there are large variations in the proportion of patients experiencing each symptom/problem in basic as well as specialized palliative care. The variation might be due to differences in the selection of patients (e.g., diagnosis), in the assessment tools and thresholds used, and in the capacity of and the referral criteria for specialized palliative care.
Patients with heart disease and especially respiratory disease in this study had significantly higher odds of dyspnea compared to cancer patients. Similarly, previous studies outside specialized palliative care found cancer patients to have a lower risk of dyspnea compared to non-cancer patients overall [62], and to patients with chronic obstructive pulmonary disease (COPD) [63, 65, 66] or heart failure [63]. Studies among patients referred to specialized palliative care have also found non-cancer patients had a higher risk of dyspnea compared to cancer patients [98–101], and two systematic reviews found that more than 70% of patients with advanced COPD receiving palliative care often experienced dyspnea [102, 103].
The fact that many patients in basic palliative care in this study had symptoms and problems identified when using the PRO-PALL questionnaire underlines the need for healthcare professionals outside specialized palliative care to be adequately trained/educated in providing palliative care, including being trained in using patient-reported outcome tools to identify palliative care needs. It is highly important that palliative education/training is available to healthcare professionals since oncologists and other healthcare professionals today have insufficient education in palliative care in many countries [104, 105]. Systematic symptom assessment in services providing basic palliative care may also help to identify and refer patients with the most complex palliative care needs early in the disease trajectory to specialized palliative care services [105, 106].
Strengths and limitations
The main strength in this study is that it included nationwide patient-reported symptoms/problems from basic and specialized palliative care services during a 1-year period, which enables comparison of patients’ symptomatology across settings. It is also a strength that the study includes cancer and non-cancer patients. Another strength is that all the need assessments (PRO questionnaires) completed at the start of palliative care in one of the 42 Danish specialized palliative care services during the study period were included in the study and that 12 sites providing basic palliative care (eight hospital departments, one research department, and three municipalities) were included. Overall, we believe the internal validity is high, although some limitations exist. First, convenience sampling was used to include patients from the 12 sites providing basic palliative care; thus, the patients are not necessarily representative for all Danish patients with life-threatening diseases outside specialized palliative care. Only in one of the sites providing basic palliative care was data collected on the proportion completing the PRO questionnaire, and in that hospital department, it was 75% (99 of 132 patients). The proportion of patients completing the PRO questionnaire at the start of specialized palliative care was 67%.
Some of the differences found, in this study, in symptomatology between patients in basic and specialized palliative care may be explained by differences in the proportion of inpatients and outpatients in the two settings as well as differences in prognosis. In specialized palliative care, 31% were inpatients and 69% were outpatients. We do not have the exact proportion of inpatients and outpatients in basic palliative care, but we know 39% were from outpatient services and 25% from inpatient services, whereas the remaining 36% were from services with a mix of inpatients and outpatients. Therefore, the proportion of outpatients could be from 39 to 75% (39% + 36%). It is also likely that the prognosis was better in basic palliative care compared to specialized palliative care; but unfortunately, information was not available at the individual level for patients in basic palliative care regarding in/outpatient status and prognosis. Another limitation is that EORTC QLQ-C15-PAL was developed for cancer patients, but the questionnaire does, however, seem to assess the most prevalent symptoms and problems experienced by cancer and non-cancer patients in palliative care [107, 108]. In addition, the EORTC QLQ-C15-PAL questions plus eight extra questions (included in the PRO-PALL questionnaire) were found easy to understand and relevant according to most of the 270 patients with cancer as well as other life-threatening illnesses [109]. Different factors may affect the generalizability of the findings in this study, such as the organization of palliative care in different countries.
Conclusions
Patients with life-threatening diseases admitted to specialized palliative care had a higher risk of symptoms and problems than patients receiving basic palliative care.
Future studies are needed to better understand changes in the level of symptoms/problems during the disease trajectory among patients with life-threatening diseases. This might help improve referral to specialized palliative care, especially for non-cancer patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO (2016) WHO Definition of Palliative Care [Available from: http://www.who.int/cancer/palliative/definition/en/. Accessed 4 Feb 2025
- 2EAPC (2013) Atlas of palliative care in Europe 2013 [Availible from: https://view.pagetiger.com/crmjfen/1. Accessed 4 Feb 2025
- 3COUNCIL OF EUROPE (2013) Recommendation Rec (2003) 24 of the Committee of Ministers to member states on the organisation of palliative care. COUNCIL OF EUROPE; 2003. pp 1–81. [Availible from: https://search.coe.int/cm?i=09000016805 de 857. Accessed 4 Feb 2025
- 4Hansen MB, Adsersen M, Groenvold M (2023) Anual report from the Danish Palliative Care Database 2022 [Dansk Palliativ Database: Årsrapport 2022]. [Availible from https://www.dmcgpal.dk//files/15_11_23_offentliggjort_aarsrapport_dpd_2022_med_3_reglen_18_12_23.pdf. Accessed 4 Feb 2025
- 5Rigsrevisonen (2020) Acces to specialized palliative care [Adgangen til specialiseret palliation]. København; 2020. [Availible from https://www.rigsrevisionen.dk/Media/637830383760074804/SR 1819.pdf. Accessed 4 Feb 2025
- 6WHO (2020) Palliative care: World Health Organization [updated August 5, 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/palliative-care. Accessed 4 Feb 2025
- 7Basic palliative care [Basal palliation]: the PRO Secretariat [PRO-sekretariatet]; 2023 [Available from: https://pro-danmark.dk/da/pro-emner/basal-palliation. Accessed 4 Feb 2025
- 8PRO-sekretariatet (2023) Final report for development of PRO for palliation [Afslutningsrapport for udvikling af PRO til palliation]. [Availible from https://admin.sundhedsdatastyrelsen.dk/Media/638653702307101758/Afslutningsrapport%20for%20udvikling%20af%20PRO%20til%20palliation.pdf. Accessed 4 Feb 2025