Connecting research and community: a methodological framework for investigating CMV transmission in childcare settings
Karen Del’Olio, Annie Geiger, Judith Terry, Cindi Callaghan, Lauren Howe, Cheryl Hamel, Delaney Platia, Alyssa Blake, Lisa Tran, Anne Davenport, Elizabeth Orvek, Stephen Lammi, Bruce Barton, Timothy Kowalik, John Holik, Anne Mirza, Olesea Cojohari, Kelsey Woods, Susan Druker

TL;DR
This study outlines a community-based approach to track CMV transmission in childcare settings, aiming to improve understanding of virus spread and immune responses.
Contribution
The novel contribution is a scalable, community-engaged methodological framework for studying CMV transmission in early education environments.
Findings
A geographically diverse EEC center network was established with culturally tailored recruitment strategies.
Protocols for saliva sample collection and optimized lab assays were developed to measure CMV shedding.
The framework supports future longitudinal studies on viral shedding, immune responses, and co-infections.
Abstract
The CMV Transmission and Immune Tracking (TransmIT) Study was developed to address critical gaps in understanding of cytomegalovirus (CMV) transmission dynamics in early education and care (EEC) settings. This two-stage, community-engaged study design integrates EEC center partnerships, digital study platforms, and data pipeline infrastructures to enable longitudinal virologic and immunologic surveillance in this high-exposure environment. Stage I focused on establishing foundational components of the study, including a geographically diverse EEC center network, culturally tailored recruitment strategies, a community advisory board, protocols for participant enrollment and saliva sample collection, and optimized laboratory assays to measure viral shedding in saliva. The study approach honed during Stage I is intended to support future longitudinal investigations into viral shedding…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
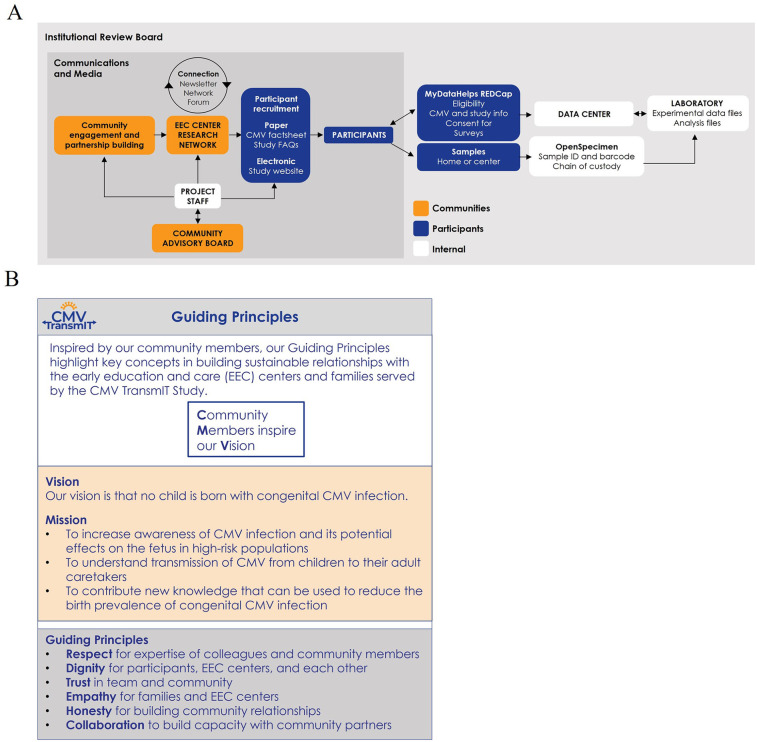 Figure 1
Figure 1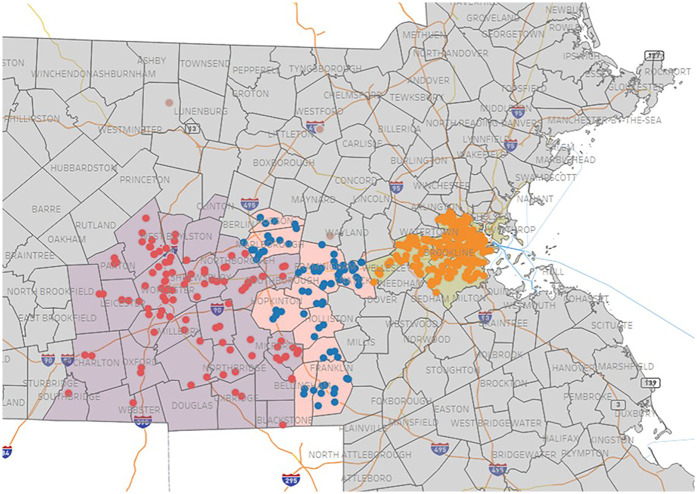 Figure 2
Figure 2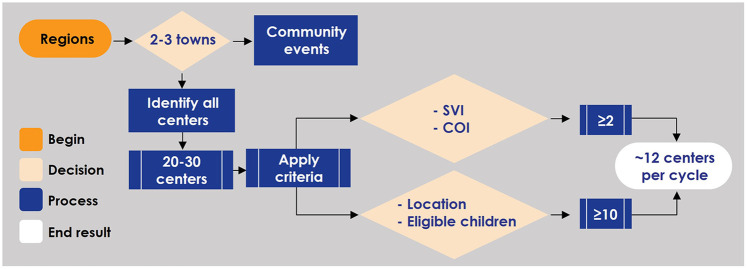 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6- —Moderna, Inc
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Herpesvirus Infections and Treatments · Parvovirus B19 Infection Studies
Introduction
1
Childcare centers provide essential services that support family and work life. However, any regular gathering of young children presents an opportunity for infectious diseases like conjunctivitis, respiratory infections, or gastroenteritis to circulate among children and their caretakers. A common pathogen in these settings is cytomegalovirus (CMV), a ubiquitous β-herpesvirus that infects people of all ages, especially children (1–3). CMV spreads via body fluids containing infectious virions, such as saliva and urine (4). Among children <3 years of age in childcare centers, the prevalence of CMV shedding in saliva or urine ranges from 10% to 70% (1). Moreover, high viral loads of CMV can continue to be shed well into early childhood up to 5 years of age (5), by which point about one-third of children in the United States have been infected (6). As a result, children attending large group programs are a major source of CMV transmission. Given their predictable exposure to saliva and urine of these children, caretakers at home or in childcare centers are at high risk for CMV exposure (7–18). If they are pregnant, CMV can disseminate to the fetus and lead to pregnancy loss or congenital CMV infection (cCMV) of live-born infants (8, 13, 16, 19–25).
CMV is not only the most common congenital infection worldwide, with a birth prevalence of 0.6%–0.7% (approximately 1 in 200 infants) in developed countries and 1%–5% in developing countries (26, 27), but also the leading infectious cause of birth defects and non-genetic cause of hearing loss (28, 29). An estimated 10%–15% of infants with CMV infection have clinically apparent symptoms at birth, such as microcephaly, hepatosplenomegaly, or cytopenias (30). Of the remainder born without visible symptoms, about 10%–15% will develop complications later in childhood, most commonly hearing loss but also neurodevelopmental delays (26, 27, 31–33). Nearly 20% of all infants with cCMV infection develop permanent long term effects (34). Despite the significant familial and societal burden of disease, awareness of cCMV is low (26, 29, 33, 35–39). Global surveys with data up to 2020 suggest that <7% of adults and <40% of pregnant women have heard of CMV (40–42). Furthermore, CMV transmission patterns and mechanisms of viral control in childcare settings remain poorly understood, limiting the development of educational materials and interventions to reduce cCMV prevalence (43).
The CMV Transmission and Immune Tracking (TransmIT) Study was developed to address gaps in understanding of CMV transmission in early education and care settings by establishing a research network through structured community engagement (44–49), integration of digital study platforms, and standardized laboratory methodologies (50–53). Our approach provides a scalable model for studying virologic and immunologic factors driving CMV shedding and transmission. This report details the methodology used in the early stages of the CMV TransmIT Study, with the potential to inform policy, clinical practice, and public health interventions for CMV and other infectious diseases.
Methods
2
Overall study design
2.1
In the absence of recent or local community-based studies in childcare centers, the CMV Transmission and Immune Tracking (TransmIT) Study was structured to progress in two stages. The initial stage was designed to establish key operational resources to support both long-term sustainability and future expansion to more complex studies and additional pathogens in this high-transmission setting.
Stage I focused on assembling a foundational infrastructure and building community relationships. Objectives included refining center and participant recruitment strategies, developing study materials, securing institutional review board (IRB) approvals, establishing data storage and flow processes, validating sample collection and experimental protocols, and addressing unique challenges in childcare settings for example, identifying appropriate, low-disruption areas within centers for sample collection or navigating variable pickup/drop-off times that complicated scheduling with families. By devising a relatively simple study protocol, Stage I not only allowed for iterative trials and refinement of critical workflows, but also enabled center staff and families to become familiar with the study team and the research process.
Stage II will expand on these activities through a longitudinal study that tracks CMV transmission dynamics and co-circulation with other pathogens. Initial aims are to characterize intra- and inter-host CMV populations, assess immune responses, and identify parameters associated with reduced CMV shedding over time. A platform study design will facilitate inclusion of other pathogens and co-infections commonly encountered in childcare settings, such as respiratory viruses.
This two-stage approach ensures that operational and methodological challenges and inefficiencies are optimized in a controlled manner during Stage I before launching more complex studies in Stage II. This method provides a replicable and scalable framework for investigating diverse infectious agents in group childcare environments and makes the work broadly applicable to public health research. The components and guiding principles of Stage I are summarized in Figure 1.
Components and guiding principles of stage I of the CMV transmIT study. (A) Conceptual flow and relationships between key components in the study. (B) The principles guiding the activities of the study. CMV, cytomegalovirus; EEC, early education and care; FAQs, frequently asked questions; ID, identifier; TransmIT, transmission and immune tracking.
Community engagement and advisory structures
2.2
Community advisory board
2.2.1
A Community Advisory Board was established to ensure that study activities aligned with community values and priorities. In consultation with the UMass Chan Medical School Community Engagement and Collaboration Core, a three-phase board member recruitment plan was implemented (Supplementary Appendixes 1A–C). The Board's objectives were to (1) advise on research design and implementation to enhance trust and acceptance, (2) ensure that protocols and materials respect community norms and traditions, (3) facilitate engagement and communication between the study team and community members, and (4) help maintain and expand community networks. The Board input also guided modifications to educational content, risk communication, and cultural considerations. These and other roles of the Board were detailed in its mission and charter (Supplementary Appendix 1D).
Diversity, equity, and inclusion
2.2.2
The CMV TransmIT Study team viewed diversity, equity, and inclusion as fundamental elements of community engagement efforts. Given that culture, language, and socioeconomic context varied widely among early education and care (EEC) centers, education and recruitment materials were developed with consideration for health literacy, linguistic accessibility, and cultural values. For example, to support participation among Spanish-speaking families, selected study materials, including social media content, educational materials, and enrollment instructions were translated into Spanish. Board and local stakeholders were engaged to ensure that study processes respected community traditions and anticipated potential concerns. For example, feedback from center directors indicated that the preferred professional terminology in Massachusetts is “early education and care” rather than “daycare” or “childcare,” reflecting both the educational and caregiving missions of these institutions. By prioritizing equitable participation and fostering an atmosphere of mutual respect, we aimed to build a more inclusive research environment—one that could ultimately strengthen trust, broaden engagement, and maximize the relevance and applicability of study findings for all communities.
Early education and care (EEC) center network
2.3
At the onset of planning in 2018, a comprehensive search of the Massachusetts Department of Early Education and Care (MA DEEC) online directory identified 247 licensed large-group centers serving infants, toddlers, and preschoolers in the Worcester (n = 107) and Cambridge (n = 140) areas (52). From this pool, the study aimed to recruit approximately 20 public or private, non–home-based centers (about 10 per region). Early data collection included center characteristics such as maximum classroom size by age group (7 children for infants aged <15 months, 9 for toddlers aged 15–33 months, and 10 for preschoolers aged 33 months–pre-kindergarten (54) and infection control protocols. To strengthen center recruitment, community engagement experts with experience in education-based research were consulted to provide best practices and training for the study team.
The primary objective was to develop a sustainable EEC center research network emphasizing collaborative partnerships and minimizing operational burden on participating sites. Initial recruitment efforts were guided mainly by convenience factors, such as existing professional contacts, proximity to the study institution, and access to organizational networks linking multiple centers. An outreach database was developed in Research Electronic Data Capture (REDCap) (55, 56), integrating data from the Massachusetts Department of Early Education and Care (MA DEEC) directory and tracking real-time progress in center recruitment. As network expansion progressed, it became clear that relying exclusively on convenience-based strategies was insufficient to achieve a diverse and representative sample of centers and families. To address this, the sampling frame was expanded by grouping eastern Massachusetts into three broad regions—Worcester, MetroWest, and Cambridge/Boston (Figure 2). Centers were then identified for outreach based on travel feasibility for field teams and the number of children eligible for study enrollment. To avoid a bias toward better-resourced areas, the Collaboration Opportunities in Research Engagement (CORE) approach was developed to intentionally engage communities less likely to have access to, familiarity with, or participation in research. Despite some overlap in the underlying datasets, a pilot approach using Social Vulnerability Index (SVI) (57) and Child Opportunity Index (COI) data was used to identify and prioritize additional centers during outreach cycles. In the revised model (Figure 3), each outreach cycle involved contacting approximately 12–14 centers selected based on travel feasibility, enrollment potential, and, for at least 20% of centers, suboptimal SVI and COI metrics despite not meeting other eligibility criteria. This strategy also included collaboration with trusted community voices, participation in local cultural events and public forums, the delivery of accessible CMV education, and additional activities to cultivate authenticity, foster trust, and encourage meaningful participation across a wide range of communities in the CMV TransmIT Study.
Regions and centers in Massachusetts included for recruitment for the CMV transmIT study. EEC centers in the Worcester (red), MetroWest (blue), and Cambridge/Boston (orange) regions were approached during recruitment to participate in the study. CMV, cytomegalovirus; EEC, early education and care; TransmIT, transmission and immune tracking.
Center outreach strategy. EEC centers were identified for outreach based on the travel feasibility for field teams and the number of eligible children. Least resourced areas were intentionally identified and engaged based on SVI and COI data. COI, child opportunity index; EEC, early education and care; SVI, social vulnerability index.
Data management and infrastructure
2.4
Given trends toward real-time data collection (58) and to minimize barriers for participants such as paper documents or travel, digital study platforms were developed. MyDataHelps (MDH), created by CareEvolution, provided a website format to streamline the user experience of enrolling children and facilitate a low-friction onboarding mechanism for parents without the need to download an application or create an account (Supplementary Appendix 2). In addition to public-facing materials, a prominent “call-to-action” was included on the website home page to encourage visitors to connect with the study. Further exploration let parents view CMV and study information, determine eligibility, provide consent, validate relevant information, follow step-by-step instructions, and access on-site visit and sample collection schedules for their specific center. Home addresses were validated through the platform and identity of the child via parents or center staff. Links to surveys and other information were provided via email and/or mobile phone text message. Similarly, REDCap (55, 56) provided a straightforward platform for center staff to enroll and perform study activities. Contact information was displayed prominently on these platforms and other study materials to encourage communication with study staff. Overall, content required not only accessible language but also formatting, graphic design, and cohesiveness for an inviting experience.
Without an existing study infrastructure, conducting a needs assessment was essential to formulating the data management plan. The assessment considered security, access, format, storage, quality control, and data pipeline needs from all sources-to-storage. Given the relatively low sensitivity of data extracted from sources and moved through the system (i.e., very limited protected health information and personal identifiable information), data security was less of a concern, so the initial design focused on efficiency and scalability. The strategy included flexible evolution across both stages of the project, starting with data collected at one time point and preparing for subsequent longitudinal data collection at multiple time points. Successfully integrating data from multiple sources (e.g., MDH for children and REDCap for center staff, sample chain-of-custody and management platforms, and laboratory experiments) required careful planning to ensure consistent exports and accurate data linkage. The data management plan also included strict quality control measures to ensure data accuracy through pipelines and into analytical activities. The final solution was not only effective and flexible enough for evolving data collection, but also reliable and efficient enough for real-time analysis. A dashboard was created for easily viewing key study components (Figure 4).
Study dashboard. Certain metrics are shown as examples for the (A) enrollment, (B) participants, (C) viral load, and (D) viral culture facets of the study dashboard. CMV, cytomegalovirus; dPCR, digital polymerase chain reaction; GSA, Guild of St Agnes; YWCA, Young Women's Christian Association.
Communications and media strategy
2.5
With the objective to increase CMV awareness and intention to disseminate study findings, we created multiple public access points. Communication and media strategies were developed in collaboration with the parent institution, funding sponsor, and public relations experts to align with best practices for branding, media engagement, and social responsibility (Supplementary Appendix 3). When appropriate, output was circulated for feedback and vetted with relevant UMass Chan Medical School and sponsor stakeholders prior to release. A logo, graphic, and other branding features were created to promote recognition (Figure 5). The study website was created not only for participant enrollment but also for public education about CMV. Other mechanisms included local and wire press releases, podcasts, monthly blogs, media briefings and pitches, thought leadership articles, and social media posts distributed through various channels. Training was provided for study personnel to ensure clear and consistent messaging to the media and public. Future efforts are planned to evaluate public engagement with these communication tools as part of future study activities.
The CMV transmIT study logo (A) and graphic (B) the CMV transmIT study logo and graphic were among the branding features designed to promote recognition of the study and for use on electronic and printed materials. CMV, cytomegalovirus; TransmIT, transmission and immune tracking.
Ethics considerations and IRB approval
2.6
The CMV TransmIT Study protocol and materials were developed per U.S. Department of Health and Human Services regulations for human subjects research (45 CFR 46) (54) and approved by the UMass Chan Medical School Institutional Review Board (IRB). Investigators, IRB staff, and study team members collaborated on iterative development of the Investigator Study Plan and informed consent form. Participant-facing materials were prepared in plain language (59) with attention to health literacy (60) and U.S. Centers for Disease Controls and Prevention health equity guidelines (60). Input from a National Institutes of Health Department of Bioethics representative guided decisions on reporting CMV polymerase chain reaction (PCR) results to participants. Consistent with that guidance, parents received education about CMV but did not receive results of saliva CMV PCR. CMV education highlighted that viral shedding in saliva is common in young children and that a positive PCR test would not change their usual healthcare or ability to continue at their center. Parents were also advised to contact their pediatrician for questions about CMV and their child specifically.
EEC center orientation and ongoing engagement
2.7
Our partnership with centers that joined the network began with an orientation meeting involving center directors and the study team (principal investigator, program manager, administrative coordinator, and research nurse; Figure 6). The conversation yielded a study operations plan customized to each center and a signed description of our collaboration to document roles and align expectations (Supplementary Appendix 4). The plan balanced IRB-approved activities with director preferences on study visit schedules, areas for meeting families and collecting samples, and other center-specific decisions. CMV education sessions for center staff and for families were provided in the format (in-person or virtual) or time (day or evening) requested by directors, thus aligning study activities with centers' familiar routines. Directors completed a survey on center demographics and practices (Supplementary Appendix 5). To provide benefit and build relationships with and among centers in the network, for center staff and families, we offered CMV education and access to the principal investigator for scientific questions, check-in and feedback sessions, annual gift cards, quarterly newsletters (Supplementary Appendix 6), group forums to provide study updates and share findings, and other appreciation efforts.
Workflow for orientation and engagement with EEC centers. Steps following center enrollment included director meetings, staff and family education, scheduled check-ins, and ongoing engagement activities to support study implementation. EEC, early education and care.
Participant recruitment and enrollment
2.8
Recruitment materials focused on CMV and study information and identified staff presence at centers (Supplementary Appendix 7). Study enrollment for Stage 1 was first limited to children <36 months of age attending EEC centers in the research network. Enrollment was later expanded to also include any staff member working at least 5 weeks per year, regardless of their role (56) with the primary goal of piloting staff participation procedures in anticipation for Stage II. Lack of exclusion criteria maintained inclusivity. The enrollment period was 4 weeks per participant to accommodate CMV education sessions, the informed consent process, demographic survey completion (Supplementary Appendix 8), and saliva sample collection. The Stage I enrollment goal was approximately five children per center at 20 centers (100 children total) and at least five staff members each at two centers (10 staff total), balancing representativeness and feasibility. Families were invited to share feedback and attend focus groups whether or not their child participated in the study (Supplementary Appendix 9).
Sample collection and laboratory procedures
2.9
A unique identification system for participants and samples (Supplementary Appendix 10) was designed to adapt to both stages of the project. The selection of saliva collection devices—Micro•SAL™ for children (later modified to include a volume indicator) and Super•SAL2™ for adults—was based on predefined criteria (Supplementary Appendix 11). One saliva sample per participant was collected either on-site by study staff or through a pilot home collection option. The pilot evaluated feasibility, logistics, and acceptability of home sample collection, planned enrollment of at least 15 children and 15 EEC center staff (no more than 60 total) and included participant feedback on home sampling safety and experience (Supplementary Appendixes 12–S13). Results from the pilot will inform Stage II sample collection procedures.
All saliva samples underwent standardized workflows for receipt, processing, and storage. Digital PCR (dPCR) assays were optimized to measure the absolute number of CMV DNA molecules per sample, which defined CMV shedding prevalence at each center. A CMV DNA standard was used to determine the limit of detection (LOD) for the dPCR assay. Results were expressed in copies/ml rather than IU/ml, as the assay was optimized for research use only and not intended as a clinical diagnostic. A viral infectivity assay was developed to quantify the level of infectious CMV in each sample and test viral tropism for fibroblast and/or epithelial cells. Known viral stocks were used to determine the LOD of this assay.
Anticipated results
3
The staged approach of CMV TransmIT is expected to yield a range of informative outcomes. Stage I will establish a robust research network and demonstrate the feasibility of recruiting participants and collecting saliva samples in the EEC setting. Evolving center outreach and community engagement activities, guided by established principles, the CORE center outreach strategy, and input from the Community Advisory Board, are intended to provide CMV education to people capable of becoming pregnant, increase access to research in general, and strengthen trust within EEC centers and their surrounding communities. Such fundamental efforts increase the probability, quality, and sustainability of partnerships with individual centers and their consortium that can lead to mutually beneficial interactions and increasing enrollment and retention rates.
The integration of MDH and REDCap platforms is anticipated to streamline participant onboarding, facilitate reliable data linkage, and enable real-time monitoring of enrollment, sample collection, and key laboratory data. Measurements of CMV in saliva obtained through digital PCR and viral infectivity assays are expected to demonstrate that children under 3 years of age in large-group early education programs frequently shed CMV in saliva and may serve as sources of infection for individuals who are pregnant.
In the longer term, the foundational structure and data from Stage I are expected to inform the design and implementation of more complex, longitudinal studies in Stage II. Learnings from Stage I will enhance operational efficiency and support the development of new collaborations with centers and other partners. Expanding study staff presence at centers and within their local communities is anticipated to improve familiarity and possibly reduce discomfort with research participation. Additionally, targeted participant enrollment strategies, refined sampling procedures, and validated laboratory methods will strengthen future study designs and enable robust hypothesis testing. Stage II will also expand investigation to include other pathogens relevant to early education and care settings, ultimately guiding a more comprehensive understanding of viral transmission patterns and immune responses.
Discussion
4
The CMV TransmIT Study was designed to address critical gaps in understanding of CMV transmission dynamics in EEC settings. Multiple studies have suggested that children under 3 years of age are a major source of infectious virus for pregnant caretakers and may therefore be an effective target population for a CMV vaccine (61, 62). The central premise of the study is that reducing CMV spread from young children to people who are pregnant will ultimately decrease the birth prevalence of cCMV. The path to achieving this goal is complicated by limited public awareness, incomplete knowledge of CMV natural history in childcare contexts, and the operational complexities of community-based research (63). To begin navigating these issues, a two-stage study was implemented that first focused on community engagement, key infrastructure components, and laboratory methodologies. From the outset, community engagement was integral to building local capacity and ensuring that the research reflected community values and priorities (57). Stakeholders were consulted to understand the current EEC landscape, engaged a Community Advisory Board with varied expertise, and incorporated principles of diversity, equity, and inclusion into participant-facing materials (58). Center-specific onboarding processes were tailored to the unique context and prior research experience of each community, promoting shared decision-making and fostering early trust. Engagement with families, staff, and local communities contributed to the establishment of an expanding research network of EEC centers. Concurrently, the development of internal staffing, technological systems, and laboratory workflows necessitated the creation of a multidimensional research infrastructure.
The study began with a relatively simple protocol—a brief survey and a single saliva sample—to introduce the research process in a non-intrusive manner and to demonstrate the feasibility of conducting research in EEC centers. Collecting one sample per participant provided sufficient volume while maintaining a manageable pace for developing essential biosafety, experimental, and data workflows.
The CMV TransmIT Study model offers many key advantages. While seemingly less efficient, the staged approach provided time for essential research components—community partnership and infrastructure development—to evolve gradually and sustainably. Building meaningful, trust-based relationships with centers required substantial time and nuanced understanding of their cultural, geographic, and familial contexts. The community-driven engagement and pace offered contextual insights that will enhance the relevance and impact of findings and future studies. Tailoring operations plans for each center allowed their leaders to guide implementation, thus reducing apprehension and ensuring that study activities accommodated their norms and routines. The scalable digital infrastructure supported efficient data collection, management, and quality assurance. Overall, we envision the study model will serve as an adaptable platform for investigating other infectious diseases and research questions in EEC settings.
As intended for this early stage, several insights emerged that required ongoing refinement of our approach or that arose from the nature of the EEC center setting. Real-time process improvement cycles (59) guided by study team insights and by feedback from participating centers or the Board were implemented frequently. Most significantly, a detailed understanding of certain communities prompted adoption of the CORE outreach strategy to more intentionally include sites with limited access to or familiarity with research, thereby enhancing inclusivity and relevance of the study for families utilizing EEC services. Similarly, we learned that integration of study staff with routine center activities during site visits—not only for participant recruitment but also for offering general support as needed—was instrumental in building trust and engagement. We discovered that familiarity with CMV among center staff and families was generally low, potentially reducing understanding and perceived relevance of the project. The resource intensive study approach, geographic constraints and in-person sample collection may have restricted center, family, or staff participation. The initial simplicity of the study protocol, while valuable for feasibility assessments, may only partially capture the complexities of CMV transmission patterns and immune responses. Outside of the study, many EEC centers faced operational demands on their attention and resources preventing or limiting their engagement in research. Given these intrinsic challenges, the primary obstacle to future studies will probably be low center or participant recruitment and retention. Some tactics to counteract this issue include increasing community engagement through collaborations with other researchers, existing resources, and local community leaders.
With Stage I completed, a versatile research infrastructure has been established, and the EEC center research network continues to expand. These efforts have yielded valuable insights into effective study implementation and have strengthened the network's readiness for more complex, longitudinal investigations. Lessons learned—from community engagement strategies to data and laboratory workflows—will guide future CMV transmission and immunity research in Stage II. Beyond CMV, the collaborative relationships formed with EEC centers provide a platform for investigating other infectious diseases of public health relevance. Leveraging this network, future studies may deploy new protocols, evaluate interventions, and generate evidence to inform policies and clinical practices aimed at improving child and community health. Importantly, Stage I underscored that research in community settings advances at the speed of trust (60) and depends on respect for local priorities and an adaptable mindset. These principles will continue to guide the evolution of the CMV TransmIT Study and inform its broader application to research on CMV and other pathogens.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Collins JP Shane A. Infections associated with group childcare. In: Principles and Practice of Pediatric Infectious Diseases. 5th ed. Philadelphia, PA: Elsevier (2018) 25-32:e 3.
- 2Gupta M Shorman M. Cytomegalovirus. In: Stat Pearls. Treasure Island, FL (2024).
- 3Centers for Disease Control and Prevention. Clinical Overview. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (2022). Available online at: https://www.cdc.gov/cmv/clinical/overview.html (Accessed May 8, 2024).
- 4Centers for Disease Control and Prevention. About Cytomegalovirus (CMV). Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (2020). Available online at: https://www.cdc.gov/cmv/overview.html (August 18, 2023).
- 5Cannon MJ Hyde TB Schmid DS. Review of cytomegalovirus shedding in bodily fluids and relevance to congenital cytomegalovirus infection. Rev Med Virol. (2011) 21(4):240–55. 10.1002/rmv.69521674676 PMC 4494736 · doi ↗ · pubmed ↗
- 6Centers for Disease Control and Prevention. Cytomegalovirus (CMV) and Congenital CMV Infection—Clinical Overview. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (2020). Available online at: https://www.cdc.gov/cmv/clinical/overview.html (Accessed October 26, 2023).
- 7Pass RF Hutto C Ricks R Cloud GA. Increased rate of cytomegalovirus infection among parents of children attending day-care centers. N Engl J Med. (1986) 314:1414–8. 10.1056/NEJM 1986052931422043010113 · doi ↗ · pubmed ↗
- 8Alain S Garnier-Geoffroy F Labrunie A MontanéA Marin B Gatet M Cytomegalovirus (CMV) shedding in French day-care centers: a nationwide study of epidemiology, risk factors, centers’ practices, and parents’ awareness of CMV. J Pediatr Infect Dis Soc. (2020) 9(6):686–94. 10.1093/jpids/piz 09732068854 · doi ↗ · pubmed ↗