Subnipple Cyst Formation Is an Important Diagnostic Clue for Mixed-Type Squamous Cell Carcinomas of the Breast: A Case Report
Togo Matsushima, Shoji Oura

TL;DR
A breast tumor with a subnipple cyst and adjacent solid mass may indicate a mixed-type squamous cell carcinoma, which is important for accurate diagnosis.
Contribution
This case report highlights subnipple cyst formation as a diagnostic clue for mixed-type breast SCCs.
Findings
The tumor had a subnipple cyst connected to a solid mass with features of scirrhous-type IDC and SCC.
Immunostaining showed HER2 negativity in IDC and equivocality in SCC components, with no HER2 amplification confirmed.
The patient had a successful outcome with surgery and chemotherapy, emphasizing the importance of early diagnosis.
Abstract
It is well known that breast squamous cell carcinomas (SCCs) have highly cystic components. It, however, is not yet known whether the location of cystic areas contributes to the diagnosis of breast SCCs. A 62-year-old woman with a right breast mass was referred to our hospital. Mammography showed an oval mass just under the right nipple and distortion of the adjacent mammary gland with pleomorphic calcifications. Ultrasound showed a subnipple large oval cystic lesion with solid parts, microcalcifications, and an adjacent polygonal mass, both with a high depth/width ratio and internal punctuate high echoes. Magnetic resonance imaging (MRI) of the masses clarified the connection between the two masses at their deep borders and showed low signals on T1-weighted images and high and slightly high signals at the cyst and mass parts on T2-weighted images, respectively. Core needle biopsy of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
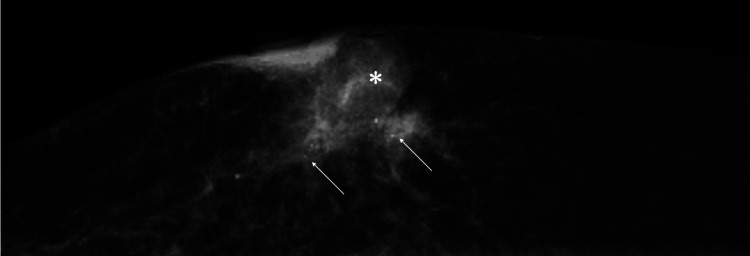 Figure 1
Figure 1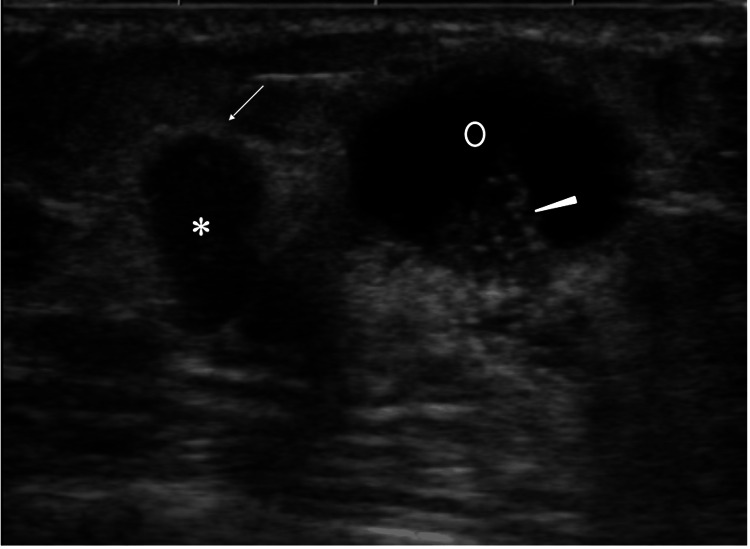 Figure 2
Figure 2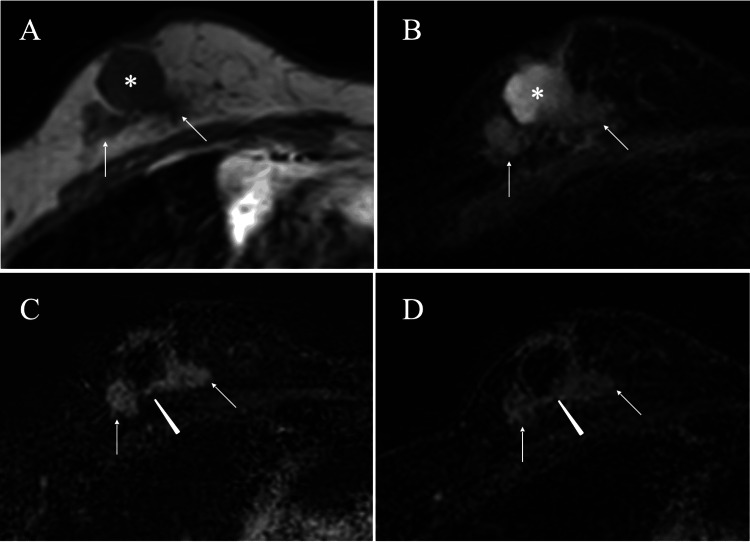 Figure 3
Figure 3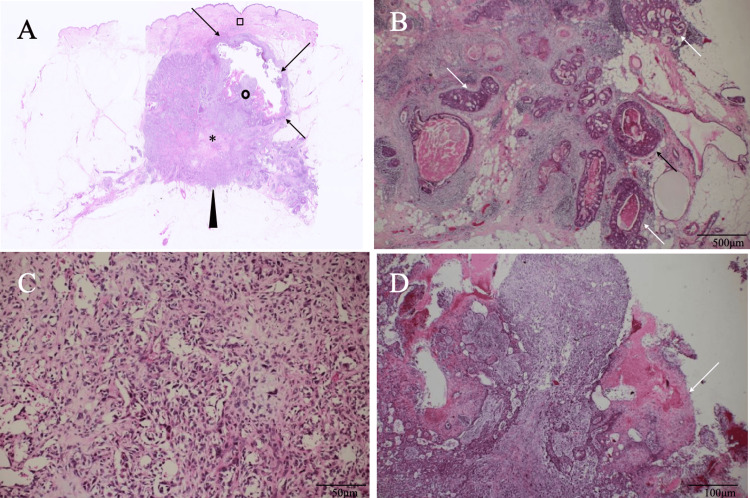 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Breast Lesions and Carcinomas · Breast Cancer Treatment Studies
Introduction
The mammary gland is a glandular tissue, which therefore makes breast carcinomas overwhelmingly adenocarcinomas. The mammary gland, however, can extremely rarely develop squamous cell carcinomas (SCCs), one phenotype of metaplastic carcinomas [1]. SCCs are classified into pure and mixed subtypes. The former has more than 90% SCC components, and the latter has predominant SCC components and more than 10% of invasive ductal carcinoma (IDC) components. Although many breast cancers are sensitive to chemotherapy, breast SCCs hardly respond to any type of systemic therapies [2,3]. Quite a few oncologists, therefore, have experienced great difficulty when treating metastatic breast SCCs.
In the past three decades, operable breast cancers have often come to be treated not with primary surgery but with neoadjuvant chemotherapy (NAC), based both on their biology [4-6] and patients’ preference for breast conservation. Breast SCCs are basically triple-negative breast cancers [2,3] and, especially in mixed-type SCCs, can be improperly treated with NAC because of the frequent diagnosis of estrogen receptor-negative IDC by the pathological evaluation of core needle biopsy specimens.
It is well known that approximately half of breast SCCs have cystic components within them due to their aggressive nature them. Therefore, the presence of cystic components can contribute to the diagnosis of breast SCCs to some extent. No studies, however, have clarified where cystic areas occur within SCCs and how the location of cystic areas contributes to the diagnosis of SCCs.
We herein report a breast SCC case with cystic components just under the nipple, which highly suggests that subnipple cyst formation is an important diagnostic clue for mixed-type breast SCCs.
Case presentation
A 62-year-old woman without any prior breast symptoms or a history of screening mammography evaluation, noticed a breast mass and was referred to our hospital due to her right breast mass. Mammography showed an oval mass just under the right nipple and distortion of the adjacent mammary gland with pleomorphic calcifications (Figure 1).
Mammography FindingsMediolateral oblique view mammography showed a sub nipple mass (asterisk) and distortion of the adjacent mammary gland (arrows) with microcalcifications.
Ultrasound showed a polygonal mass with a high depth/width ratio and internal punctate high echoes and an adjacent subnipple large oval cystic lesion, which had solid parts with microcalcifications (Figure 2).
Ultrasound FindingsUltrasound showed a high depth/width ratio mass (asterisk) both with haloes (arrow) and internal punctuate high echoes, and a mixed cystic (open circle) and solid (arrowhead) mass in the nipple direction with microcalcifications in its solid parts.
Magnetic resonance imaging (MRI) of the masses showed a maximum size of 3.5 cm, low signals on T1-weighted images, and high and slightly high signals at the cyst and mass parts on T2-weighted images, respectively. In addition, time-signal intensity images showed weak early and retained enhancement up to the late phase, and clarified the connection between the two masses at their deep borders (Figure 3).
Magnetic Resonance Imaging (MRI) FindingsMRI of the solid parts in the two masses showed low signals on T1-weighted images (A, arrows) and weak high signals on T2-weighted images (B, arrows). MRI of the cystic parts showed low signals on T1-weighted images (A, asterisk) and high signals on T2-weighted images (B, asterisk). Time-signal intensity images showed early enhancement on early phase images (C, arrows), retained weak enhancement on late phase images (D, arrows), and connection of the two masses at their deep borders (C and D, arrowhead).
These imaging findings made us do the core needle biopsy of the solid breast mass under the tentative diagnosis of breast cancer. Pathological study showed atypical cells growing in tubular and cord-like fashions with connective tissue proliferation and focal microcalcifications, leading to the diagnosis of scirrhous type IDC. Immunostaining of cancer cells showed estrogen and progesterone receptor negativity, human epidermal growth factor receptor type 2 (HER2) equivocality, and a high Ki-67 labelling index of 30%. The patient, therefore, underwent mastectomy and sentinel node biopsy, showing pathological node negativity on frozen section. Postoperative pathological study showed that the scirrhous type IDC cells were connected to pleomorphic spindle cells and further tied up to SCC cells containing central cystic structures (Figure 4).
Pathological findingsA) Low magnified view showed a mixed cystic mass (arrows) with solid parts (open circle) just beneath the nipple (open square) and an adjacent solid mass (arrowhead) with abundant fibrous components (asterisk). B) Magnified view of the solid mass showed atypical cells growing in a cribriform fashion (arrows). C) Spindle cells with sarcomatoid features intervened between the cystic and invasive ductal carcinoma areas. D) Solid parts in the intracystic mass had squamous cell carcinoma cells with keratinization (arrow).
Immunostaining showed HER2 negativity in the IDC components and equivocality in the SCC components. Thereafter, fluorescence in situ hybridization clarified no amplification of HER2 genes in the SCC components. The patient recovered uneventfully, was discharged on the seventh day after the operation, received dose-dense chemotherapy consisting of four cycles of epirubicin and cyclophosphamide followed by four cycles of paclitaxel, and is scheduled for long-term follow-up on an outpatient basis.
Discussion
Various breast disorders can have cystic structures just beneath the nipple: intraductal papillomas, nipple adenomas, malignant phyllodes tumors, and non-invasive/IDCs growing in tubule-forming fashions [7,8]. Among these diseases, only (non-) IDCs can have microcalcifications in and around the cystic walls. MRI and ultrasound findings, therefore, made us speculate that IDCs had caused both internal punctate high echoes in the solid mass and cyst formation under the nipple. We further speculated that, probably due to the tumor heterogeneity, fibrous components present among IDC cells led to the formation of the high depth/width ratio solid mass [9].
When evaluating mixed cystic and solid breast lesions, it is naturally imperative for diagnostic physicians to obtain biopsy samples from the solid areas, which generally harbor more important pathologic elements. We, therefore, performed a core needle biopsy of the solid mass and obtained pathological information of IDC cells with estrogen receptor negativity, a high value of Ki-67 labelling index, and HER2 equivocality. It is well known that estrogen receptor (ER)-negative IDCs, regardless of HER2 status, show higher pathological complete response rates to NAC than ER-positive IDCs [10]. We, therefore, might have applied NAC to the patient if the patient had strongly requested us to treat her breast cancer with breast-conserving therapy. Breast SCCs, however, hardly respond to any type of chemotherapy and generally show progression when treated with NAC under the tentative diagnosis of ER-negative IDC.
The vast majority of tubule-forming IDCs with cystic structures can spread beyond the cystic walls, but hardly form a solid mass with abundant fibrous components [7]. Conversely, solid-type IDCs can often have ductal spread predominantly toward the nipple direction, but extremely rarely have cyst-forming type ductal spread. In short, by considering the relative positions among the solid mass, cystic parts, and the nipple, we could have negated both intracystic breast cancer with peripheral solid type invasion and solid type IDCs with cyst-forming type ductal spread toward the nipple.
It is well known that pulmonary SCCs often present cavitation due to both central necrosis and subsequent subclinical expectoration of necrotic debris via the bronchi [11]. Breast SCCs grow similarly and often have cystic components due to central necrosis. In hindsight, we should have speculated that breast cancers with both subnipple cystic parts and adjacent IDC parts could present with imaging findings similar to those observed in this case. In any case, when diagnosing an intracystic tumor just beneath the nipple and an adjacent solid tumor, diagnostic physicians need to keep in mind the possibility of mixed-type SCCs.
Conclusions
Mixed-type SCCs can have cystic structures just beneath the nipple. Diagnostic physicians, therefore, should take mixed-type breast SCCs into mind when breast tumors have cystic structures just under the nipple and an adjacent solid mass. In addition, even if breast cancer with these structures is diagnosed as an ER-negative IDC, oncologists should be cautious about applying NAC to it.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Management and prognosis of pure primary squamous cell carcinoma of the breast J Gynecol Obstet Hum Reprod Benoist P Mureau A Joueidi Y 2752804720182995908610.1016/j.jogoh.2018.06.007 · doi ↗ · pubmed ↗
- 2Squamous cell carcinoma of the breast J Clin Oncol Hennessy BT Krishnamurthy S Giordano S 782778352320051625808510.1200/JCO.2004.00.9589 · doi ↗ · pubmed ↗
- 3Squamous cell carcinoma of the breast: clinico-pathologic implications and outcome Eur J Surg Oncol Behranwala KA Nasiri N Abdullah N Trott PA Gui GP 3863892920031271129510.1053/ejso.2002.1422 · doi ↗ · pubmed ↗
- 4Neoadjuvant versus adjuvant chemotherapy in premenopausal patients with tumours considered too large for breast conserving surgery: preliminary results of a randomised trial: S 6Eur J Cancer Scholl SM Fourquet A Asselain B 64565230199410.1016/0959-8049(94)90537-18080680 · doi ↗ · pubmed ↗
- 5Preoperative chemotherapy in primary operable breast cancer: results from the European Organization for Research and Treatment of Cancer trial 10902 J Clin Oncol van der Hage JA van de Velde CJ Julien JP Tubiana-Hulin M Vandervelden C Duchateau L 422442371920011170956610.1200/JCO.2001.19.22.4224 · doi ↗ · pubmed ↗
- 6Neoadjuvant versus adjuvant systemic treatment in breast cancer: a meta-analysis J Natl Cancer Inst Mauri D Pavlidis N Ioannidis JP 1881949720051568736110.1093/jnci/dji 021 · doi ↗ · pubmed ↗
- 7Ductal abnormalities as primary findings on breast ultrasonography: a literature review and proposed classification Ultrasonography Oba K Tsunoda H Moon WK 2452594420254053416410.14366/usg.25048 PMC 12242359 · doi ↗ · pubmed ↗
- 8A case of giant nipple adenoma Surg Case Rep Ono S Tanaka M Yoshinaga Y Satou T Aoki M 701020243852668510.1186/s 40792-024-01869-y PMC 10963697 · doi ↗ · pubmed ↗