Endoscopic ultrasound-guided coil and Histoacryl therapy of varices at the hepaticojejunostomy
Thomas Roland Heiduk, André Sasse, Giovanni Federico Torsello, Ali Seif Amir Hosseini, Volker Ellenrieder, Golo Petzold, Ahmad Amanzada

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
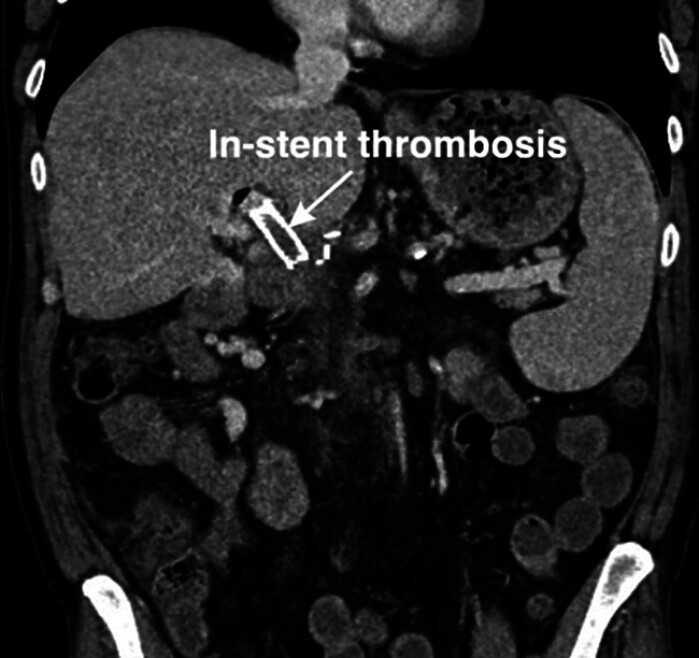 Fig. 1
Fig. 1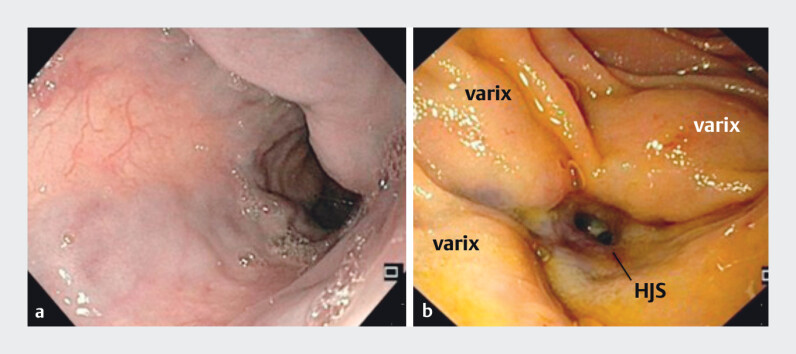 Fig. 2
Fig. 2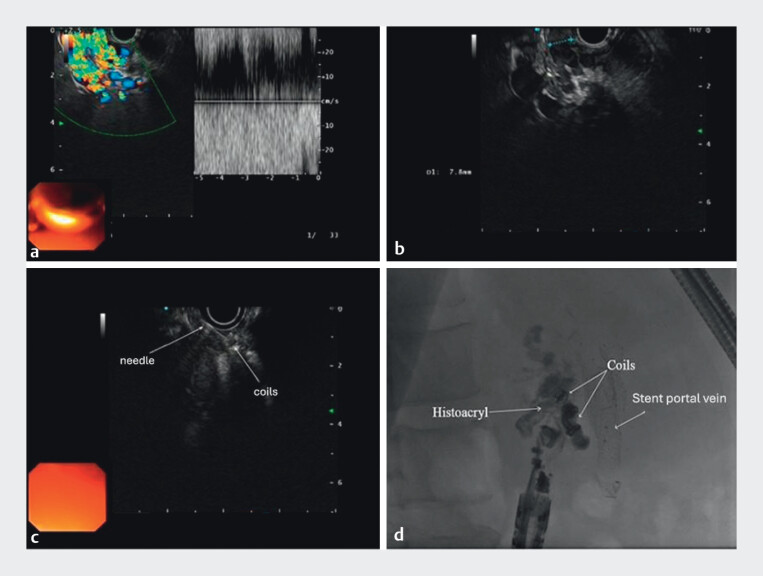 Fig. 3
Fig. 3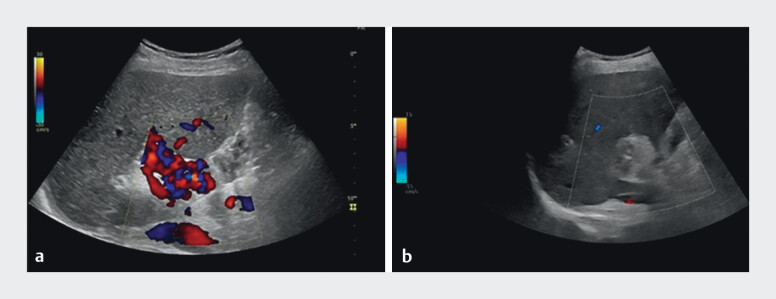 Fig. 4
Fig. 4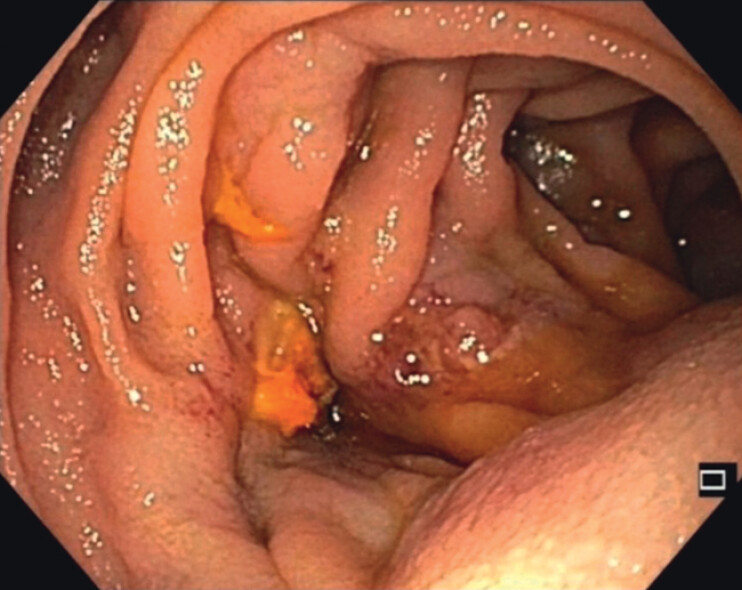 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Organ Transplantation Techniques and Outcomes · Gallbladder and Bile Duct Disorders
The development of varices is a common complication of untreated portal hypertension, typically caused by liver cirrhosis or portal vein thrombosis 1 . Uncontrolled portal pressure can result in life-threatening hemorrhages, most often from esophageal or gastric varices 2 . Endoscopic hemostasis or prophylaxis is essential. Treatment options include pharmacologic therapy, endoscopic ligation or glue injection, Sengstaken–Blakemore tamponade, radiological interventions, and surgery 3 . Varices can also occur in other GI segments, such as hepaticojejunostomy (HJS) after pancreatic surgery. Optimal management remains unclear due to the lack of large trials and guidelines 4 .
A patient presented with melena after a prior pylorus-preserving pancreaticoduodenectomy and partial portal vein resection for chronic pancreatitis. Portal vein thrombosis with secondary portal hypertension was evident. External endoscopy showed fresh blood in the small bowel and Grade III esophageal varices without active bleeding. CT imaging confirmed no active hemorrhage but extensive portosystemic collaterals. The patient was referred to the University Medical Center Göttingen.
A transhepatic portal vein stent was placed after successful recanalization, but in-stent thrombosis occurred, and a second attempt failed ( Fig. 1 ).
CT imaging confirming In-stent thrombosis.
Endoscopic intervention was then planned. Endoscopy visualized HJS and variceal convolutes. Due to their size, direct puncture was avoided ( Fig. 2 ). A guide wire was placed, and EUS confirmed a large adjacent vessel, supporting EUS-guided intervention.
a Endoscopic view of esophageal varices and b varices at the hepaticojejunostomy site.
One varix was treated with three fibered coils (7 mm each) and Histoacryl; another with two nonfibered coils (8 mm) and Histoacryl ( Fig. 3 ).
a Color Doppler sonographic visualization of hepaticojejunostomy varices; b endosonographic measurement of variceal size; c puncture of the varix and coil deployment; and d radiologic image showing deployed coils and Histoacryl.
Transabdominal ultrasound confirmed success without complications. Follow-up gastroscopy after 3 weeks showed favorable results ( Fig. 4 , Fig. 5 ).
a Preinterventional transcutaneous ultrasonography demonstrating varices and b postinterventional transcutaneous ultrasonography.
Postinterventional gastroscopic image of the varices at the BDA showing a favorable outcome.
This case demonstrates that endoscopic techniques can effectively treat varices in complex postoperative anatomy ( Video 1 ).
Upper gastrointestinal bleeding control by endoscopic ultrasound-guided coil and Histoacryl therapy of varices at the hepaticojejunostomy in a patient after pylorus-preserving pancreaticoduodenectomy and partial portal vein resection for chronic pancreatitis.Video 1
Endoscopy_UCTN_Code_TTT_1AO_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kovacs TOG Jensen DM Varices: Esophageal, Gastric, and Rectal Clin Liver Dis 20192362564210.1016/j.cld.2019.07.00531563215 · doi ↗ · pubmed ↗
- 2Gunarathne LS Rajapaksha H Shackel N Cirrhotic portal hypertension: From pathophysiology to novel therapeutics World J Gastroenterol 2020266111614010.3748/wjg.v 26.i 40.611133177789 PMC 7596642 · doi ↗ · pubmed ↗
- 3Liu B Li G Progress in Endoscopic and Interventional Treatment of Esophagogastric Variceal Bleeding Dis Markers 202220222.940578 E 610.1155/2022/2940578 PMC 910650635571609 · doi ↗ · pubmed ↗
- 4Garbuzenko DV Current approaches to the management of jejunal variceal bleeding at the site of hepaticojejunostomy after pancreaticoduodenectomy World J Gastroenterol 2024304083408610.3748/wjg.v 30.i 37.408339474403 PMC 11514537 · doi ↗ · pubmed ↗