Appendiceal adenocarcinoma diagnosed by endoscopic retrograde appendicitis therapy – the first clinical experience
Ning Su, Jiyu Zhang, Qingfen Zheng, Lixia Zhao, Bingrong Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
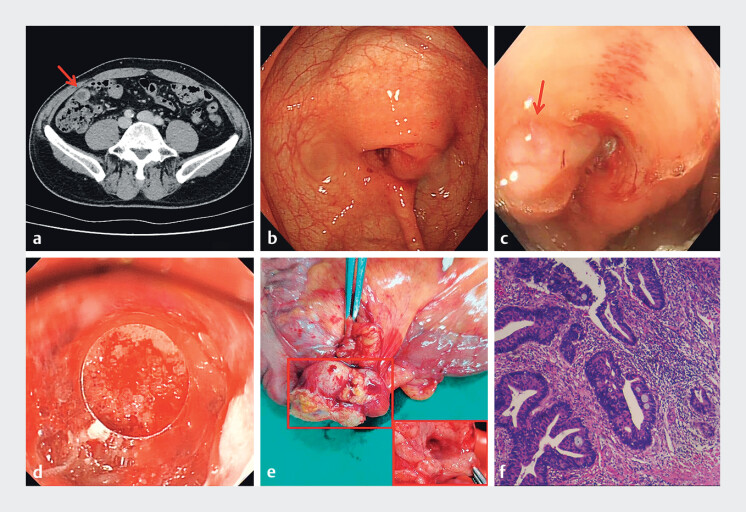 Fig. 1
Fig. 1- —Zhongyuan Talent Program
- —The Key R&D Program of Henan Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Appendicitis Diagnosis and Management · Gastric Cancer Management and Outcomes
A 67-year-old male was admitted to our hospital with intermittent abdominal pain. Physical examination revealed no tenderness at McBurneyʼs point but tenderness around the umbilicus. CT imaging showed a dilated appendix, intraluminal fluid, and wall thickening ( Fig. 1 a ).
a CT imaging showed a dilated appendix, intraluminal fluid, and wall thickening. b The appendiceal orifice showed an eccentric bulge, severe edema, and mucoid secretion. c There is a jelly-like secretion in the appendix cavity. d Adenomatous hyperplasia tissue was observed at the opening of the appendiceal. e Radical right hemicolectomy was performed. f Pathological image of the surgical resection specimen.
Based on these findings and the patient’s requirement, endoscopic retrograde appendicitis therapy (ERAT) was performed. The colonoscope was advanced to the terminal ileum, revealing an eccentric bulge, severe edema, and mucoid secretion at the appendiceal orifice ( Fig. 1 b, c ). A guidewire was inserted using a cone-shaped transparent cap, followed by catheter insertion. A large cavity was seen via appendiceal radiography, and no fecalith was found. Given the large opening of the appendix, a conical transparent cap was used directly for irrigation and enlargement. The secretions were mixed with masses resembling necrotic tumor tissue. After repeated irrigating with normal saline, adenomatous hyperplasia tissue was observed at the opening of the appendiceal ( Fig. 1 d ). A biopsy was taken, which confirmed the presence of adenocarcinoma. The patient subsequently underwent radical right hemicolectomy ( Fig. 1 e ). Pathological examination showed vascular invasion present, neural invasion absent, no regional lymph node metastasis, and negative surgical margins ( Fig. 1 f ). The patient's symptoms resolved postoperatively, and 1-year follow-up imaging showed no recurrence ( Video 1 ).
The whole diagnosis and treatment process of the patient.Video 1
To our knowledge, this may represent the first reported case of appendiceal adenocarcinoma diagnosed via ERAT. Beyond its established therapeutic role, ERAT demonstrates significant diagnostic potential by enabling direct endoscopic visualization of the appendiceal orifice – a capability that positions it as a potential gold standard for detecting appendiceal orifice lesions. Our experience, based on this case, suggests that ERAT might transform the diagnostic paradigm for appendiceal pathology, potentially improving patient outcomes through earlier detection and more precise planning.
Endoscopy_UCTN_Code_TTT_1AQ_2AJ