A rare cause of partial small bowel obstruction
Ben-Hua Wu, Jia-Lin Yuan, Li-Sheng Wang, Wen-Biao Chen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
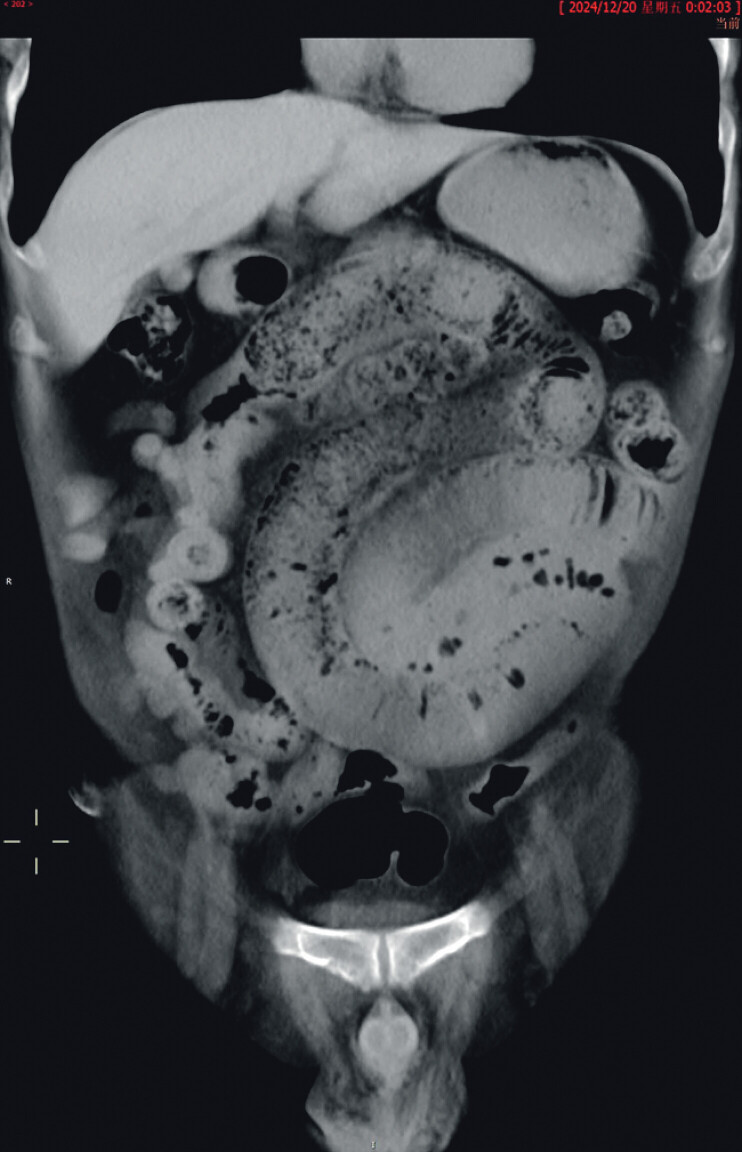 Fig. 1
Fig. 1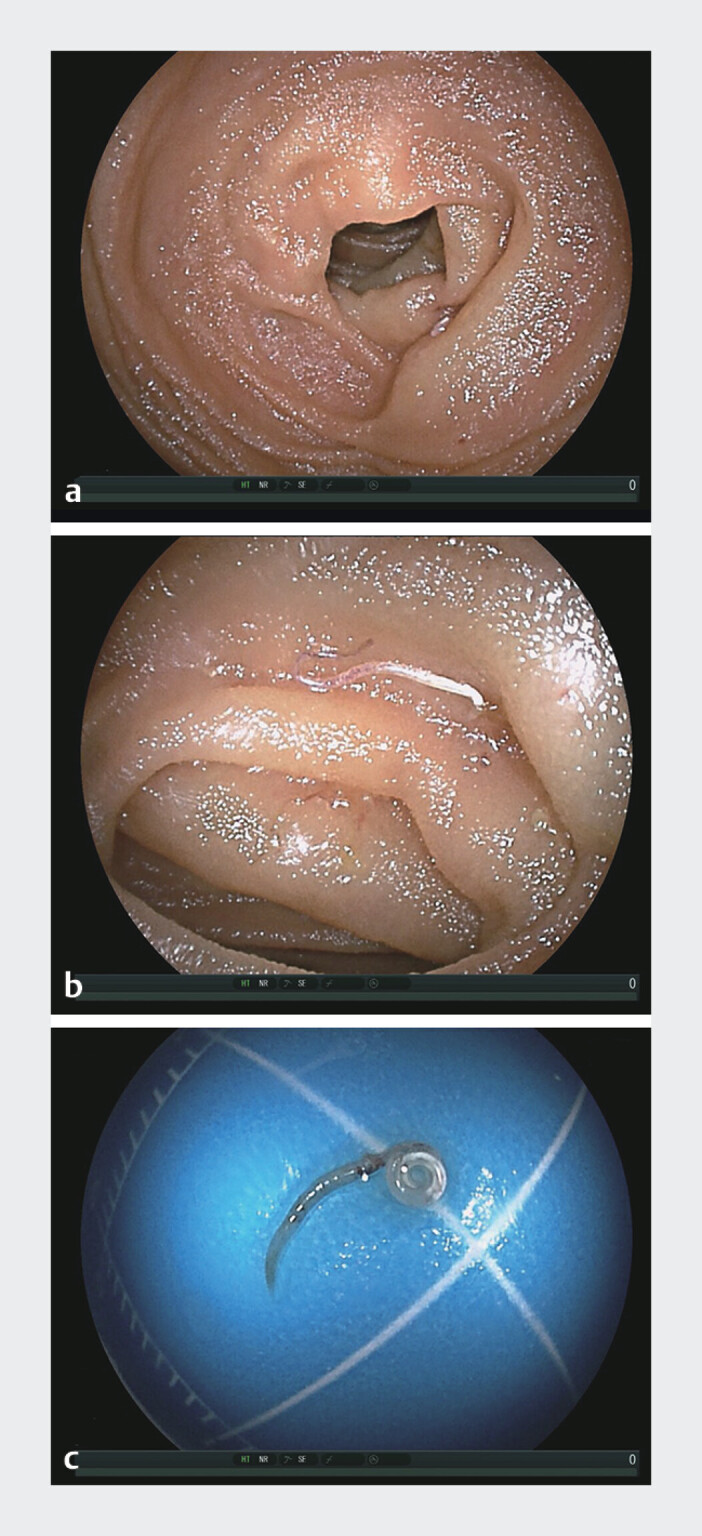 Fig. 2
Fig. 2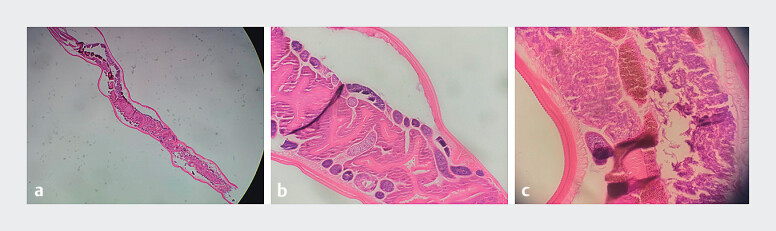 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiliary and Gastrointestinal Fistulas · Intestinal and Peritoneal Adhesions · Gastrointestinal disorders and treatments
A 59-year-old man presented with a five-month history of recurrent abdominal pain and vomiting. Five months prior to admission, during an episode of abdominal pain, an abdominal computed tomography (CT) revealed segmental wall thickening and blurring of the small bowel wall in the right mid-abdomen, with obscuration of the adjacent mesenteric fat planes. Mild upstream small bowel dilatation with fecalized content and mural blurring suggested partial small bowel obstruction ( Fig. 1 ). He was managed conservatively at a local hospital with fasting, intravenous fluids, and antibiotic therapy, which resulted in symptomatic improvement. However, he subsequently experienced two milder episodes of abdominal pain, neither of which received a medical evaluation.
The computed tomography imaging manifestations suggest incomplete intestinal obstruction.
On admission, a physical examination revealed a soft, non-distended, and non-tender abdomen. Laboratory investigations revealed a normal white blood cell count (6.87 × 10^9/L) with mild eosinophilia (14.3%). No abnormalities were found in other blood biochemical tests. Upper gastrointestinal endoscopy revealed a nonspecific gastroduodenal inflammation. Random colonoscopic biopsy results were unremarkable. During oral double-balloon enteroscopy, advancement to approximately 300 cm into the ileum revealed a segment of markedly edematous and hyperemic small-bowel mucosa ( Fig. 2 a ). An actively motile live worm surrounded by congested and edematous mucosa with mild hemorrhage was observed penetrating the intestinal mucosa ( Fig. 2 b ). The helminth was successfully extracted using the biopsy forceps ( Fig. 2 c , Video 1 ). Histopathological analysis confirmed that the specimen was Enterobius vermicularis ( Fig. 3 a–c ). Based on this, the patient was clearly diagnosed with partial small bowel obstruction caused by enterobiasis of the small intestine. The patient underwent a course of albendazole, an anthelmintic agent effective against Enterobius vermicularis . Following antiparasitic therapy, the patient achieved complete resolution of symptoms, with no further episodes of abdominal pain or vomiting.
The double-balloon enteroscopy revealed incomplete intestinal obstruction caused by Enterobius vermicularis. a Intestinal mucosa congestion and edema. b The double-balloon enteroscopy revealed an active worm, surrounded by congested and edematous mucosa, with mild bleeding. c Worm, adult specimen.
The double-balloon enteroscopy revealed an actively moving worm penetrating the edematous, hyperemic, and slightly bleeding intestinal mucosa, followed by its successful retrieval with biopsy forceps.Video 1
The histopathological analysis confirmed that this specimen was a Enterobius vermicularis worm.
Small bowel involvement by Enterobius vermicularis is exceptionally rare, particularly when it presents as a mechanical intestinal obstruction. In this case, the diagnosis was established through enteroscopy, which directly visualized a live worm traversing the inflamed mucosa of the ileal segment. Previous reports have documented small bowel obstruction secondary to parasitic infections such as Schistosoma-associated Meckel’s diverticulitis 1 and nematode infestation 2 , both of which were diagnosed intraoperatively through laparoscopy or laparotomy. In contrast, our case highlights the role of deep enteroscopy as a minimally invasive diagnostic and therapeutic modality, representing a rare instance of small bowel obstruction caused by Enterobius vermicularis infection that was successfully managed without surgical intervention.
Endoscopy_UCTN_Code_CCL_1AB_2AZ_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Almadi F Aljohani E Rare cause of complicated Meckel's with Schistosoma infection: An unusual cause of acute intestinal obstruction in adults Int J Surg Case Rep 20206625725910.1016/j.ijscr.2019.11.03931877547 PMC 6931112 · doi ↗ · pubmed ↗
- 2Appleby D Kapoor W Karpf M Anisakiasis: nematode infestation producing small-bowel obstruction Arch Surg 198211783610.1001/archsurg.1982.013803000760167200765 · doi ↗ · pubmed ↗