Simultaneous Presentation of Post-Transplant Lymphoproliferative Disorder (PTLD) and Acute Cellular Rejection (ACR) in a Liver Transplant Recipient: A Therapeutic Conundrum
Ankit Mishra, Matthew Kubina, Dhiraj K. Peddu, Benjamin L. Viglianti, Anamarija M. Perry, Priya Kathuria, Hellan Kwon, Shannon A. Carty, Patricia Bloom

TL;DR
A liver transplant patient developed two serious complications at the same time, requiring careful balancing of treatments to preserve the transplant and manage both conditions.
Contribution
This case study presents a rare co-occurrence of PTLD and ACR in a liver transplant patient and highlights a successful therapeutic strategy.
Findings
Early PTLD and severe ACR occurred simultaneously in a liver transplant recipient.
Prioritizing treatment of rejection preserved allograft function and led to resolution of both conditions.
A multidisciplinary approach was essential in managing the conflicting complications.
Abstract
We report a 64-year-old liver transplant recipient who developed early nondestructive post-transplant lymphoproliferative disorder (PTLD) and severe acute cellular rejection (ACR) concurrently. Hepatic lymphadenopathy led to a liver biopsy demonstrating early PTLD. Immunosuppression (IS) was reduced for early PTLD, which led to acute liver injury requiring high-dose steroids. However, subsequent augmentation in immunosuppression for ACR led to progression of PTLD, requiring rituximab treatment. This case highlights the complexity of managing conflicting liver transplant complications and underscores the importance of a multidisciplinary approach. In our case, prioritizing the treatment of rejection preserved the allograft function. Long-term follow-up showed complete resolution of both rejection and PTLD.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
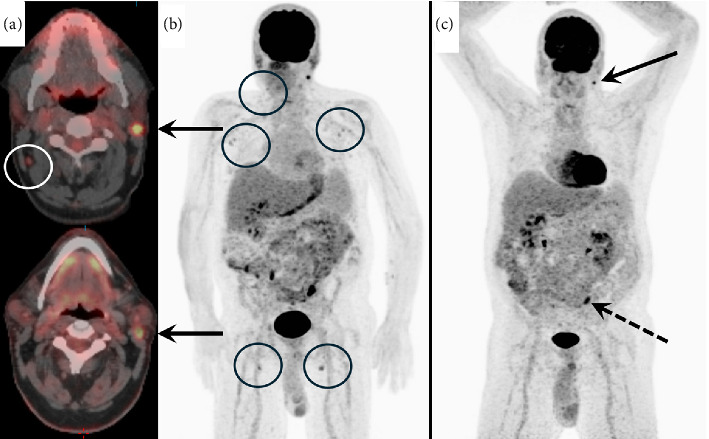 Figure 1
Figure 1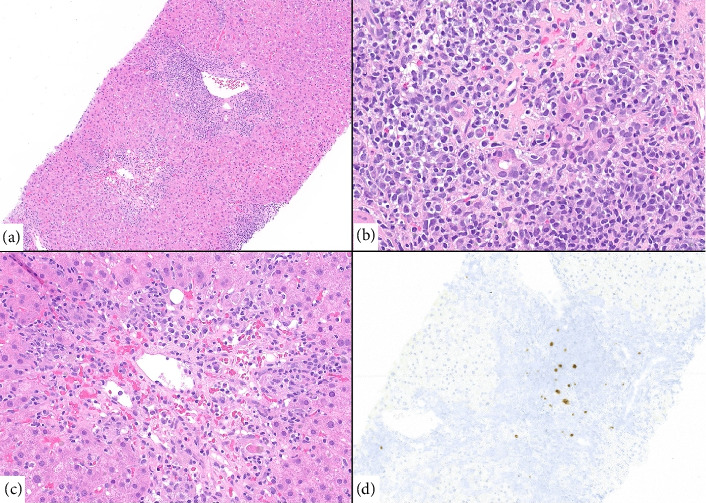 Figure 2
Figure 2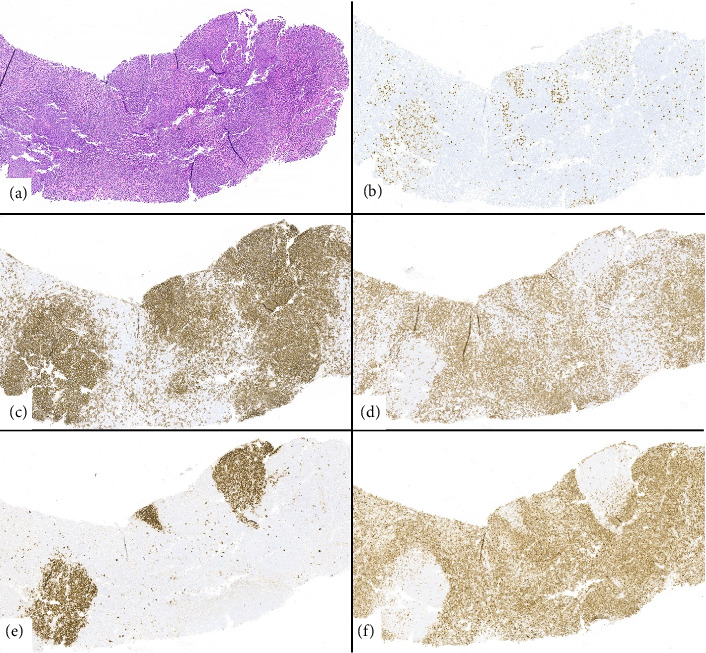 Figure 3
Figure 3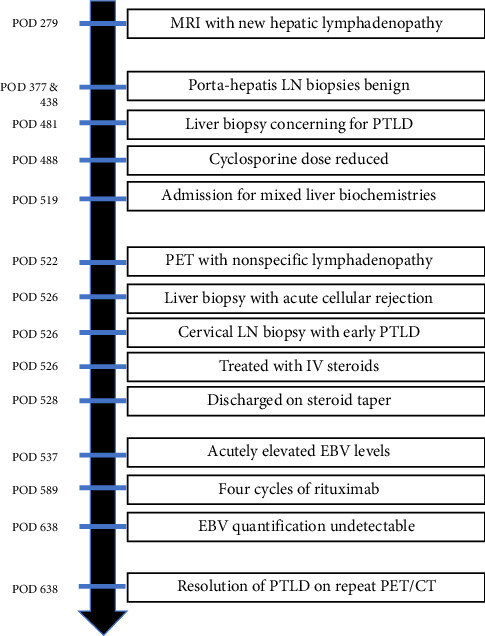 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · Polyomavirus and related diseases · Cytomegalovirus and herpesvirus research
1. Introduction
Post-transplant lymphoproliferative disorder (PTLD) and severe acute cellular rejection (ACR) are post liver transplantation (LT) complications, each contributing to high rates of morbidity and mortality, and necessitate divergent treatment strategies. PTLD occurs through uncontrolled lymphocyte proliferation, with early PTLD typically driven by Epstein–Barr virus (EBV) [1, 2]. ACR is also common after LT, with an incidence of up to 25%–30% and often occurring within 1 month post-transplantation [3]. ACR occurs due to recipient T cells recognizing donor alloantigens, which results in T-cell recruitment and an innate immune response [4]. The mainstay of early, nondestructive PTLD management is reduction of immunosuppression, while ACR is usually managed by augmenting IS, typically with high-dose steroids and/or escalation in immunosuppressive therapies [3]. Specifically, recommendations state to discontinue antimetabolites (e.g., azathioprine and mycophenolate mofetil) and reduce calcineurin inhibitors by 50%; however, such reduction carries a risk of rejection [5]. Our literature search did not identify any liver transplant cases with biopsy-proven concurrent PTLD and ACR, but a case report published in 2001 demonstrated a similar clinical scenario in a lung transplant patient [6]. This patient likely had coexistent ACR and PTLD which is different from our case where the patient developed ACR after RIS for early PTLD [6]. The authors in this study point out the possibility of two different subpopulations of T cells: EBV-specific T cells implicated in PTLD and allospecific T cells directed toward alloantigens in ACR [6]. This report describes the first documented instance of simultaneously managing PTLD and severe acute liver rejection, underscoring the necessity of a tailored, multidisciplinary approach.
2. Case Report
A 64-year-old man with a history of Type 2 diabetes mellitus, hypertension, metabolic dysfunction–associated steatotic liver disease with cirrhosis, and multifocal moderately differentiated hepatocellular carcinoma (HCC), status-post orthotopic LT (donor EBV+, recipient EBV-) in August 2022, underwent a routine liver MRI on postoperative day (POD) 279 as part of the intermediate risk protocol for HCC monitoring. The MRI revealed new porta hepatis lymphadenopathy. Two porta hepatis lymph nodes biopsies obtained via endoscopic ultrasound on POD 377 and 438, respectively, were pathologically benign. A follow-up MRI on POD 445 showed continued enlarging perihepatic lymph nodes. Given the continued enlarging lymph nodes on liver MRI, the patient underwent a liver biopsy on POD 481.
The liver biopsy demonstrated few aggregates of small lymphocytes and scattered EBV-positive cells, with a quantitative plasma EBV (qEBV) level of 42,882 I.U./mL. Given the nondisruptive nature of lymphocytes, as well as elevated serum EBV viral load, there was a concern for early PTLD, and the patient's cyclosporine dose was reduced from 100 to 75 mg twice daily on POD 488. On POD 519, the patient was urgently admitted to the inpatient liver service at the University of Michigan for rising liver biochemistries, consistent with mixed pattern of injury in the setting of recently decreased immunosuppression (aspartate aminotransferase 93–321 U/L [< 34]; alanine aminotransferase 117–420 U/L [10–49]; alkaline phosphatase 187–287 U/L [40–116]; and total bilirubin 0.8–1.1 mg/dL [0.2–1.2]).
During this admission, a nuclear medicine fluorodeoxyglucose (FDG) positron emission tomography (PET) scan showed FDG-avid nonspecific lymphadenopathy in the thorax, abdomen, and pelvis (Figures 1(a), 1(b)). The patient's qEBV level was 2518 I.U./mL. A cervical lymph node and liver biopsy were performed. The liver biopsy indicated a severe bile duct injury and endotheliitis concerning for severe ACR (Figure 2). The cervical lymph node biopsy showed follicular hyperplasia with numerous EBV-positive cells, consistent with early/non-destructive PTLD (Figure 3). After extensive discussion with pathology, hematology, and hepatology, the patient was treated with a three-day course of methyl-prednisolone (100 mg on Day 1, 250 mg on Day 2, and 250 mg on Day 3) for severe acute cellular liver rejection. This was deemed the most immediate threat to preserve his transplanted liver function [7].
Shortly after his treatment with high-dose IV steroids, he was discharged home with a steroid taper (60 mg for 7 days, 50 mg for 7 days, and then 40 mg for 7 days with ongoing prednisone taper) and his prior IS regimen (mycophenolate mofetil 500 mg two times daily and cyclosporine 75 mg two times daily). A few days later, he underwent outpatient laboratory testing to monitor his liver function tests (LFTs) as well as qEBV levels. This demonstrated improving liver biochemistries, but acute elevation in EBV level from 2518 to 10,252 I.U./mL, concerning for rapidly progressing PTLD. The patient was evaluated by hematology and received four doses of weekly rituximab 375 mg/m^2^ for early PTLD in the setting of ACR preventing a reduction in immunosuppression. Post-treatment, his EBV quantification rapidly came down to undetectable (10,252 I.U./mL ⟶ 211 I.U./mL ⟶ 59 I.U./mL ⟶ < 35 I.U./mL ⟶ undetectable), PET/CT demonstrated complete metabolic response, and his LFTs have remained within normal limits (Figure 1(c)). The patient had no recurrence of PTLD or ACR with the last follow-up on POD 932. He has remained on prednisone 3 mg daily, mycophenolate mofetil 500 mg two times daily, and cyclosporine 75 mg two times daily (last trough on 8/26/25 was 99 ng/mL) (Figure 4).
3. Discussion
ACR and PTLD are distinct pathophysiological processes, each requiring careful management in transplant recipients. Lifelong immunosuppression is essential for all transplant patients to preserve liver allograft function. PTLD is a serious post-transplant complication, occurring in 1%–20% of solid organ transplant (SOT) recipients [1, 8]. Based on timing, PTLD is classified into early (12–24 months post-SOT) and late (> 24 months post-SOT) categories [8]. Additionally, PTLD is further categorized into nondestructive, polymorphic, and monomorphic subtypes. First-line treatment for early nondestructive PTLD typically involves reducing immunosuppression, enabling the patient's immune system to mount a T-cell response against proliferating malignant cells [9]. In contrast, polymorphic and monomorphic PTLD often require reduction in immunosuppression, rituximab, and sometimes immunochemotherapy, in cases of B-cell lymphoid neoplasms [8].
Rejection occurs when the recipient's immune system mounts a response against the donor's major histocompatibility complex [10]. The Banff Working Group classifies cellular rejection as T-cell-mediated rejection (TCMR) with acute and chronic components [11, 12]. TCMR is primarily defined by T-cell infiltrates, with histologic features including ductulitis, portal or central venous endotheliitis, and mixed portal inflammation [10, 13]. Notably, minimal to no inflammatory activity is observed in hepatocytes adjacent to the portal triad's connective tissue [13].
Our patient presented with an unusual case of early PTLD alongside features suspicious for severe ACR. To date, no documented cases have demonstrated the concurrent presentation of these two distinct pathophysiological processes. The liver showed plasmacytic infiltrates, atypical lymphocytes, and severe bile duct injury with endotheliitis (Figure 2), findings suggestive of severe ACR. The Banff score for this patient's ACR was 7, with individual scores of 3 for portal inflammation, 3 for bile duct damage, and 1 for venous endothelial inflammation.
The cervical lymph node met the histologic criteria for early PTLD; however, the histologic appearance of the liver infiltrates did not align with PTLD, as there was no morphologic evidence of tissue effacement (Figure 3). We believe that the EBV-positive cells in the liver were likely due to EBV viremia. Rituximab therapy carries important infection risks, particularly when used with corticosteroids. These include hepatitis B virus reactivation and pneumocystis jirovecii pneumonia (PJP) [14, 15]. For our patient, we began trimethoprim-sulfamethoxazole (400/80 mg once daily) when pulse dose steroids were started for PJP prophylaxis and obtained HBV serologies prior to initiating rituximab.
In summary, we present this unique case to highlight the clinical dilemma where both increased and decreased IS are required simultaneously [7]. In this specific scenario, high-dose steroids followed by one course of weekly rituximab successfully managed both conditions. The uniqueness of this case lies in the fact that while reducing immunosuppression is typically sufficient for early nondestructive PTLD, it was not a viable option due to the presence of severe ACR.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Allen U. D. Preiksaitis J. K. Post-Transplant Lymphoproliferative Disorders, Epstein-Barr Virus Infection, and Disease in Solid Organ Transplantation: Guidelines From the American Society of Transplantation Infectious Diseases Community of Practice Clinical Transplantation 2019 September 339p. e 1365210.1111/ctr.136522-s 2.0-8506991816531230381 · doi ↗ · pubmed ↗
- 2Styczynski J. Sadlok J. Styczynski T. Marjanska A. Richert-Przygonska M. Management of Resistant Post-Transplant Lymphoproliferative Disorder: CAR-T is a New Option Anticancer Research 2022 November 42115181518610.21873/anticanres.1602436288856 · doi ↗ · pubmed ↗
- 3Choudhary N. S. Saigal S. Bansal R. K. Saraf N. Gautam D. Soin A. S. Acute and Chronic Rejection After Liver Transplantation: What a Clinician Needs to Know Journal of Clinical and Experimental Hepatology 2017 December 7435836610.1016/j.jceh.2017.10.0032-s 2.0-8503407614429234201 PMC 5715482 · doi ↗ · pubmed ↗
- 4Maspero M. Ali K. Cazzaniga B. Acute Rejection After Liver Transplantation With Machine Perfusion Versus Static Cold Storage: A Systematic Review and Meta-Analysis Hepatology 2023 September 78383584610.1097/hep.000000000000036336988381 · doi ↗ · pubmed ↗
- 5Parker A. Bowles K. Bradley J. A. Management of Post-Transplant Lymphoproliferative Disorder in Adult Solid Organ Transplant Recipients-BCSH and BTS Guidelines British Journal of Haematology 2010 June 149569370510.1111/j.1365-2141.2010.08160.x 2-s 2.0-7795263079320408848 · doi ↗ · pubmed ↗
- 6Longchampt E. Achkar A. Tissier F. Rabbat A. Audouin J. Molina T. J. Coexistence of Acute Cellular Rejection and Lymphoproliferative Disorder in a Lung Transplant Patient Archives of Pathology & Laboratory Medicine 2001 November 125111500150210.5858/2001-125-1500-coacra 11698014 · doi ↗ · pubmed ↗
- 7Mishra A. Kathuria P. Peddu D. S 4545 Simultaneous Presentation of Post-Transplant Lymphoproliferative Disorder (PTLD) and Acute Cellular Rejection (ACR) in a Liver Transplant Recipient: A Therapeutic Conundrum American Journal of Gastroenterology 202411910 SS 2893 S 289410.14309/01.ajg.0001047548.68165.3f · doi ↗
- 8Zaffiri L. Chambers E. T. Screening and Management of PTLD Transplantation 2023 November 107112316232810.1097/tp.000000000000457736949032 · doi ↗ · pubmed ↗