Rapid Initiation of Hyperbaric Oxygen Therapy for Multiple Simultaneous Cases of Acute Carbon Monoxide Poisoning at a Single Center
Takayuki Kurokawa, Ichiyo Ohara, Chie Watanabe, Koji Kuwata, Itsumi Hashimoto, Manabu Kitagaki, Takehiko Murakami

TL;DR
This paper describes the successful treatment of 11 patients with acute carbon monoxide poisoning using hyperbaric oxygen therapy at a single hospital in Japan.
Contribution
The study demonstrates the feasibility of managing multiple simultaneous carbon monoxide poisoning cases using HBOT in a single facility.
Findings
All patients received normobaric oxygen and those with severe conditions underwent HBOT within 3 hours of hospital arrival.
Symptoms resolved completely within 2 to 4 weeks with no physical or cognitive sequelae.
The study emphasizes the importance of disaster medicine training and coordination in managing mass casualty incidents.
Abstract
Hyperbaric oxygen therapy (HBOT) is used to treat acute carbon monoxide poisoning. However, few reports have detailed its use in large patient cohorts, and optimal management guidelines have yet to be established. Herein, we report the clinical presentation and simultaneous treatment of multiple patients experiencing acute carbon monoxide poisoning on an offshore ship within the territorial waters of Japan. Eleven patients were promptly transported to our hospital from a Japanese Maritime Self-Defense Force destroyer owing to accidental acute carbon monoxide poisoning. We opted to treat this incident as a mass casualty and immediately appointed a medical control officer and established medical teams. The medical control officer guided the general treatment plan and coordinated with the various sections, and the medical teams treated the patients. The patients were immediately…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
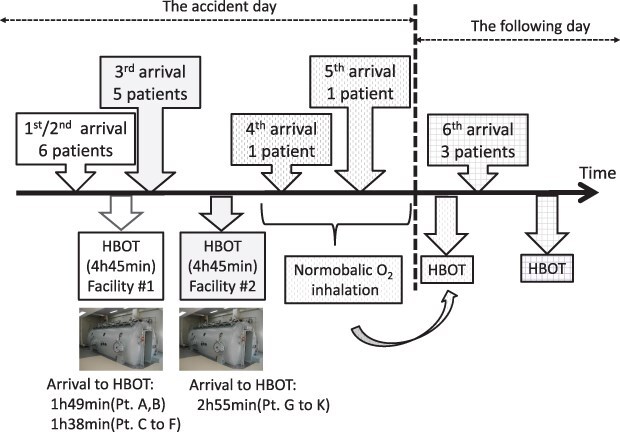 Figure 1
Figure 1| Blood CO-Hb (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pt | Age (years),sex | SDF/Civ | LOC | Symptoms | Medical history | Smoker | Pre-HBOT | Day 0 | Day 1 | HBOT protocol |
| A | 65, M | Civ | Yes | Numbness, fatigue, headache | None | Yes | 41.5 | 2.0 | 0.8 | TT6 × 3, TT5 × 2 |
| B | 73, M | Civ | No | Eye field abnormality, headache | None | Yes | 37.4 | 3.6 | 0.8 | TT6 × 3, TT5 × 2 |
| C | 67, M | Civ | No | None | None | Yes | 36.1 | 2.7 | 0.9 | TT6 × 3, TT5 × 2 |
| D | 40, M | Civ | No | Numbness, fatigue | Type 2 DM | Yes | 31.8 | 0.8 | 0.0 | TT6 × 3, TT5 × 2 |
| E | 38, F | Civ | Yes | Numbness, hyperventilation | None | Yes | 18.6 | 0.8 | 0.5 | TT6 × 3, TT5 × 2 |
| F | 49, M | SDF | No | Dull headache | None | Yes | 22.8 | 0.6 | 0.6 | TT6 × 2, TT5 × 3 |
| G | 23, M | SDF | No | Dull headache | None | Yes | 15.8 | 0.5 | 0.5 | TT6 × 1, TT5 × 2 |
| H | 29, M | SDF | No | Dull headache | None | Yes | 10.1 | 0.6 | 0.5 | TT6 × 1, TT5 × 2 |
| I | 46, M | SDF | No | Chills | None | Yes | 8.7 | 0.8 | 0.7 | TT6 × 1, TT5 × 2 |
| J | 46, M | SDF | No | Dull headache | None | No | 6.4 | 0.6 | 0.6 | TT6 × 1, TT5 × 2 |
| K | 29, M | SDF | No | Dull headache | None | Yes | 3.9 | 0.3 | 0.3 | TT6 × 1, TT5 × 2 |
| L | 27, M | SDF | No | Headache, nausea | None | Yes | 3.5 | – | 0.8 | TT6 × 1, TT5 × 2 |
| M | 46, M | SDF | No | Headache | None | Yes | 2.8 | – | 0.5 | TT6 × 2, TT5 × 1 |
| N | 39, M | SDF | No | Headache | None | Yes | 1.0 (Day 1) | – | 0.4 | TT5 × 3 |
| O | 47, M | SDF | No | Eye field abnormality, headache | None | Yes | 1.4 (Day 1) | – | 0.9 | TT5 × 3 |
| P | 51, M | SDF | No | None | None | Yes | 3.6 (Day 1) | – | 1.1 | TT5 × 3 |
| Time | Event | Details |
|---|---|---|
| ∼10:30 | Accident occurred | One patient with LOC on the destroyer |
| ∼10:35 | Emergency call | Nearest JMSDF MSU team (EMT, nurses) arrived at the destroyer |
| ∼10:40 | Triage at the scene by the MSU team | |
| 10:45 | First call | “The accident in the destroyer may be due to ACOP.” |
| “Request to accept 4 patients obtained, one with LOC.” | ||
| 10:48 | Mass casualty declared | Assigned an MCO, called for an HBOT team |
| 11:00 | Second call | “Request to accept 1 conscious patient.” |
| 11:15 | Third call | “Request to accept 6 patients. LOC patient recovered consciousness.” |
| Assigned 6 medical teams (MD, nurses) | ||
| 11:24 | Patient arrival | Patients A and B, via ambulance |
| 11:35 | Patient arrival | Patients C to F, via ambulance |
| 11:40 | ACOP diagnosed | |
| HBOT control (first) | The MCO approved the provision of HBOT. | |
| 11:45 | Patient arrival | Patients G to K, walk-in |
| 12:50 | HBOT set-up (first) | Patients A to F transferred to our HBOT facility |
| 13:00 | HBOT control (second) | The MCO began negotiating to another HBOT facility, and assembling a second HBOT team. |
| 13:13 | HBOT start (first) | Protocol: Table 6 of the US Diving Manual |
| 14:15 | Patient arrival | Patient L, by walk-in |
| 14:20 | HBOT set-up (second) | Patients G to K, transferred to another HBOT facility |
| 14:35 | HBOT start (second) | Protocol: Table 6 of the US Navy Diving Manual |
| 16:45 | Patient arrival | Patient M, walk-in |
| 18:10 | HBOT finish (first) | No problems |
| 19:32 | HBOT finish (second) | No problems |
| Pt. | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Criteria | A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P |
| Impairment of consciousness | Yes | No | No | No | Yes | No | No | No | No | No | No | No | No | No | No | No |
| Initial CO-Hb > 25% | Yes | Yes | Yes | Yes | No | No | No | No | No | No | No | No | No | No | No | No |
| Age > 36 | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Existing physical symptom | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeme Oxygenase-1 and Carbon Monoxide · Poisoning and overdose treatments · Neonatal Health and Biochemistry
INTRODUCTION
Carbon monoxide (CO) is generated by the incomplete combustion of organic matter. In confined spaces, CO accumulation can result in acute CO poisoning (ACOP). In accidental events, mass exposure of a large number of individuals to CO may occur simultaneously.^1^
Our 100-bed hospital is managed by the Japanese Maritime Self-Defense Force (JMSDF). It is equipped with 2 type-2 multiplace hyperbaric oxygen therapy (HBOT) chambers and actively performs HBOT. A similar type-2 HBOT facility near our hospital is managed by another JMSDF squadron.
In this report, we describe the simultaneous treatment of multiple patients afflicted with ACOP on an offshore ship within the territorial waters of Japan. Notably, initial HBOT was immediately administered, and no neurological sequelae were encountered.
CASE PRESENTATION
Ethical standards were applied in this human research study.
In September 2017, a civilian worker (patient A in Table 1) on a JMSDF destroyer experienced malaise and loss of consciousness while performing repairs inside a sewage tank with a running engine generator. His colleagues attempted to rescue him but subsequently experienced similar symptoms (Table 1). Although ventilation within the tank took place indoors, the exhaust gas from the generator was released outdoors through a duct.
Details of the timeline are presented in Table 2 and Figure 1. Initially, the information from the scene was confusing, and we struggled to organize a medical treatment system. However, once it became clear that at least 6 patients were involved, we opted to treat the CO exposure (and presumed ACOP) as a mass casualty. To manage the event without disrupting outpatient care, we appointed a medical control officer (MCO) and established 6 separate medical teams based in the emergency department. The MCO guided the general treatment plan and coordinated the various aspects of the plan, and the medical teams were responsible for treating the patients. The patients were triaged at the aid station on the pier, and 11 patients (A to K) were transported by ambulance to our hospital, located approximately 5 minutes away, in order of severity. Patients L and M were late-arrival walk-ins.
Time course of arrival to initial HBOT.
Patient characteristics are presented in Table 1. Upon arrival at our hospital, all patients were immediately administered normobaric oxygen via a facial mask. The results of the physical exams were unremarkable for all 16 patients, with no obvious injuries. Laboratory results, including pCO_2_ and pO_2_ levels, were within normal limits, except for carboxyhemoglobin (CO-Hb) levels, which were elevated in patients A to K.
We immediately divided the patients into 2 groups (most severe and less severe) and administered HBOT within 3 hours of the exposure to the most severely injured patients (A to F) and approximately 4 hours after the exposure to the less severely injured patients (G to K). The general conditions and vital signs of patients L and M were stable; therefore, normobaric oxygenation therapy was initially administered, and HBOT was performed the next day. The day following the accident, elevated CO-Hb levels or post-exposure symptoms despite normal CO-Hb levels were observed in outpatients N to P.
All 16 patients were diagnosed with ACOP and underwent ongoing normobaric oxygenation therapy and at least 3 HBOT sessions, as outlined in Treatment Tables (TT) 5 and 6 of the U.S. Navy Diving Manual, during hospitalization.^2^ Not all patients required myringotomy. Although symptoms resolved in all patients after the second HBOT session, 6 patients (A to F) underwent 5 sessions owing to elevated CO-Hb levels. All patients were discharged after completing their scheduled HBOT sessions and were followed up at 2 and 4 weeks after the exposure. As soon as possible after admission and at the 4-week follow-up, the patients underwent brain magnetic resonance imaging and cognitive function tests. No abnormalities were evident in any of the patients at either time.
DISCUSSION
We report the clinical presentation and treatment of a large number of patients with ACOP occurring at an offshore location. The treatment of ACOP primarily aims to prevent (1) acute organ hypoxia, especially in the brain and myocardium, by reducing CO-Hb levels during the acute phase and (2) late-onset brain damage and neuropsychiatric disorders.^1^ Despite controversy regarding the role of HBOT in ACOP,^3–5^ some studies suggest that HBOT reduces the risk of chronic cognitive impairment in patients with specific symptoms.^6,7^ In our cohort, several criteria for ACOP were met (Table 3), including impaired consciousness (patients A and E), CO-Hb of 25% or more (patients A to D), and age over 36 years (patients A to F, I, J, and M to P) (Table 3).^1,7,8^ Although patients G, H, K, and L did not meet these criteria, they were considered eligible for HBOT because they exhibited symptoms and worked in the same confined space as did the other patients.^1^
In our study, treatment proceeded smoothly owing to the early admission of the large cohort and the appointment of an MCO to manage various adjustments. HBOT was planned, and all 16 patients received treatment as scheduled. Although a single HBOT session can last more than 4 hours,^2^ many patients can be treated simultaneously in a type-2 HBOT facility. Therefore, if the number of patients, their symptoms, and the facility’s treatment capacity and equipment performance are deemed acceptable, multiple patients can be treated simultaneously in a single facility.
We could find no consensus regarding the appropriate HBOT protocol for ACOP treatment; different protocols have been presented.^1,4^ Therefore, we performed the protocols listed in TT 5 and 6 of the U.S. Navy Diving Manual,^2^ which is frequently used at our facility. In TT 6, the patient is pressurized to 60 feet and administered oxygen for 60 minutes and then pressurized to 30 feet and administered oxygen for 120 minutes. The total treatment time is 4 hours and 45 minutes. In TT 5, the patient is pressurized to 60 feet and administered oxygen for 40 minutes and then pressurized to 30 feet and administered oxygen for 20 minutes. The total treatment time is 2 hours and 15 minutes.
We determined that patients A to F, who exhibited particularly high CO-Hb levels, should receive 5 HBOT sessions. Given their severe ACOP, we aimed to maximize oxygen administration through HBOT. However, we recognized that dispensing an excessive amount of oxygen increases the risk of oxygen toxicity. Therefore, we planned to provide an oxygen amount that would avoid this risk while still being effective. The protocol for doing so was determined under the supervision of an HBOT expert. There were no adverse effects of the treatment and no ACOP sequelae. However, the number of HBOT sessions and choice of protocol require continued discussion.
In a mass casualty event, patients should be dispersed to various facilities with appropriate treatment capabilities. Based on preliminary observations, including transient loss of consciousness in some patients, the cause of the symptoms in the present report was likely ACOP. Therefore, we determined that immediate HBOT was necessary, and 11 patients (A to K) were simultaneously admitted to our hospital. Notably, dispersing patients to more distant facilities would have required oxygenation during transport, numerous oxygen cylinders, and several ambulances, leading to a significant delay in HBOT initiation, as described by Valerio et al.^9^ In the present study, the time from ASOP onset to HBOT initiation was within 3 hours for patients A to F and approximately 4 hours for patients G to K (Table 2). Lee et al. reported that the neurocognitive prognosis is significantly worse when HBOT is initiated ≥6 vs. <6 hours after ACOP onset.^10^ Therefore, treating all patients at our facility was the best option, and treatment was successfully accomplished by dividing the patients into 2 severity-based groups.
Important for a successful treatment of ACOP by HBOT is a full understanding of the urgency of the situation by not only the medical staff but also receptionists, administrators, drivers, and procurers of medical equipment such as oxygen. Cooperation among these individuals and knowledge of disaster medicine by all, including the administrative staff, is essential. However, a different strategy may be required for larger exposure groups or even for the same exposure group, depending on the timing and clinical presentations. Specifically, if the number of patients exceeds the capacity of the HBOT facility, evacuation to and performance of HBOT at another facility should be considered in addition to treatment at the facility following triage. Therefore, when training HBOT personnel to handle a large number of patients, the possibility of ACOP among the patients should be taken into account.
CONCLUSION
We initiated HBOT almost simultaneously at a single facility despite a large number of patients with ACOP and obtained good outcomes. In cases where HBOT may be beneficial and the number of nearby facilities is limited, treatment at a single facility should be considered to prioritize early treatment initiation. Assigning an MCO for local disasters and focused coordination can ensure smoother operation and effective treatment. Importantly all staff members, including managers, should understand the concept of disaster medicine, and HBOT facilities should conduct regular training sessions for potential situations involving a large number of patients with ACOP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jain KK . Carbon monoxide and other tissue poisons. In: Jain KK, ed. Textbook of Hyperbaric Medicine. 6th ed. Springer; 2017:131–54
- 2U.S. Navy . U.S. Navy Diving Manual Revision 7. 2016;SS 521-AG-PRO-010. Updated December 2016. Accessed October 23, 2024. https://www.navsea.navy.mil/Portals/103/Documents/SUPSALV/Diving/US%20DIVING%20MANUAL_REV 7.pdf?ver=2017-01-11-102354-393
- 3Weaver LK . Carbon Monoxide Poisoning. Undersea Hyperb Med. 2020;47(2):151–69.doi: 10.1016/S 0749-0704(05)70056-732176957 · doi ↗ · pubmed ↗
- 4Rose JJ, Wang L, Xu Q, et al Carbon Monoxide Poisoning: Pathogenesis, Management, and Future Directions of Therapy. Am J Respir Crit Care Med. 2017;195(5):596–606.doi: 10.1164/rccm.201606-1275 CI 27753502 PMC 5363978 · doi ↗ · pubmed ↗
- 5Nañagas KA, Penfound SJ, Kao LW. Carbon Monoxide Toxicity. Emerg Med Clin N Am. 2022;40(2):282–313. doi: 10.1016/j.emc.2022.01.00535461624 · doi ↗ · pubmed ↗
- 6Weaver LK, Hopkins RO, Chan KJ. Hyperbaric Oxygen for Acute Carbon Monoxide Poisoning. N Engl J Med. 2002;347(14):1057–67.doi: 10.1056/NEJ Moa 01312112362006 · doi ↗ · pubmed ↗
- 7Thom SR . Carbon monoxide pathophysiology and treatment. In: Neuman TS, Thom SR, eds. Physiology and Medicine of Hyperbaric Oxygen Therapy. Saunders; 2008:321–47
- 8Weaver LK, Valentine KJ, Hopkins RO. Carbon Monoxide Poisoning: Risk Factors for Cognitive Sequelae and the Role of Hyperbaric Oxygen. Am J Respir Crit Care Med. 2007;176(5):491–7.doi: 10.1164/rccm.200701-026OC 17496229 · doi ↗ · pubmed ↗