Spontaneous Regression of Pediatric Osteochondroma: Clinical Case and Comprehensive Literature Review
Kazu Matsumoto, Daichi Ishimaru, Kazuki Sohmiya, Nobuo Terabayashi

TL;DR
A child's benign bone tumor spontaneously regressed over six years, a rare occurrence that may avoid surgery in similar cases.
Contribution
This paper presents a rare case of spontaneous regression in a pediatric osteochondroma and reviews existing literature to identify patterns and mechanisms.
Findings
Spontaneous regression occurred in a six-year-old with a solitary osteochondroma of the distal femur.
Regression was observed predominantly in skeletally immature males with solitary lesions.
Physeal remodeling is proposed as a likely mechanism for regression in such cases.
Abstract
Osteochondromas are the most common benign bone tumors in children, typically arising in the metaphyseal regions of long bones. While most lesions remain asymptomatic and stable, their natural history is not fully understood, and spontaneous regression is exceptionally rare. We present the case of a six-year-old boy with a solitary pedunculated osteochondroma of the distal femur who was managed conservatively. Initial radiographs demonstrated a stalk-like exostosis arising from the medial aspect of the distal femur without features of hereditary multiple exostoses. The patient remained clinically stable, and serial imaging revealed progressive reduction in tumor size, with marked regression noted at three years and near-complete resolution by six years. Throughout follow-up, the patient reported no pain or functional limitation. A review of 38 published cases, including the present…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
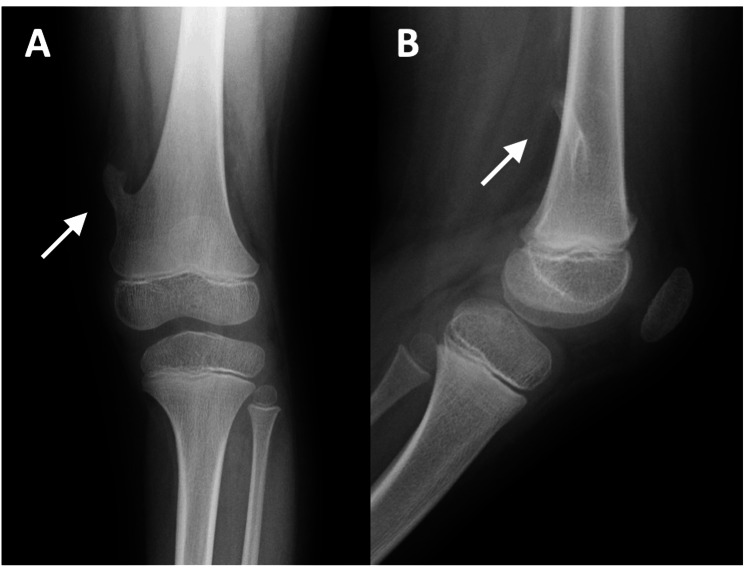 Figure 1
Figure 1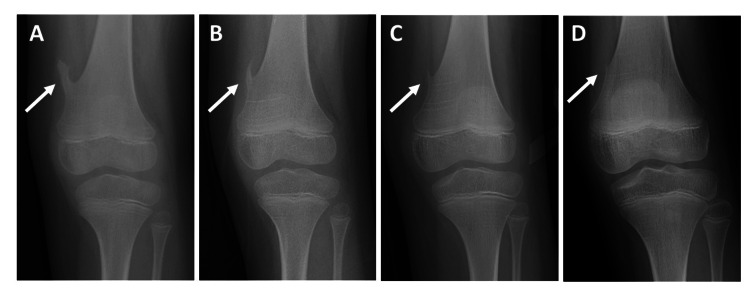 Figure 2
Figure 2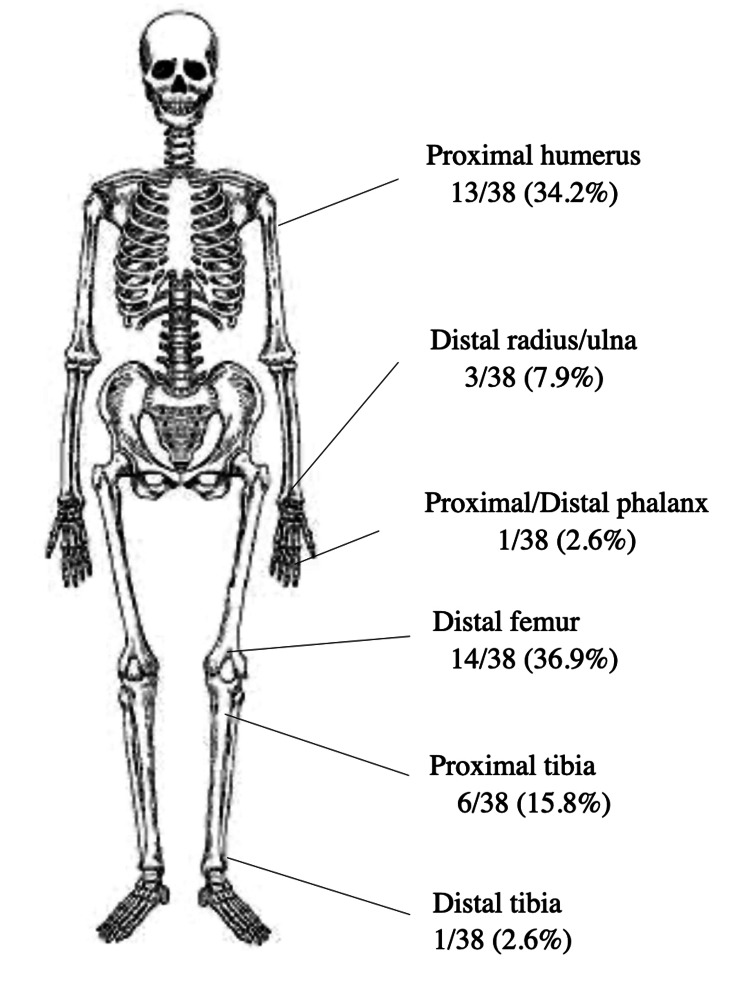 Figure 3
Figure 3| Case No. | Sex | Solitary or Multiple | Type of Osteochondroma | Location of the Lesion | Age at First Visit (yrs) | Time Until Regression (yrs) | Trauma | References |
| 1 | M | Solitary | Pedunculated | Distal femur | 6 | 6 | No | Our case |
| 2 | M | Solitary | Pedunculated | Proximal humerus | 16 | 1.5 | Yes | Moghamis IS et al. [ |
| 3 | M | Solitary | Pedunculated | Proximal tibia | 6 | 6 | No | Adachi R et al. [ |
| 4 | M | Solitary | Pedunculated | Distal femur | 11 | 6 | No | Le HM et al. [ |
| 5 | M | Solitary | Sessile | Proximal humerus | 11 | 6 | No | Kalifis G Sr et al. [ |
| 6 | M | Solitary | Sessile | Distal femur | 4 | 3 | No | Durán-Serrano M et al. [ |
| 7 | M | Solitary | Sessile | Proximal humerus | 10 | 3 | No | - |
| 8 | M | Solitary | Pedunculated | Proximal humerus | 11 | 4 | No | - |
| 9 | M | Solitary | Sessile | Distal femur | 1.3 | 0.5 | Yes | Heyworth PB et al. [ |
| 10 | M | Solitary | Pedunculated | Distal femur | 16 | 3 | No | Aiba H et al. [ |
| 11 | M | Solitary | Sessile | Distal femur | 7 | 5 | No | - |
| 12 | M | Solitary | Sessile | Distal femur | 6 | 2 | No | Hill CE et al. [ |
| 13 | M | Solitary | Sessile | Proximal humerus | 6 | 3 | No | Passanise AM et al. [ |
| 14 | M | Solitary | Sessile | Proximal humerus | 7 | 5 | No | - |
| 15 | M | Solitary | Sessile | Proximal humerus | 10 | 2.5 | No | - |
| 16 | M | Solitary | Sessile | Distal femur | 12 | 4 | No | - |
| 17 | F | Solitary | Pedunculated | Proximal tibia | 9 | 9 | No | Mahmoodi SM et al. [ |
| 18 | F | Solitary | Sessile | Distal femur | 9 | 4 | No | Valdivielso-Ortiz A et al. [ |
| 19 | F | Solitary | Sessile | Distal tibia | 6 | 2 | No | Minami S et al. [ |
| 20 | M | Multiple | Sessile | Proximal tibia | 7 | 14 | No | Yasuda H et al. [ |
| 21 | M | Solitary | Pedunculated | Proximal humerus | 7 | 1.25 | No | Hoshi M et al. [ |
| 22 | F | Solitary | Pedunculated | Distal femur | 12 | 6 | No | Arkader A et al. [ |
| 23 | M | Solitary | Sessile | Distal femur | 12 | 0.16 | No | Choi JY et al. [ |
| 24 | M | Solitary | Pedunculated | Distal femur | 15 | 4 | No | Reston SC et al. [ |
| 25 | M | Solitary | Sessile | Distal radius | 7 | 1.5 | No | Yanagawa T et al. [ |
| 26 | M | Solitary | Sessile | Proximal phalanx | 3 | 6 | No | Yamamoto T et al. [ |
| 27 | F | Solitary | Sessile | Proximal humerus | 9 | 5 | No | Revilla Y et al. [ |
| 28 | M | Solitary | Sessile | Distal ulna | 7 | 0.5 | No | Claikens B et al. [ |
| 29 | F | Solitary | Sessile | Proximal humerus | 5 | 2 | No | Castriota-Scanderbeg A et al. [ |
| 30 | M | Solitary | Sessile | Distal radius | 12 | 1 | Yes | - |
| 31 | M | Solitary | Pedunculated | Proximal tibia | 10 | 3 | No | Montgomery DM and LaMont RL [ |
| 32 | M | Solitary | Sessile | Proximal humerus | 11 | 5.5 | No | - |
| 33 | M | Solitary | Sessile | Distal femur | 11 | 2 | Yes | Copeland RL et al. [ |
| 34 | M | Solitary | Pedunculated | Distal femur | 10 | 2.5 | Yes | - |
| 35 | M | Solitary | Pedunculated | Proximal tibia | 9 | 1 | No | Paling MR [ |
| 36 | M | Solitary | Sessile | Proximal humerus | 6 | 6 | No | Merle P et al. [ |
| 37 | F | Solitary | Sessile | Proximal humerus | 5 | 1 | No | Callan JE et al. [ |
| 38 | M | Solitary | Sessile | Proximal tibia | 8.5 | 3.5 | No | Sellink JL [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Oral and Maxillofacial Pathology · Sarcoma Diagnosis and Treatment
Introduction
Osteochondromas are the most common benign bone tumors, accounting for up to 35% of all benign bone lesions [1,2]. They are classified as sessile, with a broad base, or pedunculated, with a narrow stalk [1]. Despite their prevalence, the natural history of osteochondromas remains poorly understood, as most lesions are asymptomatic and spontaneous regression is exceedingly rare.
Herein, we describe a rare case of near-complete spontaneous regression of a solitary pedunculated osteochondroma of the distal femur in a child. Importantly, we complement this case with a comprehensive literature review of all previously reported cases of regressed osteochondromas, thereby providing the most updated and systematic overview of this phenomenon. Recognition of this potential outcome is crucial to avoid unnecessary surgical intervention in children.
Case presentation
A 6-year-old boy presented with a solitary mass around his left knee, associated with mild tenderness for several months. There was no history of trauma, systemic symptoms, or significant past medical conditions, aside from birth palsy of the right upper extremity.
On examination, a firm, mildly tender, non-adherent mass was palpable over the anteromedial aspect of the distal femur. The knee had a full range of motion, with intact neurovascular function, and no additional masses were found.
Plain radiographs revealed a pedunculated osteochondroma with a long stalk arising from the medial aspect of the distal femur (Figures 1A-1B). Features of hereditary multiple exostoses were absent. After multidisciplinary discussion with the family, conservative observation was chosen.
Radiographs of the osteochondroma at presentation.(A) Anteroposterior view and (B) lateral view showing a pedunculated osteochondroma with a long stalk arising from the medial aspect of the distal femur.
At the 1-year follow-up, radiographs showed a slight reduction in the size of the osteochondroma (Figure 2A). At the 3-year follow-up, a significant reduction in tumor size was observed (Figure 2B). By 4 years, marked regression of the tumor was evident (Figure 2C). At the 6-year follow-up, near-complete regression of the lesion was demonstrated (Figure 2D), and the patient remained asymptomatic. Written informed consent for publication, including radiographs, was obtained from the patient’s parents.
Radiographic course of spontaneous regression.(A) One-year follow-up radiograph showing a slight reduction in the osteochondroma. (B) Three-year follow-up radiograph showing a significant reduction in tumor size. (C) Four-year follow-up radiograph showing marked regression of the tumor. (D) Six-year follow-up radiograph demonstrating near-complete regression of the lesion.
Discussion
Spontaneous regression of osteochondromas is exceptionally rare. The first case was described by Hunter J in 1835 [3]. Between 1960 and 2011, 22 cases were reported [4], and since then, an additional 16 cases, including ours, have been identified [5-32]. The current review demonstrates that regression predominantly occurs in skeletally immature patients, particularly in boys, with the distal femur and proximal humerus being the most frequent sites. This distribution corresponds to the most common anatomical locations of osteochondromas in general.
We reviewed 38 reported cases of spontaneous regression of osteochondromas, including our case (Table 1). The majority occurred in males (76.3%) and as solitary lesions (97.4%). Sessile morphology accounted for 65.8%, while 34.2% were pedunculated. The anatomical distribution is summarized in Figure 3. The distal femur (36.9%) and proximal humerus (34.2%) were the most frequent sites, followed by the proximal tibia (15.8%). Less common sites included the distal radius, distal tibia, distal ulna, and proximal phalanx. The mean age at presentation was 9.8 years, and the mean regression period was 4.2 years. A history of trauma was reported in approximately 13.2% of cases.
Distribution of reported regression sites.Anatomical distribution of 38 reported cases of spontaneous regression of osteochondromas, highlighting the distal femur and proximal humerus as the most commonly affected sites.This figure was created by the authors using data aggregated from published cases [5-32].
Regression was more common in sessile lesions than in pedunculated ones (60.5% vs. 39.5%), although it can occur in both morphologies. The mean regression period was approximately four years, but individual cases varied widely, ranging from a few months to over a decade, highlighting variability in biological behavior. Trauma was reported in 10.5% of cases, supporting the hypothesis that fracture-related remodeling or vascular compromise may contribute to regression in some instances.
Three mechanisms of regression have been proposed: (1) physeal remodeling as the growth plate migrates away from the lesion [25, 26], (2) remodeling following fracture or vascular compromise [6, 7, 18], and (3) resorption due to pseudoaneurysm formation [20]. Our case most likely represents physeal remodeling, as there was no evidence of fracture or vascular injury.
The clinical implications of this review are significant. Since most regressing osteochondromas were asymptomatic and resolved without intervention, conservative management with long-term follow-up is a reasonable strategy in children, particularly for lesions in common sites such as the distal femur. Recognizing the potential for regression may help avoid premature or unnecessary surgical excision, which carries inherent risks of complications.
Conclusions
This case, together with a systematic review of 38 regressed osteochondromas, highlights that spontaneous regression, though rare, is a real and clinically significant phenomenon, particularly in children. Our report underscores the importance of long-term observation in selected asymptomatic cases and provides one of the most comprehensive updates on this topic in recent literature. Awareness of this natural course can help guide orthopedic surgeons toward more judicious treatment decisions and prevent unnecessary surgical interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Imaging of osteochondroma: variants and complications with radiologic-pathologic correlation Radiographics Murphey MD Choi JJ Kransdorf MJ Flemming DJ Gannon FH 14071434202000 https://pubs.rsna.org/doi/10.1148/radiographics.20.5.g 00se 171407?url_ver=Z 39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub 0pubmed 1099203110.1148/radiographics.20.5.g 00se 171407 · doi ↗ · pubmed ↗
- 2Osteochondromas: review of the clinical, radiological and pathological features In Vivo Kitsoulis P Galani V Stefanaki K Paraskevas G Karatzias G Agnantis NJ Bai M 633646222008 https://iv.iiarjournals.org/content/22/5/633.short 18853760 · pubmed ↗
- 3The Works of John Hunter: With Notes by JF Palmer Longmans, London,UK Hunter J London, UK Longmans 1885 https://books.google.co.jp/books?hl=ja&lr=lang_ja|lang_en&id=Uw QHAAA Ac AAJ&oi=fnd&pg=PR 1&dq=The+Works+of+John+Hunter,With+notes+by+JF+Palmer.+&ots=j PX Nq 46tcv&sig=Sf ZA Txlw 219X 8z 5l LO Zh CWDH Oe 8#v=onepage&q&f=false
- 4Regression of a sessile osteochondroma: a case study and review of the literature UPOJ Stitzman-Wengrowicz ML Pretell-Mazzini J Dormans JP Davidson RS 7376212011 https://www.researchgate.net/profile/Juan-Pretell-Mazzini/publication/267426996_Regression_of_a_Sessile_Osteochondroma_A_Case_Study_and_Review_of_the_Literature/links/548589 d 00cf 283750 c 372617/Regression-of-a-Sessile-Osteochondroma-A-Case-Study-and-Review-of-the-Literature.pdf
- 5Vanishing solitary osteochondroma of humerus following trauma: a case report Trauma Case Rep Moghamis IS Elramadi A Radi M Hejleh HA Mudawi A Elsayed AM 100874462023 https://www.sciencedirect.com/science/article/pii/S 235264402300122 X?via=ihub 3739611510.1016/j.tcr.2023.100874 PMC 10310942 · doi ↗ · pubmed ↗
- 6Thin cartilage cap may be related to the spontaneous regression in pediatric patients with osteochondroma Curr Oncol Adachi R Nakamura T Asanuma K Hagi T Uchiyama T Sudo A 98849890292022 https://www.mdpi.com/1718-7729/29/12/7773654719110.3390/curroncol 29120777 PMC 9777135 · doi ↗ · pubmed ↗
- 7Femoral injury over the site of spontaneous regression of an osteochondroma in a teenage athlete Curr Sports Med Rep Le HM Schwartz RB Corrado G 51851912021 https://journals.lww.com/acsm-csmr/fulltext/2021/10000/femoral_injury_over_the_site_of_spontaneous.7.aspx 10.1249/JSR.000000000000088934622815 · doi ↗ · pubmed ↗
- 8Minor shoulder injury reveals spontaneous regression of proximal humerus osteochondroma Cureus Kalifis G Sr Marin Fermin T Sr Konstantinou E Raoulis V Sr Hantes M Sr 0132021 https://www.cureus.com/articles/64300-minor-shoulder-injury-reveals-spontaneous-regression-of-proximal-humerus-osteochondroma 10.7759/cureus.16793 PMC 832884334354896 · doi ↗ · pubmed ↗