Extensive Odontogenic Buccal Space Infection With Multispace Extension in a Diabetic Elderly Patient: A Case Report
Sandeep Khandaitkar, Ramakrishna Shenoi, Anant Kahare, Teena Oommen

TL;DR
A diabetic elderly woman developed a severe facial infection from a tooth issue, highlighting the need for quick treatment in high-risk patients.
Contribution
This case report highlights the aggressive progression of odontogenic infections in diabetic patients and emphasizes multidisciplinary management.
Findings
The infection extended to multiple facial spaces with bone erosion and lymph node necrosis.
Treatment included drainage, tooth extraction, and intravenous antibiotics.
Early diagnosis and multidisciplinary care are critical for diabetic patients with such infections.
Abstract
Odontogenic infections are common in oral and maxillofacial practice but may progress rapidly in medically compromised individuals. Diabetes mellitus is a recognized risk factor, predisposing patients to severe and recurrent infections with poor healing potential. We report the case of a 70-year-old diabetic, hypertensive, and hypothyroid female who presented with a left buccal space infection extending to the submandibular, sublingual, and infratemporal spaces, complicated by cortical bone erosion and necrotic lymphadenitis. The patient was managed with incision and drainage, extraction of the offending teeth, and broad-spectrum intravenous antibiotics. This case underscores the aggressive nature of odontogenic infections in diabetic patients and emphasizes the importance of early diagnosis, prompt surgical drainage, systemic control, and multidisciplinary management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
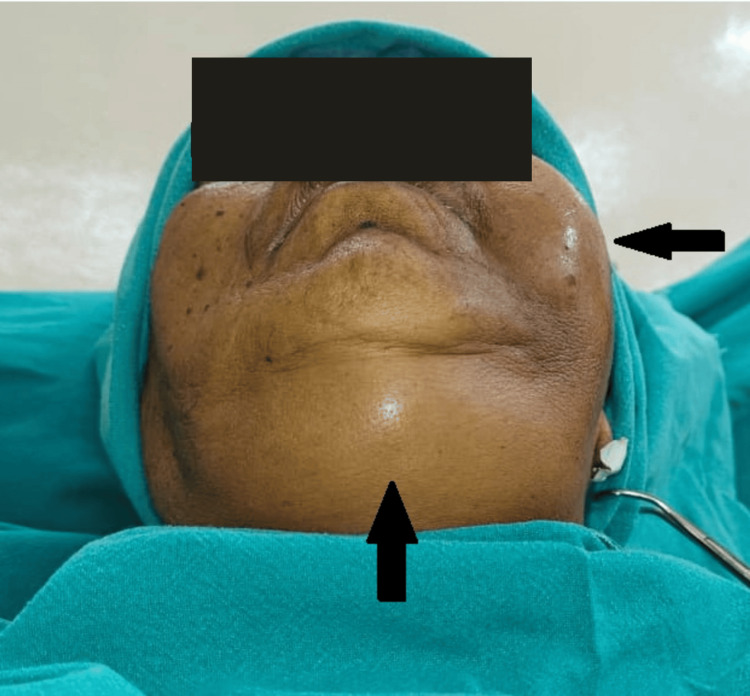 Figure 1
Figure 1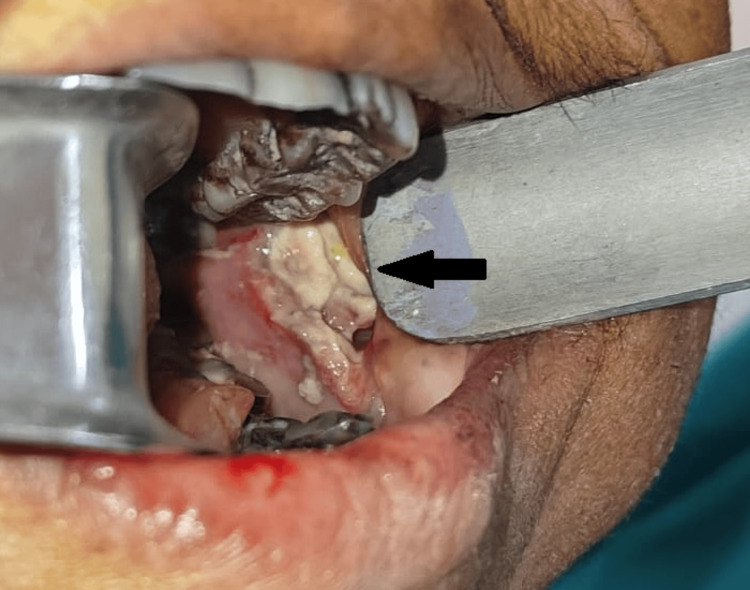 Figure 2
Figure 2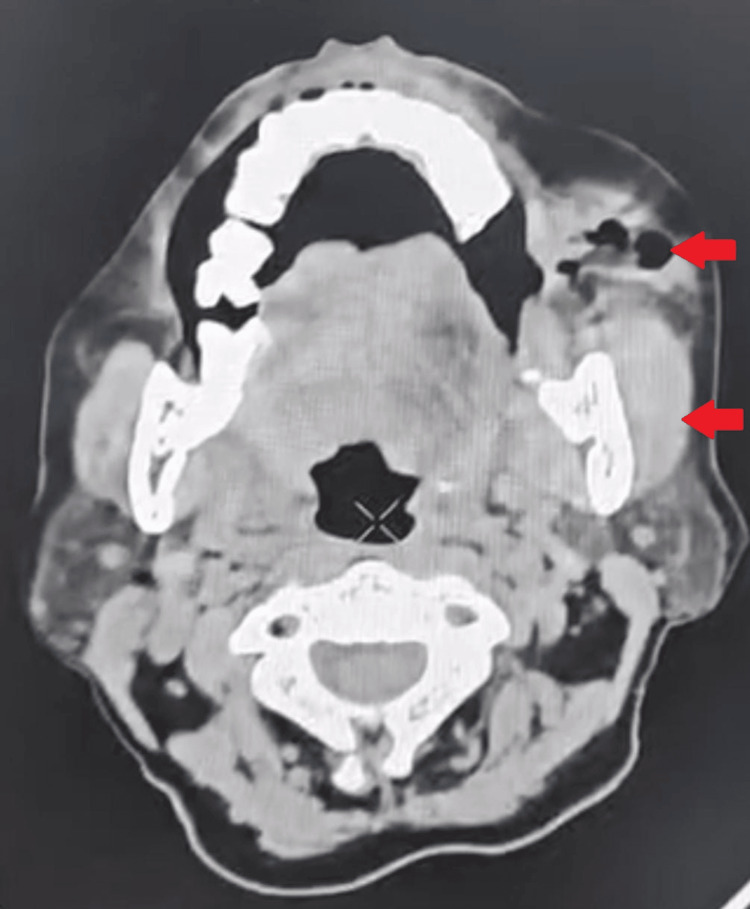 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5| Parameter | Patient’s result | Reference range | Unit | Interpretation |
| Hemoglobin | 9.9 | 12.0–16.0 | g/dL | ↓ Anemia |
| TLC | 18,000–22,000 | 4,000–11,000 | /mm³ | ↑ Leukocytosis |
| RBS | 166 | 70–140 | mg/dL | ↑ Hyperglycemia |
| HbA1c | 6.7 | <5.7 (normal), <7 (good control) | % | Borderline control |
| ALP | Mildly raised | 44–147 | IU/L | ↑ Mild elevation |
| Temperature | Afebrile | 36.5–37.5 | °C | Normal |
| Blood pressure | Stable | 90/60–120/80 | mmHg | Normal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOtolaryngology and Infectious Diseases · Salivary Gland Tumors Diagnosis and Treatment · Head and Neck Anomalies
Introduction
Odontogenic infections arise primarily from pulpal or periodontal pathology and can spread rapidly along fascial planes of the head and neck. While localized infections are usually controlled with drainage and antibiotics, systemic comorbidities such as diabetes mellitus significantly alter the host immune response. Diabetes impairs neutrophil chemotaxis, phagocytosis, and oxidative burst, leading to rapid progression and poor prognosis [1,2].
The most frequently involved fascial spaces include buccal, submandibular, and sublingual regions. However, untreated or aggressive cases may extend to secondary spaces such as infratemporal, parapharyngeal, and mediastinal regions, increasing morbidity and mortality [3,4]. Diabetic patients are especially predisposed because of impaired immunity and chronic low-grade inflammation, which further worsens healing capacity [5].
Chang et al. demonstrated that diabetic patients with odontogenic infections tend to present with more fascial space involvement, higher complication rates, and longer hospital stays compared to non-diabetic patients [6].
Case presentation
A 70-year-old female presented to the Department of Oral and Maxillofacial Surgery, Ranjeet Deshmukh Dental College and Research Centre, Nagpur, with complaints of swelling on the left side of the face for 8-10 days, gradually increasing in size despite prior oral antibiotics. She reported pain, pus discharge, and restricted mouth opening but denied fever, dysphagia, or voice change.
The patient gave a history of diabetes mellitus (20 years, controlled with oral hypoglycemics), hypertension, and hypothyroidism (controlled). The patient also had a habit of chronic areca nut chewing (30 years). She had been on long-term treatment with metformin 500 mg twice daily for diabetes, amlodipine 5 mg once daily for hypertension, and levothyroxine 75 µg once daily for hypothyroidism. The patient was admitted to the Department of Oral and Maxillofacial Surgery as the primary team. Given her comorbidities, concurrent consultation with the Department of Internal Medicine was obtained to optimize glycemic status and antihypertensive therapy.
Previous outpatient records of glycemic monitoring were available, showing an HbA1c value of 6.6% three months before admission. At the time of admission, laboratory investigations revealed an HbA1c of 6.7%. These findings, in conjunction with the elevated random blood sugar level of 166 mg/dL, suggested that the patient’s diabetes was moderately controlled with ongoing oral hypoglycemic therapy.
Clinical examination revealed a diffuse extraoral swelling ~11 × 8 × 3 cm with trismus (mouth opening of 1.5 fingers) (Figure 1).
Preoperative extraoral view showing diffuse swelling on the left side of the face and one finger below the lower border of the mandible crossing the midline.
Intraoral swelling measured 5 × 4 × 2 cm with whitish slough, pus discharge, and obliteration of the vestibule (Figure 2).
Intraoral view showing necrotic slough and pus discharge from the left buccal mucosa.
Multiple grossly carious teeth were noted. Laboratory investigations showed anemia, leukocytosis, and hyperglycemia (Table 1).
Contrast-enhanced CT revealed multispace involvement (buccal, submandibular, sublingual, infratemporal) with cortical bone erosion and necrotic lymphadenitis (Figure 3).
Contrast-enhanced CT revealed multispace involvement (buccal infratemporal).
Surgical management included intraoral and extraoral incision and drainage, removal of necrotic slough, and debridement of necrotic tissue (Figure 4).
Intraoperative view showing drainage.
Dependent drainage was achieved via a submandibular incision. The offending teeth 21-28 and 31-38 were extracted (Figure 5).
Extracted grossly carious and non-restorable teeth.
The patient was managed postoperatively with intravenous ceftriaxone and metronidazole, later escalated to piperacillin-tazobactam, along with supportive care and strict glycemic control. She improved gradually and was discharged after 23 days of hospitalization.
Discussion
Odontogenic infections are among the most common conditions encountered in oral and maxillofacial practice [1]. In immunocompetent individuals, these infections are usually localized, but in immunocompromised patients, particularly those with diabetes mellitus, the course is often aggressive with multispace involvement [2,3].
Diabetes mellitus is associated with altered innate immune responses [4]. Microvascular changes hinder perfusion and delay healing [5]. Chang et al. [6] showed that diabetic patients tend to present with more fascial space involvement, while Huang et al. [7] reported higher complication rates, including necrotizing fasciitis. The buccal space often serves as the initial site before extension to the submandibular and sublingual spaces [8]. Infratemporal spread increases the risk of cavernous sinus thrombosis and airway compromise. If untreated, odontogenic infections may progress to airway obstruction, descending necrotizing mediastinitis, or septicemia [9,10], with mortality especially high in diabetics [11].
Our patient demonstrated rapid progression of a buccal space infection into submandibular, sublingual, and infratemporal spaces, with radiological evidence of cortical erosion and necrotic lymphadenitis. The differential diagnoses considered included suppurative odontogenic cellulitis and deep neck infections of non-odontogenic origin, such as salivary gland suppuration or tuberculous lymphadenitis. Odontogenic cellulitis was excluded as imaging revealed multiple loculated abscesses with cortical bone erosion rather than diffuse soft tissue swelling. Non-odontogenic deep neck infections were also ruled out, as the infection was clearly contiguous with grossly carious teeth and responded well to extraction and surgical drainage.
Management principles include elimination of the source, surgical drainage, and systemic antibiotic therapy [1,2]. In this case, multiple decayed teeth were extracted, drainage was established, and intravenous antibiotics were escalated according to clinical response [12,13]. Supportive measures, particularly strict glycemic control, were critical. Adjuncts such as negative-pressure wound therapy and culture-guided antibiotics improve prognosis [14].
This case is significant because it demonstrates uncommon severity, emphasizes the need for vigilance in diabetics, highlights educational value for clinicians, and underlines global importance given rising diabetes prevalence [15,16].
Conclusions
Odontogenic infections in elderly diabetic patients can progress rapidly with multispace extension and bone destruction. Early recognition, prompt surgical drainage, removal of the odontogenic foci, and broad-spectrum intravenous antibiotics, alongside strict systemic control, are key. This case demonstrates how a common dental infection can evolve into a severe, life-threatening condition in the presence of diabetes mellitus.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Severe odontogenic infections, part 1: prospective report J Oral Maxillofac Surg Flynn TR Shanti RM Levi MH Adamo AK Kraut RA Trieger N 109311036420061678134310.1016/j.joms.2006.03.015 · doi ↗ · pubmed ↗
- 2Surgical management of orofacial infections Atlas Oral Maxillofac Surg Clin North Am Flynn TR 7710082000 https://pubmed.ncbi.nlm.nih.gov/11212388/11212388 · pubmed ↗
- 3Microbiology and management of deep facial infections and Lemierre syndrome ORL J Otorhinolaryngol Relat Spec Brook I 1171206520031282473410.1159/000070776 · doi ↗ · pubmed ↗
- 4Infections in patients with diabetes mellitus N Engl J Med Joshi N Caputo GM Weitekamp MR Karchmer AW 1906191234119991060151110.1056/NEJM 199912163412507 · doi ↗ · pubmed ↗
- 5Low-grade inflammation in chronic infectious diseases: paradigm of periodontal infections Ann N Y Acad Sci Moutsopoulos NM Madianos PN 251264108820061719257110.1196/annals.1366.032 · doi ↗ · pubmed ↗
- 6Automated continuous distraction osteogenesis may allow faster distraction rates: a preliminary study J Oral Maxillofac Surg Peacock ZS Tricomi BJ Murphy BA Magill JC Kaban LB Troulis MJ 107310847120132349915910.1016/j.joms.2012.11.015PMC 3660410 · doi ↗ · pubmed ↗
- 7Virtual endoscopy of laryngeal carcinoma: is it useful?Otolaryngol Head Neck Surg Magnano M Bongioannini G Cirillo S 77678213220051588663410.1016/j.otohns.2005.01.031 · doi ↗ · pubmed ↗
- 8Cervicofacial infection of dental origin presenting to maxillofacial surgery units in the United Kingdom: a national audit Br Dent J Carter LM Layton S 737820620091916526210.1038/sj.bdj.2009.4 · doi ↗ · pubmed ↗