Variability in Clinical Response to Steroids in Granulomatous Mastitis: A Report of Two Cases
Karla V Corona-López, Monserrat Sánchez-Romero, Valeria B Fernández-Rodríguez, Ana K Barba-Rojas, Alejandro Rendón-Molina

TL;DR
This paper reports two cases of a rare breast disease showing different responses to steroid treatment, highlighting the need for personalized treatment approaches.
Contribution
The study emphasizes variable steroid responses in granulomatous mastitis and proposes individualized treatment strategies based on disease extent and phenotype.
Findings
One patient had partial response and frequent relapses despite prolonged steroid treatment.
Another patient achieved complete remission with a low-dose steroid regimen and no recurrences.
Abstract
Idiopathic granulomatous mastitis (IGM) is a rare, benign, chronic inflammatory breast disease that primarily affects premenopausal women, often in the postpartum period or after breastfeeding. Its nonspecific clinical and imaging presentation, frequent overlap with infectious and neoplastic conditions, and variable therapeutic response make both diagnosis and management challenging. This report aims to describe the clinical characteristics, diagnostic approach, and corticosteroid response in two histologically confirmed cases, highlighting differences in therapeutic outcomes and the relevance of individualized regimens. Both patients presented with chronic inflammatory breast lesions unresponsive to antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs), requiring corticosteroid therapy for disease control. One case showed partial response with frequent relapses despite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
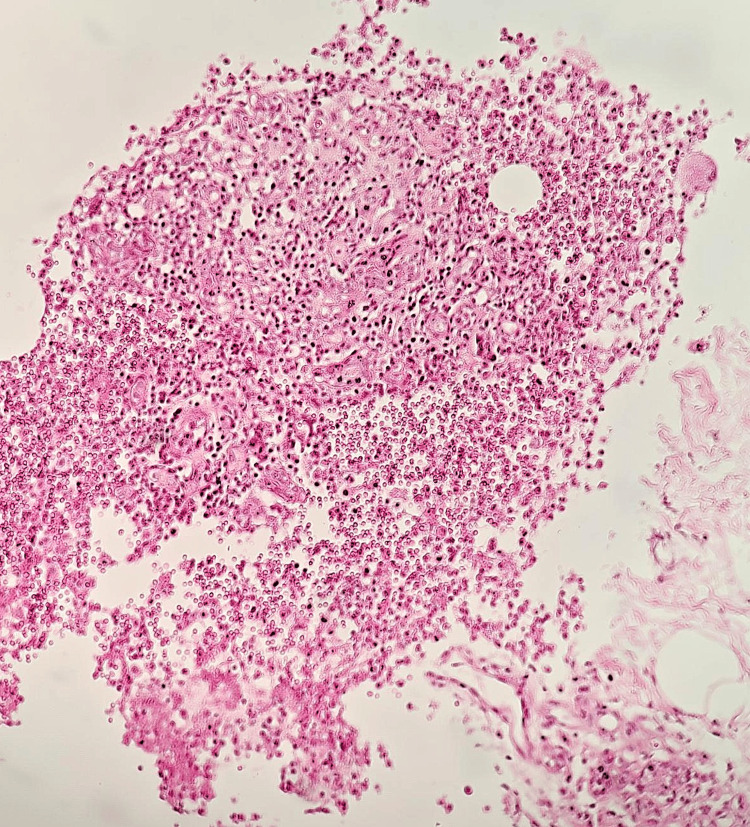 Figure 1
Figure 1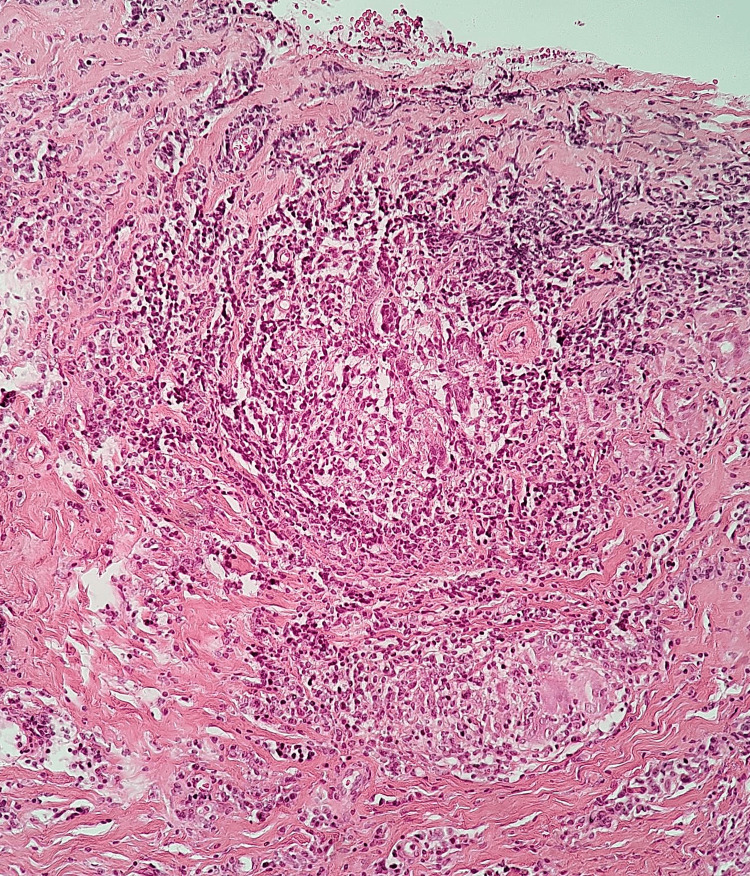 Figure 2
Figure 2| Variable | Patient one | Patient two |
| Age at diagnosis | 40 years | 47 years |
| Comorbidities | Obesity grade II, uterine fibroids | Obesity grade III, uterine fibroids, chronic venous insufficiency |
| Affected side | Initially right breast, later bilateral | Left breast only |
| Diagnosis by biopsy | Xanthogranulomatous mastitis with reactive atypia | Chronic granulomatous mastitis, negative stains |
| Initial dose | Prednisone 5 mg PO every 24 hours | Prednisone 5 mg PO every 24 hours |
| Treatment course | Increased to 20 mg in January 2025 due to recurrences; tapered to 10 mg | Gradual taper: 5 mg → 2.5 mg every 48 hours; discontinued in June 2024 |
| Total duration of steroid therapy | >1 year (ongoing) | <8 months |
| Clinical response | Partial, with frequent relapses and need for drainage | Sustained complete response |
| Need for dose adjustment due to relapse | Yes – increased to 20 mg, then adjusted to 10 mg | No – progressive tapering without flares |
| Suggested escalation | Yes – candidate for immunosuppressants (e.g., methotrexate) | Not required |
| Current status | Active disease, on 10 mg PO | Discharged from follow-up since January 2025 |
| Treatment type | Average dose used | Approximate duration | Remission rate (%) | Relapse rate (%) |
| Oral steroids (prednisone) | 0.5–1 mg/kg/day (e.g., 20–50 mg/day) | 6–12 weeks or longer | 70–80% | 30–40% |
| Tapered oral regimen (Montazer) | 50 → 25 → 12.5 → 5 mg every 2 weeks | 2 months | 93% | 0% |
| With methotrexate (MTX) | MTX 7.5–25 mg/week + prednisone | Induction: 3–6 months | 90–95% | <10% |
| With azathioprine (AZA) | AZA 50–100 mg/day ± prednisone | Maintenance: ≥6 months | 95.3% | 4.7–9.1% |
| Intralesional steroids | Triamcinolone 10–40 mg/injection (1–4 sessions) | 1–3 months | 71.9–93.5% | 8.7–46.9% |
| Antibiotics only (inadequate management) | Dicloxacillin, TMP-SMX (no steroids) | Variable, ineffective | Low (<30%) | High (>60%) |
| Surgery as first-line treatment | Resection or surgical drainage | — | <60% | 66.1% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Cancer and Skin Lesions · Metastasis and carcinoma case studies
Introduction
Idiopathic granulomatous mastitis (IGM) is a rare, benign, chronic inflammatory disease of the mammary gland. It primarily affects premenopausal women, often in the context of the puerperium or following breastfeeding. Clinically, it may mimic common breast infections or even inflammatory breast cancer, making initial diagnosis particularly challenging [1]. Given that idiopathic granulomatous mastitis frequently affects women in the postpartum period, therapeutic strategies must also consider breastfeeding safety. Corticosteroids such as prednisone are generally considered compatible with breastfeeding in low-to-moderate doses; however, prolonged or high-dose regimens may still represent a challenge, requiring individualized planning [2].
The clinical importance of reporting IGM cases lies in their low prevalence, non-specific presentation, and often relapsing course, which together complicate their management. Although no standardized treatment protocol exists, available therapeutic strategies include nonsteroidal anti-inflammatory drugs (NSAIDs), antibiotics, systemic corticosteroids, immunosuppressants, and surgery. Emerging therapies such as intralesional steroid administration are still under investigation regarding their efficacy [3].
In the two cases presented here, diagnosis was hindered by atypical clinical progression, poor response to conventional antibiotic and anti-inflammatory therapy, and inconclusive imaging findings. In one case, the disease manifested bilaterally and relapsed repeatedly, with multiple abscesses and drainage, and no improvement until corticosteroid therapy was initiated. In the other, a suspected but later ruled out association with tuberculous mastitis added complexity to the diagnostic process and delayed definitive treatment. Both cases demonstrate that without prompt and sustained steroid use, clinical improvement would not have been achieved [2].
The aim of this report is to describe the clinical characteristics, diagnostic challenges, and therapeutic response in two cases of idiopathic granulomatous mastitis managed at the Instituto Nacional de Perinatología between March 2023 and April 2025, highlighting the crucial role of systemic corticosteroids in disease resolution and thereby strengthening clinical understanding, particularly in settings with suspected infectious or atypical etiology.
Case presentation
Case one: torpid evolution and partial response to steroids
A 40-year-old female, G4 C2 P2, with a history of grade II obesity and uterine fibroids, and no autoimmune background, presented in October 2023 with severe right breast pain (visual analogue scale (VAS) 8/10) and progressive inflammation. Physical examination revealed a non-adherent mass and a mobile axillary lymph node. Initial anti-inflammatory management showed no response; antibiotics were escalated, and a spontaneously draining abscess was later documented.
By January 2024, the clinical picture extended to the left breast, with pain, pruritus, and induration. A 62 × 40 mm mass was documented. Biopsy revealed a xanthogranulomatous inflammatory process with reactive epithelial atypia. Oral prednisone at 5 mg/day was initiated, increasing to 20 mg/day in January 2025 due to persistent inflammatory lesions and symptoms. Since April, she has been maintained on 10 mg/day.
Throughout this period, the patient required multiple antibiotic regimens (dicloxacillin, trimethoprim/sulfamethoxazole (TMP/SMX)) and ambulatory drainages in both breasts. Clinical response has been partial, with intermittent symptomatic improvement but frequent recurrences, particularly in the left breast. The most recent episode occurred in April 2025, presenting as spontaneous drainage from an indurated area. This clinical course suggests possible corticosteroid resistance. At the time of the last follow-up, the patient was asymptomatic, under treatment with prednisone 10 mg/day and close surveillance.
Case two: clinical control with low-dose steroids and no relapses
A 47-year-old female, G3 C3, with grade III obesity, uterine fibroids, and chronic venous insufficiency, presented in March 2023 with a mass and pain in the left breast. She was initially treated as a breast abscess with antibiotics, and a core needle biopsy reported fibrocystic mastopathy. Due to persistent symptoms, a second biopsy was performed, confirming chronic granulomatous mastitis with negative special stains (Ziehl-Neelsen, Grocott, PAS staining).
In October 2023, treatment with oral prednisone 5 mg once daily was initiated, accompanied by dicloxacillin for four weeks. The patient showed progressive improvement, documented by imaging studies reporting a reduction in fluid collections and resolution of the inflammatory process (Breast Imaging Reporting and Data System (BI-RADS) 2-3). By January 2024, she was clinically asymptomatic.
Over the following months, the steroid dose was gradually tapered to 2.5 mg orally every 48 hours, achieving complete withdrawal in June 2024. No relapses or need for additional antibiotics were documented. In January 2025, the patient was discharged due to sustained clinical remission. This case stands out for its excellent response to low-dose glucocorticoid therapy, without requiring escalation to immunosuppressive agents.
Clinical and histological findings of both cases are summarized in Table 1, accompanied by representative histological images illustrating granulomatous inflammation and cellular features from each patient (Figures 1, 2).
Case one histological section showing mixed inflammatory infiltrate with neutrophil-rich microabscesses and evolving granulomas, consistent with suppurative granulomatous mastitis
Case two representative histological section showing a well-formed non-caseating granuloma with epithelioid cells, multinucleated giant cells, and surrounding lymphocytic inflammation
Discussion
Idiopathic granulomatous mastitis (IGM) represents a clinical challenge due to its chronic course, non-specific presentation, and variable therapeutic response. In the absence of standardized guidelines, its approach and management have been based on observational studies and individualized decisions, as demonstrated in the two cases presented [1-3].
From a pathophysiological standpoint, several hypotheses have been proposed to explain its origin, including autoimmune, infectious, hormonal mechanisms, and alterations in the breast microbiome [4]. The autoimmune hypothesis is the most widely accepted, supported by similarities with other granulomatous diseases such as thyroiditis or prostatitis, and by the favorable response to corticosteroids [4]. Associations with breastfeeding have also been described, attributed to increased permeability of the lactiferous ducts due to chemical or physical stimuli, although these mechanisms are still under investigation. Hyperprolactinemia is another proposed etiological factor and has justified the use of bromocriptine in selected cases [1].
Clinically, IGM presents with pain, inflammatory nodules, erythema, and occasionally abscesses or fistulas. Although typically unilateral, bilateral forms have been reported in 1-8% of cases [1]. Its course is chronic, with frequent recurrences, and it often requires surgical incision or drainage due to poor response to conventional antibiotic therapy [1,4].
Differential diagnosis
IGM is a benign inflammatory breast disease that poses a considerable diagnostic challenge due to its non-specific clinical and imaging features. Given its low prevalence and the absence of universal diagnostic criteria, IGM is largely a diagnosis of exclusion, based on the integration of clinical findings, imaging studies, and especially histopathological analysis [5]. Below are the main conditions to consider in the differential diagnosis of IGM.
Breast Abscess
Breast abscess, of infectious etiology, is a common cause of acute breast inflammation. Clinically, it can mimic IGM, presenting with pain, erythema, a palpable mass, and fever [3]. However, it typically responds well to antibiotics and drainage. On imaging, it appears as a well-defined anechoic collection, in contrast to the irregular hypoechoic lesions seen in IGM [3]. A positive culture and the presence of purulent necrosis are distinguishing features of abscesses.
Tuberculous Mastitis
Tuberculous mastitis (TM) should be considered particularly in endemic regions or immunocompromised patients. TM has a specific infectious etiology, with distinctive histological findings such as caseating necrosis and acid-fast bacilli on Ziehl-Neelsen staining [6]. In contrast, IGM presents with non-caseating granulomas and no evidence of mycobacteria. Since the treatment of TM requires antituberculous therapy, accurate differentiation is essential [3].
Inflammatory Breast Carcinoma
Inflammatory breast carcinoma represents one of the most relevant and complex differential diagnoses for IGM, due to the significant overlap in clinical and radiologic features. Studies indicate that in up to 50% of IGM cases, the initial suspected diagnosis is breast cancer, given the severity of clinical presentation and imaging findings [7,8]. On mammography or ultrasound, IGM may present as a spiculated, hypoechoic lesion with irregular margins or architectural distortion-features corresponding to BI-RADS categories 4 or 5. The literature emphasizes the need for histopathological confirmation [3].
Benign Breast Tumors
Benign tumors, such as fibroadenomas or adenomas, may be mistaken for IGM when presenting as palpable masses. Clinically, benign tumors are typically painless, mobile, well-circumscribed, and without inflammatory signs. Biopsy is essential, as cytology has low sensitivity for IGM (<20%) and may be confused with reactive processes in complex benign tumors [8].
Other Entities
Less common conditions to consider include mammary sarcoidosis, foreign body reactions (from implants or trauma), fungal infections (e.g., histoplasmosis), duct ectasia, and rheumatologic diseases such as granulomatosis with polyangiitis, giant cell arteritis, or polyarteritis nodosa.
It is important to note that various studies have reported a higher incidence of IGM in Hispanic and Latin American women compared to Caucasian or African American women [5,9].
Evidence of steroid management in granulomatous mastitis
The main objectives of steroid treatment are to control active inflammation, prevent recurrences, and reduce sequelae such as persistent pain and breast fibrosis, which negatively impact patients' quality of life [10]. Although spontaneous resolution has been documented in up to 50% of mild cases within a period of 6 to 24 months, expectant management is rarely adequate for moderate or severe symptoms. In these cases, the rational use of NSAIDs and antibiotics may offer temporary relief in the presence of superinfection, but they do not replace immunosuppression with steroids [1].
In the clinical cases analyzed, the use of prednisone was crucial for achieving symptom control. Patient one started with 5 mg daily, with progressive escalation to 20 mg/day due to frequent relapses. She was subsequently titrated to 10 mg daily, without achieving complete remission. In contrast, patient two followed a more conservative regimen with progressive adjustments and complete discontinuation at month nine, achieving sustained remission. In both patients, response was assessed by clinical improvement (pain, suppuration, resolution of abscesses) and imaging findings (reduction of collections and residual fibrosis).
Clinical experience and the literature agree that systemic steroids constitute the first-line therapy for moderate to severe IGM, with response rates of 70-80%, although recurrences are reported in 30-40% [1,11]. The recommended starting dose of prednisolone ranges from 0.5 to 1 mg/kg/day, with progressive reduction over at least 6 to 12 weeks [5]. This raises the question of whether the regimen used in patient one was insufficient. The trial by Montazer et al. demonstrated that a stepped regimen (50-25-12.5-5 mg for two months) achieved a higher remission rate (93% vs. 53%) and lower recurrence (0% vs. 37.5%) than a sustained low-dose regimen, suggesting that an aggressive initial approach could prevent early recurrences in more severe cases [12].
This finding is even more relevant considering that patient one presented with a bilateral form, a rare clinical manifestation documented in only two of 41 patients in a 10-year retrospective study [13]. This more extensive and symmetrical presentation could represent a more inflammatory phenotype or even a more resistant variant of the disease's clinical spectrum, which would explain its poor response to conventional regimens. The literature has suggested that bilateral forms or those with multiple affected areas often require higher doses and prolonged immunosuppression regimens to prevent relapse [1]. Patient two, with a unifocal presentation and less intense symptoms, achieved remission with a less aggressive regimen. This contrast suggests that the inflammatory phenotype and extent of breast involvement significantly modulate the response to immunosuppressive treatment.
This discrepancy also highlights that demographic factors such as age or obesity grade are not necessarily decisive predictors of therapeutic outcome in idiopathic granulomatous mastitis. Instead, recent studies indicate that the extent of breast involvement and the presence of bilateral or recurrent lesions are more closely associated with poor steroid responsiveness [13]. In our series, case one showed a bilateral and relapsing course with abscess formation, features commonly linked to resistance and frequent relapses, whereas case two exhibited a localized, unifocal presentation that allowed complete control with a low-dose tapered regimen. Furthermore, although obesity represents a relevant comorbidity for long-term metabolic risks, its impact on steroid response in IGM has not been consistently demonstrated [7]. These observations support the notion that the initial inflammatory burden and disease extent are more decisive than demographic characteristics in determining therapeutic success. Therefore, personalizing the therapeutic regimen is vitally important, avoiding the indiscriminate application of standard regimens that may be insufficient in some cases or excessive in others. The initial inflammatory burden, lesion size, and the presence of collections should guide both the initial dose and the rate of steroid tapering.
A central aspect in the management of IGM is the recurrence rate after steroid discontinuation or reduction. In a cohort study of 505 patients, it was found that those treated with corticosteroids alone had a 28.8% recurrence rate, significantly higher compared to those receiving immunosuppressants such as azathioprine, either as monotherapy (4.7%) or in combination with steroids (9.1%) [14]. These data reinforce the notion that combined immunosuppression not only enhances remission but also prolongs its duration.
Methotrexate has also demonstrated efficacy as a steroid-sparing therapy. In a Latin American series, three patients achieved complete remission with a regimen of prednisone induction and MTX maintenance, without serious adverse events [15]. Furthermore, other studies have indicated that MTX allows for more rapid reduction of steroid doses, with a lower risk of side effects such as hyperglycemia, weight gain, or insomnia, which significantly improves therapeutic adherence.
On the other hand, early surgical treatment, although tempting for persistent lesions or complex abscesses, has shown a higher recurrence rate. In an analysis of 120 patients, those who underwent surgery as first-line treatment had a recurrence rate of 66.1%, significantly higher than those treated with steroids alone or in combination with immunosuppressants [16]. This finding suggests that surgery should be strictly reserved for refractory cases, with close postoperative follow-up.
In recent years, intralesional steroids have gained popularity as an effective and less toxic alternative. A systematic review of nine studies including 474 patients demonstrated remission rates comparable to systemic steroids, but with a lower incidence of adverse effects and, in many cases, lower recurrence [17]. This approach offers a viable option for patients with localized disease or comorbidities that contraindicate systemic immunosuppression. An additional study of 78 patients showed that treatment with intralesional steroids combined with topical steroids achieved significantly higher remission rates than oral steroids (93.5% vs. 71.9%), with lower recurrence rates (8.7% vs. 46.9%) and less need for surgery (2.2% vs. 9.4%) [18]. These findings promote the use of local approaches as first-line treatment in selected patients.
Furthermore, the coexistence of systemic manifestations, such as arthritis, has been described in patients with GIM. A case series documented that the use of MTX or AZA not only controlled mastitis but also associated joint symptoms, suggesting a systemic autoimmune nature of the disease in some cases [19]. This finding warrants a comprehensive rheumatologic evaluation in recurrent cases or those with extraparenchymal symptoms.
Even in cases resistant to conventional steroids and immunosuppressants, successful alternative therapies have been described. Mycophenolate mofetil, for example, achieved complete resolution in a patient with IGM refractory to multiple lines of therapy, opening a new avenue for the treatment of severe or resistant forms.
Finally, the identification of Corynebacterium kroppenstedtii in breast abscesses has raised the hypothesis of an underlying infectious component. In a series of cases, the targeted use of antibiotics such as teicoplanin allowed remission without the need for immunosuppression, highlighting the importance of performing adequate cultures before initiating steroids, especially in regions with a high prevalence of tuberculosis or chronic infections [20].
Current evidence strongly supports the use of steroids as a therapeutic base for IGM, but cautions that their efficacy depends on the inflammatory phenotype, extent of involvement, and the regimen used. Combined use with immunosuppressants reduces relapses and allows for steroid dose reduction. The intralesional route is emerging as an effective option with lower toxicity. These findings underscore the need for individualized therapeutic strategies and the generation of local evidence to guide decisions in specific contexts such as Mexico.
Predisposition to the development of malignant breast tumors
Regarding oncological risk, there is no direct or sufficient evidence to propose a causal relationship between IGM and an increased incidence of breast cancer [2,4]. It has been suggested that alterations in the breast microbiome and deterioration of the extracellular matrix could be involved in cellular transformation, although these mechanisms remain under investigation [1,4].
Challenges in idiopathic granulomatous mastitis
The diagnosis of idiopathic granulomatous mastitis (IGM) remains a clinical challenge due to its non-specific presentation and the need to exclude other infectious or neoplastic entities before starting immunosuppressive treatment. The prolonged clinical course, variable responses to treatment, and the absence of specific biomarkers make timely diagnosis difficult, which can delay appropriate management and worsen the inflammatory process. In contexts with diagnostic and therapeutic limitations, such as Mexico, the lack of standardized clinical guidelines requires individualized treatment. Evidence suggests that the Mexican population presents a clinical course similar to that reported in other countries, highlighting the need to generate local evidence that allows international therapeutic regimens to be adapted to our clinical and epidemiological conditions [19].
Report limitations
This report presents limitations inherent to its descriptive and retrospective design. Because it deals with only two clinical cases, it is not possible to generalize about the efficacy of steroid treatment in IGM. Furthermore, clinical outcome was assessed qualitatively, without objective scales, which introduces interpretation bias. There were no standardized dosing protocols or defined discontinuation criteria, reflecting both a limitation of the study and of the current clinical approach. Finally, follow-up was limited to the period documented in the medical record, preventing the evaluation of relapses or long-term adverse effects.
Clinical implications and management recommendations in our population
These findings illustrate the heterogeneity in therapeutic response among patients with idiopathic granulomatous mastitis (Table 2). Corticosteroids remain the preferred first-line therapy, while immunosuppressive agents such as methotrexate may be considered in cases of recurrence or corticosteroid resistance. Surgical intervention is generally reserved for persistent or complicated cases. Tailoring treatment to the clinical presentation may help optimize remission rates and reduce recurrences.
Conclusions
These cases contribute significantly to the clinical understanding of granulomatous mastitis by demonstrating the diagnostic complexity when it presents in immunocompromised patients, especially with suspected mammary tuberculosis. Although both entities are rare, their overlap can generate diagnostic uncertainty and delay therapeutic decisions.
The difficulty in distinguishing between idiopathic granulomatous mastitis and mammary tuberculosis directly affects treatment, as the strategies are completely different: while in IGM, steroids can be used to control inflammation, in tuberculosis, starting immunosuppressants without specific antibiotics is contraindicated. This case demonstrates that, without a clear diagnosis, physicians are limited to offering only surveillance, which may not be sufficient if there is an active, untreated infection. It is necessary to maintain a high level of clinical suspicion in patients with risk factors and to remember that not all painful breast lumps are cancer or common infections. It is also essential to promote further research to develop more sensitive and specific diagnostic tests for breast tuberculosis and to establish safe and effective management protocols, especially in vulnerable populations such as immunosuppressed patients.
An additional clinical challenge is the management of women who are actively breastfeeding, where prolonged corticosteroid regimens may raise concerns regarding neonatal exposure. This reinforces the importance of tailoring therapy to the patient's reproductive stage and of generating further evidence in this specific population. Only through rigorous study and clinical reflection can we develop diagnostic tools that not only improve treatment but also provide certainty to those caught between two probable diagnoses and no definitive answer. In cases like this, medicine becomes not only a science but a profound exercise in observation, patience, and compassion.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Idiopathic granulomatous mastitis as a benign condition mimicking inflammatory breast cancer: current status, knowledge gaps and rationale for the GRAMAREG Study (EUBREAST-15)Cancers (Basel) Krawczyk N Kühn T Ditsch N 16202410.3390/cancers 16193387 PMC 1147602939410007 · doi ↗ · pubmed ↗
- 2Granulomatous mastitis: etiology, imaging, pathology, treatment, and clinical findings Breast Cancer Res Treat Barreto DS Sedgwick EL Nagi CS Benveniste AP 52753417120182997162410.1007/s 10549-018-4870-3 · doi ↗ · pubmed ↗
- 3Granulomatous lobular mastitis co-existing with ductal carcinoma in situ: Report of three cases and review of the literature Ann Diagn Pathol Zhu J Miao X Li X Zhang Y Lou Y Chen H Liu X 1522416820243800801610.1016/j.anndiagpath.2023.152241 · doi ↗ · pubmed ↗
- 4Bilateral granulomatous mastitis with a different etiology Cancer Biomark Choi SH Jang KS Chung MS 3333381520152551901310.3233/CBM-140447 PMC 12964679 · doi ↗ · pubmed ↗
- 5Idiopathic granulomatous mastitis: manifestations at multimodality imaging and pitfalls Radiographics Pluguez-Turull CW Nanyes JE Quintero CJ Alizai H Mais DD Kist KA Dornbluth NC 3303563820182952881910.1148/rg.2018170095 · doi ↗ · pubmed ↗
- 6Red flags for the differential diagnosis of granulomatous mastitis: a case report J Med Case Rep Chalmers R Mc Clellan P Silva V Shutt N Restini C 2151420203316806910.1186/s 13256-020-02563-x PMC 7654600 · doi ↗ · pubmed ↗
- 7Idiopathic granulomatous mastitis: Etiology, clinical manifestation, diagnosis and treatment J Invest Surg Yin Y Liu X Meng Q Han X Zhang H Lv Y 7097203520223369156310.1080/08941939.2021.1894516 · doi ↗ · pubmed ↗
- 8Technical aspects: Coronary artery bypass grafting in a case of dextrocardia with situs inversus Cureus Ravikumar MS Palanisamy V Tamilselvan M Sangili S Sethuratnam R 013202110.7759/cureus.14932 PMC 818890534123630 · doi ↗ · pubmed ↗