Gut Microbiota-Directed Interventions in Type 2 Diabetes: A Systematic Review of Clinical Outcomes and Complication Risk
Mustafeez Ur Rehman, Hadia Saeed, Osman Omer, Shahbaz Tashfeen

TL;DR
This review explores how gut microbiota interventions may help manage type 2 diabetes by improving metabolism and reducing complications.
Contribution
The paper systematically reviews clinical outcomes of gut microbiota-directed therapies in type 2 diabetes.
Findings
Butyrate-producing bacteria and Akkermansia muciniphila are linked to improved insulin sensitivity and reduced inflammation.
Probiotics, prebiotics, and dietary changes show promise in glycemic control and cardiometabolic risk reduction.
Personalized approaches based on baseline microbiota may enhance therapeutic effectiveness.
Abstract
Type 2 diabetes mellitus is increasingly recognized as a disorder not only of glucose metabolism but also of gut microbial imbalance, with emerging evidence suggesting a bidirectional link between microbiome composition and metabolic dysfunction. Recent randomized controlled trials and dietary interventions highlight that specific microbial taxa, such as butyrate-producing bacteria and Akkermansia muciniphila, play crucial roles in regulating insulin sensitivity, lipid metabolism, and systemic inflammation. Modulation of the gut-metabolic axis through probiotics, prebiotics, dietary strategies, and pharmacological agents demonstrates promising effects on glycemic control, cardiometabolic risk reduction, and attenuation of diabetes-related complications, though results vary across populations and intervention types. The variability in outcomes underscores the importance of personalized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
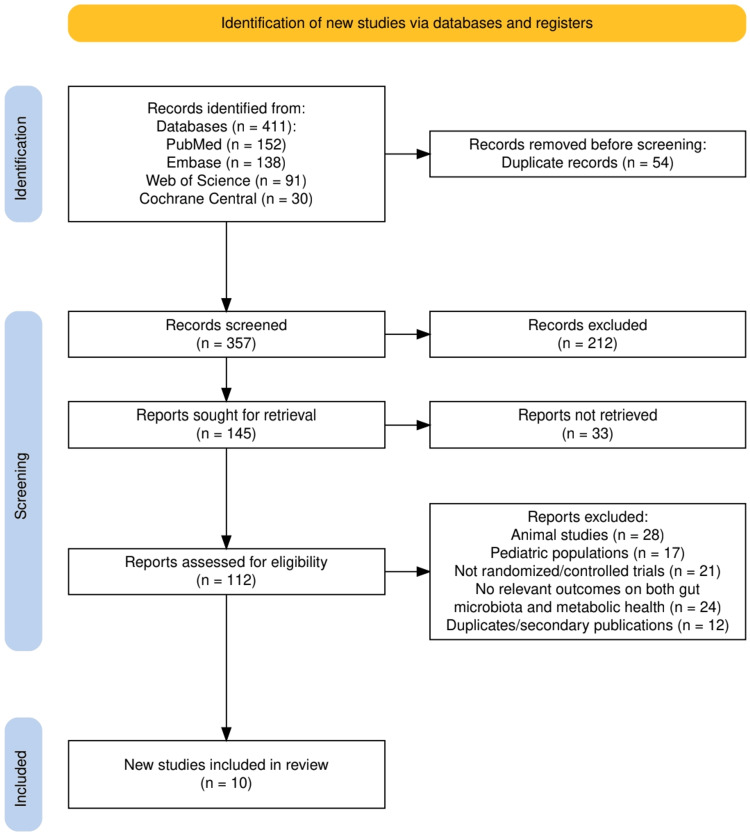 Figure 1
Figure 1| Authors (Year) | Study Design | Population (P) | Intervention (I) | Comparator (C) | Outcomes (O) | Key Findings |
| Depommier et al., 2019 [ | RCT (double-blind, placebo-controlled, pilot) | 40 overweight/obese insulin-resistant adults (32 completed) | Oral supplementation with live or pasteurized Akkermansia muciniphila for 3 months | Placebo | Primary: Safety, tolerability, metabolic parameters (insulin resistance, lipids, adiposity, BMI). Secondary: gut barrier function, gut microbiota composition | Pasteurized A. muciniphila improved insulin sensitivity (+28.6%), reduced insulinemia (-34%) and cholesterol (-8.7%); slight reduction in weight, fat mass, and hip circumference. Safe and well-tolerated. |
| Wang et al., 2022 [ | Multicenter, double-blind, placebo-controlled RCT | 365 patients with type 2 diabetes (PREMOTE study) | Combined berberine (BBR) + probiotics (Bifidobacterium breve) for 3 months | Placebo; BBR alone; Probiotic alone | Primary: Postprandial lipidemia (total cholesterol, LDLc). Secondary: gut microbiota composition, lipidomic metabolites, mechanistic gene expression | Combination (Prob+BBR) significantly reduced postprandial cholesterol and LDLc vs. control and single interventions; linked to increased B. breve activity and FFA metabolism; suggests synergistic hypolipidemic and microbiome-mediated effect. |
| Rein et al., 2022 [ | Randomized crossover pilot trial (with six-month extension) | 23 adults with newly diagnosed T2DM (mean age 53.5 ± 8.9 years, 48% male) | Personalized postprandial-targeting (PPT) diet using machine learning integrating microbiome & clinical features | Mediterranean-style diet (MED) | CGM-based glycemic measures, HbA1c, fasting glucose, triglycerides, gut microbiome shifts | PPT diet significantly lowered postprandial glucose response, mean glucose, and time >140 mg/dl vs. MED diet. Long-term PPT reduced HbA1c (−0.39%), fasting glucose (−16.4 mg/dl), triglycerides (−49 mg/dl), with 61% achieving diabetes remission. Clinical improvements linked to microbiome changes. |
| Deng et al., 2022 [ | Randomized, open-label, two-arm clinical trial (three months) | 76 treatment-naïve T2DM patients with cardiovascular risk factors (Empagliflozin n=40; Metformin n=36) | Empagliflozin 10 mg/day | Metformin 1700 mg/day | HbA1c, glucose metabolism, cardiovascular risk factors, gut microbiota (16S rRNA), plasma metabolites (LC-MS) | Both groups reduced HbA1c, but only empagliflozin improved cardiovascular risk factors. Empagliflozin reshaped gut microbiota (↑ Roseburia, Eubacterium, Faecalibacterium; ↓ Escherichia-Shigella, Bilophila, Hungatella) and altered plasma metabolites (↑ sphingomyelin; ↓ glycochenodeoxycholate, cis-aconitate, uric acid). Suggests cardiovascular benefit linked to microbiota/metabolite shifts. |
| Companys et al., 2022 [ | Randomized, double-blind, placebo-controlled parallel trial (12 weeks + acute 4h test) | 120 abdominally obese adults | 50 g/day enriched seafood sticks containing heat-inactivated B. animalis subsp. lactis CECT8145 (10¹⁰ CFU), 370 mg/day omega-3, and 1.7 g/day inulin | Placebo seafood sticks (50 g/day) | Insulin, HOMA-IR, pulse pressure (PP), postprandial triglycerides, gut microbiota composition | Significant ↓ insulin (-5.25 mg/dL) and HOMA-IR (-1.33). In women, ↓ PP (-4.69 mmHg). Acute study: lower rise in postprandial triglycerides vs placebo (+23.9 vs +49.0 mg/dL). Gut microbiota: ↓ Alistipes finegoldii and Ruminococcaceae linked to glycemic improvement; ↓ Prevotella 9-ASV0283 and Christensenellaceae linked to PP reduction. Suggests protection against T2DM and CVD risk. |
| Kallapura et al., 2024 [ | Prospective, open-label, randomized, controlled, proof-of-concept study (three months) | 30 participants with T2DM and hyperlipidemia (Test arm n=15; Control arm n=15) | Microbiome-based personalized nutrition guided by BugSpeaks® microbiota profiling (whole genome shotgun sequencing → tailored diet) | Standard diabetic nutritional guidance | HbA1c, BP, CRP, gut microbiota diversity and composition | Test arm: HbA1c ↓ from 8.3 → 6.67 (p<0.001); systolic BP ↓ 5% (subgroup with >130 mmHg: ↓ 14%); CRP ↓ 19.5%. Gut microbiota showed ↑ beneficial species (Phascolarctobacterium succinatutens, B. angulatum, L. brevis) and ↓ potentially harmful species (A. finegoldii, S. faecalis). Significant ↑ Shannon diversity (p<0.05). Overall: improved glycemia, BP, inflammation linked to microbiota modulation. |
| Feng et al., 2022 [ | Randomized, double-blinded, placebo-controlled clinical trial (four months) | 90 T2DM patients (intensive phase) → 55 continued in maintenance phase | White Common Bean Extract (WCBE, 1.5 g before meals, α-amylase inhibitor) + normal carbohydrate intake | Placebo (1.5 g maltodextrin) | HbA1c, diabetic neuropathy (TCSS), sural sensory nerve conduction velocity, gut microbiota composition | WCBE group: HbA1c ↓ by 0.72% (p<0.05); fewer cases of diabetic peripheral neuropathy; sural SNCV improved (vs. decline in placebo). Gut microbiota: ↑ Bifidobacterium, Faecalibacterium, Anaerostipes; ↓ Weissella, Klebsiella, Cronobacter, Enterobacteriaceae. SCFA-producers enrichment linked to benefits. Overall: WCBE improved glycemic control and attenuated diabetic complications via microbiota modulation. |
| Haro et al., 2016 [ | Randomized, open-label, controlled dietary intervention (one year) | 20 obese men (from the CORDIOPREV study, with coronary heart disease) | Mediterranean diet (35% fat, 22% MUFA) | Low-fat, high-complex carbohydrate (LFHCC) diet (28% fat, 12% MUFA) | Gut microbiota composition, fecal and plasma metabolome, insulin sensitivity markers | LFHCC diet: ↑ Prevotella, ↓ Roseburia. Mediterranean diet: ↓ Prevotella, ↑ Roseburia & Oscillospira. Both diets: ↑ beneficial species (Parabacteroides distasonis with Med; Faecalibacterium prausnitzii with LFHCC). Microbiota shifts correlated with metabolomic changes (amino acids, peptides, sphingolipids). Overall, both diets improved gut microbial balance linked to improved insulin sensitivity and protection against T2DM development. |
| Balfegó et al., 2016 [ | Pilot randomized controlled trial (six months) | 35 drug-naïve patients with type 2 diabetes | Standard T2DM diet + 100 g sardines, 5 days/week | Standard T2DM diet (control) | Glycemic control (HbA1c, glucose, insulin, HOMA-IR), adiponectin, inflammatory markers, erythrocyte membrane fatty acid composition, gut microbiota composition | Both groups ↓ fasting insulin and HOMA-IR (improved insulin sensitivity). Only sardine group ↑ adiponectin (+40.7%, P = 0.04) and omega-3 index (+2.6% vs +0.6% in CG, P = 0.001). Gut microbiota: both ↓ Firmicutes, ↑ E. coli; sardine group specifically ↓ Firmicutes/Bacteroidetes ratio and ↑ Bacteroides-Prevotella. No significant differences in HbA1c between groups. Suggests cardiometabolic benefit more than glycemic benefit. |
| Eriksen et al., 2020 [ | Randomized crossover trial (eight weeks) | 40 men with a metabolic syndrome risk profile | Whole-grain rye diet ± lignan (secoisolariciresinol diglucoside, 280 mg at weeks 4–8) | Whole-grain wheat diet | Glucose tolerance (OGTT), cardiometabolic outcomes (lipids, BP), microbiota composition, enterolignans | WG rye (± lignan) did not improve glucose tolerance vs. wheat. After 4 weeks, rye ↓ total cholesterol (−0.06 mmol/L) and LDL-C (−0.09 mmol/L, P < 0.05), but effect not sustained at 8 weeks. WG rye ↑ Bifidobacterium (FC = 2.58, P < 0.001) and ↓ Clostridium genus (FC = 0.54, P = 0.02). Response to the WG diet differed by baseline microbiota enterotype. |
| Authors (Year) | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall Risk of Bias |
| Depommier et al., 2019 [ | Low (randomization, blinding clear) | Low (double-blind, placebo) | Low (32/40 completed) | Low (objective metabolic outcomes) | Low | Low |
| Wang et al., 2022 [ | Low (multicenter RCT, good concealment) | Low (double-blind, placebo-controlled) | Low (large n, minimal attrition reported) | Low (biochemical measures) | Some concerns (complex outcome reporting, many secondary endpoints) | Some concerns |
| Rein et al., 2022 [ | Low (randomized crossover, well described) | Some concerns (short duration crossover may have carryover effect) | Low (high completion rate) | Low (CGM and HbA1c are reliable) | Low | Some concerns |
| Deng et al., 2022 [ | Some concerns (open-label → performance bias risk) | High (not blinded, behavior may differ by treatment group) | Low (minimal attrition reported) | Low (objective lab outcomes) | Low | Some concerns |
| Companys et al., 2022 [ | Low (double-blind RCT) | Low (good control/placebo) | Low (n=120, balanced arms) | Low (standard metabolic markers) | Low | Low |
| Kallapura et al., 2024 [ | Some concerns (open-label design) | High (no blinding → intervention adherence bias) | Low (30/30 analyzed) | Low (HbA1c, BP, CRP are objective) | Some concerns (pilot “proof of concept” study → selective reporting possible) | Some concerns |
| Feng et al., 2022 [ | Low (double-blind, placebo-controlled) | Low | Low (reasonable follow-up, maintenance phase) | Low (objective endpoints, neuropathy scoring validated) | Low | Low |
| Haro et al., 2016 [ | Low (randomized, clear dietary allocation) | Some concerns (open-label diet trial, adherence self-reported) | Low | Low (microbiota + metabolome objectively measured) | Some concerns (dietary adherence reporting selective) | Some concerns |
| Balfegó et al., 2016 [ | Low (randomized, dietary trial) | Some concerns (open-label nutrition trial, adherence issues) | Low (35/35 analyzed) | Low | Some concerns (pilot, small sample) | Some concerns |
| Eriksen et al., 2020 [ | Low (crossover RCT, good design) | Some concerns (possible carryover effects) | Low | Low | Low | Some concerns |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiet and metabolism studies · Gut microbiota and health · Obesity and Health Practices
Introduction and background
Type 2 diabetes mellitus (T2DM) is one of the most prevalent metabolic disorders worldwide, accounting for more than 90% of diabetes cases. Its hallmark features include chronic hyperglycemia, insulin resistance, and progressive β-cell dysfunction, which together increase the risk of long-term complications such as cardiovascular disease, nephropathy, neuropathy, and retinopathy [1,2]. Despite advances in pharmacotherapy and lifestyle interventions, the global burden of T2DM continues to rise, underscoring the need to explore novel determinants of disease development and progression [3].
In recent years, the gut microbiome has emerged as a key player in metabolic health. The human intestinal microbiota functions as a metabolic “organ,” influencing host physiology through nutrient absorption, immune modulation, bile acid metabolism, and production of bioactive metabolites such as short-chain fatty acids (SCFAs), trimethylamine-N-oxide (TMAO), and succinate [4,5]. Alterations in microbiome composition and diversity, collectively termed dysbiosis, have been consistently associated with obesity, insulin resistance, and T2DM. Dysbiosis may exacerbate systemic inflammation, impair insulin signaling, and contribute to the development of both microvascular and macrovascular complications [6].
Multiple interventional studies have begun to evaluate whether targeted modulation of the gut microbiome, through dietary interventions, probiotics, prebiotics, synbiotics, fecal microbiota transplantation (FMT), and antidiabetic pharmacotherapies, can improve insulin sensitivity and reduce cardiometabolic risk [7]. For example, supplementation with Akkermansia muciniphila, use of specific probiotics, and diets enriched in fiber or omega-3 fatty acids have demonstrated beneficial effects on glucose metabolism and inflammatory pathways. Similarly, widely used antidiabetic agents such as metformin and SGLT2 inhibitors appear to exert part of their therapeutic effects through microbiome-mediated mechanisms.
The objective of this systematic review is to synthesize and critically evaluate clinical evidence on gut microbiota-directed interventions in adults with type 2 diabetes, with a dual focus on glycemic outcomes and diabetes-related complications. Unlike previous reviews that examined isolated probiotic or dietary effects, this study integrates findings across diverse interventional strategies, including dietary, pharmacological, and personalized nutrition approaches, to provide a comprehensive overview of how modulation of the gut-metabolic axis influences both metabolic control and complication risk. By highlighting mechanistic insights and identifying evidence gaps, this review aims to clarify the clinical potential and limitations of microbiome-targeted therapies in the context of precision diabetes management [8].
Review
Materials and methods
Study Design and Protocol Registration
This study was conducted as a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [9]. The review protocol was designed a priori to ensure methodological transparency and consistency. The primary objective was to evaluate the role of gut microbiome composition in insulin resistance and the development of complications in type 2 diabetes mellitus (T2DM). The review incorporated randomized controlled trials (RCTs), pilot studies, and dietary intervention trials that directly assessed the impact of microbiota-targeted therapies, dietary modulation, or pharmacological interventions on metabolic outcomes.
Eligibility Criteria (PICO Framework)
The inclusion criteria were defined using the PICO framework [10]. The Population (P) included adult individuals with type 2 diabetes, obesity, metabolic syndrome, or insulin resistance. The Interventions (I) considered were microbiome-directed therapies, including probiotics, prebiotics, synbiotics, dietary modifications, microbiota-targeted personalized nutrition, or pharmacological interventions with a demonstrated effect on the gut microbiome. The Comparators (C) comprised placebo, standard care, conventional dietary regimens, or alternative interventions not targeting the gut microbiome. The Outcomes (O) of interest included glycemic parameters (glycated hemoglobin A1c (HbA1c), fasting glucose, postprandial glucose, insulin sensitivity indices), cardiometabolic markers (lipid profile, blood pressure, inflammatory markers), diabetes-related complications (neuropathy, vasculopathy), and gut microbiota composition or diversity. Only randomized controlled trials or controlled dietary interventions published in peer-reviewed journals were eligible. Studies involving pediatric populations, animal models, or those without primary outcomes related to both gut microbiota and metabolic health were excluded.
Information Sources and Search Strategy
A comprehensive literature search was conducted across PubMed, Embase, Web of Science, and Cochrane Central Register of Controlled Trials from inception until September 2024. Search terms were developed in consultation with controlled vocabulary (MeSH) and keywords, combining terms such as “type 2 diabetes,” “insulin resistance,” “gut microbiota,” “microbiome,” “complications,” “diet,” “probiotics,” “prebiotics,” and “cardiometabolic risk.” Boolean operators and truncation were applied to maximize retrieval. The reference lists of relevant reviews and included studies were also screened to capture additional eligible trials. Only studies published in English were considered.
Study Selection and Data Extraction
Titles and abstracts retrieved from the initial search were independently screened by two reviewers for eligibility. Full-text assessment was performed for all potentially relevant studies. Discrepancies were resolved through discussion or by a third reviewer when necessary. Data were systematically extracted into a predesigned form, capturing study characteristics (author, year, country, design, sample size), participant demographics, details of intervention and comparator arms, duration of follow-up, and primary and secondary outcomes. Key findings were summarized for narrative synthesis.
Risk of Bias Assessment
The quality and risk of bias of included RCTs were assessed using the Cochrane Risk of Bias 2.0 tool (RoB 2) [11]. The tool evaluates five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was judged as low risk, some concerns, or high risk, with an overall risk of bias rating for each study. This assessment was conducted independently by two reviewers, with disagreements resolved by consensus.
Data Synthesis and Analysis
Given the heterogeneity in interventions and outcomes across studies, a meta-analysis was not performed, and results were synthesized narratively. A structured summary of study designs, populations, interventions, comparators, outcomes, and key findings was compiled in tabular form. Particular emphasis was placed on linking microbiota composition and functional shifts with metabolic outcomes, including glycemic control, insulin resistance, lipid regulation, and diabetes-related complications. Where applicable, trends and mechanistic insights into microbiome-host interactions were highlighted to provide context for clinical implications and future research directions.
Results
Study Selection Process
A total of 411 records were identified through database searches, including PubMed (n = 152), Embase (n = 138), Web of Science (n = 91), and Cochrane Central (n = 30). After removal of 54 duplicates, 357 records were screened by title and abstract, of which 212 were excluded for irrelevance. Of the remaining 145 reports sought for retrieval, 33 could not be accessed, leaving 112 full-text articles assessed for eligibility. Following detailed evaluation, 28 animal studies, 17 involving pediatric populations, 21 without randomized or controlled trial design, 24 lacking outcomes related to both gut microbiota and metabolic health, and 12 duplicate or secondary publications were excluded. Ultimately, 10 studies met the inclusion criteria and were synthesized for this systematic review. The whole screening process is illustrated in Figure 1.
The PRISMA flowchart represents the study selection processPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of the Selected Studies
The 10 randomized controlled and controlled dietary intervention trials included in this review demonstrated a diverse range of microbiome-targeted approaches in type 2 diabetes and metabolic syndrome. As summarized in Table 1, interventions ranged from probiotic and synbiotic supplementation (e.g., Akkermansia muciniphila, Bifidobacterium breve with berberine) to pharmacological agents (empagliflozin), functional foods (white bean extract, enriched seafood sticks, whole-grain rye), and personalized nutrition guided by microbiome profiling. Across studies, improvements were consistently observed in glycemic parameters, insulin sensitivity, lipid metabolism, and cardiometabolic risk markers, with several trials also linking these outcomes to shifts in gut microbial diversity and composition. Collectively, these findings highlight both the therapeutic potential and heterogeneity of microbiome-based strategies in modulating insulin resistance and complication risk in type 2 diabetes.
Risk of Bias Assessment
The risk of bias assessment summarized in Table 2 indicates that most included studies demonstrated low risk across key domains such as randomization, outcome measurement, and completeness of follow-up, particularly in double-blind, placebo-controlled trials. However, open-label designs and short-duration crossover interventions introduced potential performance and carryover biases in some cases, while pilot or proof-of-concept studies raised concerns regarding selective reporting due to limited scope and complex outcome endpoints. Overall, although the evidence base is generally robust and methodologically sound, the identified concerns highlight the importance of cautious interpretation and emphasize the need for larger, well-blinded, multicenter studies to strengthen confidence in the observed associations.
Discussion
Summary of Main Findings
This systematic review demonstrates that modulation of the gut microbiota through dietary, probiotic, pharmacological, and personalized nutrition strategies consistently yields favorable effects on glycemic control, insulin sensitivity, and cardiometabolic outcomes in patients with type 2 diabetes mellitus (T2DM) or at high metabolic risk. Pasteurized Akkermansia muciniphila improved insulin sensitivity by 28.6% and reduced insulinemia by 34% [12], while combined berberine and Bifidobacterium breve supplementation reduced postprandial LDL cholesterol more effectively than either agent alone [13]. Personalized machine learning-guided diets integrating microbiome profiles achieved diabetes remission in 61% of newly diagnosed patients and significantly reduced triglycerides by 49 mg/dL [14]. Pharmacological intervention with empagliflozin reshaped the microbiome-enriching butyrate-producing species such as Roseburia and Faecalibacterium, and uniquely improved cardiovascular markers beyond glycemic control [15]. Diet-based strategies, including seafood sticks enriched with heat-inactivated Bifidobacterium animalis and omega-3 [16], Mediterranean versus low-fat diets [19], and sardine-enriched diets [20], consistently linked microbial enrichment to improved insulin sensitivity and lipid metabolism. Collectively, these trials highlight the gut-metabolic axis as a therapeutic target, with interventions enhancing short-chain fatty acid producers such as Faecalibacterium prausnitzii and Bifidobacterium emerging as particularly beneficial.
Critical Comparison and Contrast
A critical evaluation of the included studies reveals heterogeneity in efficacy that appears to be driven by the nature of intervention, baseline disease stage, and host-microbiome interactions. For example, live versus pasteurized Akkermansia muciniphila produced divergent outcomes, with the pasteurized form demonstrating superior metabolic improvements, likely due to preserved membrane proteins stimulating host pathways [12]. In contrast, pharmacological modulation with empagliflozin induced rapid and broad microbial shifts toward butyrate-producing taxa, an effect not mirrored by metformin, underscoring drug-specific microbiome crosstalk [15]. Dietary interventions generally produced gradual but sustained microbial changes, such as the rise in Roseburia with the Mediterranean diet [19], while machine learning-based personalized diets achieved stronger glycemic responses than standardized Mediterranean diets, highlighting the role of individualized microbiome-host integration [14]. Notably, sex-specific effects emerged in [16], where women experienced a greater reduction in pulse pressure, suggesting hormonal or microbial compositional differences in responsiveness. Furthermore, heterogeneity in outcomes across whole-grain interventions indicated that baseline enterotype predicted cholesterol reduction [21], a finding that reinforces the emerging paradigm of precision nutrition. These contrasts emphasize that while microbiome modulation consistently benefits metabolic outcomes, the magnitude and nature of benefit depend on the form of intervention, host phenotype, and baseline microbial ecology.
Mechanistic Insights: Linking Microbiome Shifts to Clinical Benefit
The included RCTs collectively highlight how microbiome modulation mediates clinical improvements in T2DM through distinct biological pathways. Supplementation with pasteurized *Akkermansia muciniphila *[12] enhanced gut barrier integrity and reduced endotoxemia, directly improving insulin sensitivity by 28.6%. Pharmacological modulation with empagliflozin [15] enriched butyrate-producing taxa (Roseburia, Faecalibacterium, Eubacterium) while reducing harmful species such as Escherichia-Shigella, leading to improved cardiovascular markers beyond glycemic control. Personalized nutrition guided by machine learning algorithms [14,17] demonstrated that therapeutic responses are contingent on baseline microbial signatures, with precision diets tailored to microbiome composition driving sustained HbA1c reductions and diabetes remission in subsets of patients. Dietary strategies such as sardine-enriched or Mediterranean diets improved omega-3 indices, enriched anti-inflammatory taxa, and reduced pro-atherogenic microbial pathways, suggesting a dual role in both metabolic and cardiovascular protection [19,20]. These mechanistic links underscore that the gut-metabolic axis acts as a mediator rather than a passive bystander in T2DM, supporting the rationale for microbiome-targeted therapies.
Gaps and Limitations in the Literature
Despite promising findings, several limitations constrain translation into clinical practice. Many RCTs were short-term, typically lasting three to six months, leaving the sustainability of microbiome-induced benefits over years largely untested. Sample sizes were modest-often fewer than 120 participants-with some pilot trials including as few as 20 patients, limiting statistical power and external validity. Methodological inconsistencies, such as reliance on 16S rRNA sequencing in some studies versus whole-genome shotgun sequencing in others, hinder comparability across interventions. Outcomes were primarily surrogate endpoints, HbA1c, HOMA-IR, or lipid changes, whereas hard endpoints such as cardiovascular events, hospitalization, or diabetic complications were rarely examined, with the exception of neuropathy outcomes in the WCBE trial [18]. Moreover, most cohorts were ethnically homogeneous and geographically narrow, restricting insights into population-level variability in microbiome response. Finally, sex-specific differences were reported only incidentally, as in Companys et al., suggesting that stratified analyses by sex, age, and ethnicity remain underexplored [16]. Together, these gaps highlight the urgent need for larger, longer-duration, and methodologically harmonized trials that incorporate clinically meaningful endpoints and diverse populations.
Novel and Useful Insights
An important emerging insight from this synthesis is that microbiome profiling should be considered for integration into diabetes management algorithms, allowing clinicians to stratify patients into likely responders to diet-based versus pharmacological therapies. Evidence from Rein et al. [14] and Kallapura et al. [17] indicates that baseline microbial composition can predict therapeutic response, suggesting that a "precision nutrition" model could optimize outcomes and reduce trial-and-error in T2DM management. Furthermore, combination strategies appear more effective than monotherapies, as seen in Wang et al. [13], where berberine plus probiotics produced synergistic lipid-lowering and microbiome-mediated effects beyond either intervention alone. The role of microbiome-targeted therapies in mitigating complications is also noteworthy. Feng et al. [18] demonstrated improvement in diabetic neuropathy, while Deng et al. [15] linked microbial shifts to cardiovascular benefit, expanding the scope of microbiome modulation beyond glycemic control alone. Finally, artificial intelligence and machine learning models, exemplified by the personalized postprandial-targeting diet, show scalability for global application in diabetes care [14]. Yet, the stability of induced microbial shifts after stopping interventions-microbiota resilience-remains a largely unstudied dimension, representing a key knowledge gap with direct implications for long-term disease management.
Clinical Implications
The findings of this review suggest that microbiome-based interventions could represent a cost-effective and scalable adjunct to traditional T2DM therapies, particularly in resource-limited settings where access to novel agents such as SGLT2 inhibitors or GLP-1 receptor agonists is restricted [22]. Dietary strategies, such as whole grains, Mediterranean diets, or functional foods enriched with probiotics, are inexpensive, culturally adaptable, and could be incorporated into routine dietary counseling for diabetes patients. Moreover, gut microbial signatures-if validated-hold promise as predictive biomarkers for therapeutic success, guiding the choice of whether a patient is more likely to benefit from dietary modification, pharmacotherapy, or combined approaches [23]. By targeting the gut-metabolic axis, clinicians may not only improve glycemic control but also reduce the risk of microvascular and macrovascular complications, thereby reshaping the paradigm of holistic diabetes management.
Future Directions
To translate these promising results into practice, future research should prioritize large-scale, multicenter RCTs with long-term follow-up (>12 months) to assess the sustainability of microbiome-induced benefits and their impact on hard outcomes such as cardiovascular events, renal decline, or neuropathy progression. Integration of multi-omics platforms, including metabolomics, proteomics, and transcriptomics, will be essential to unravel causal pathways linking microbial changes with host metabolic physiology. Trials directly comparing personalized versus standardized microbiome-directed interventions are also warranted to determine the added value of precision strategies in real-world populations. Importantly, stratified analyses addressing sex-specific and age-specific responses to microbiome modulation must be incorporated, given signals of differential efficacy observed in some trials (e.g., blood pressure effects in women [16]). Finally, understanding the resilience of microbiota changes-whether interventions induce permanent or transient shifts-will be critical for designing long-term therapeutic protocols.
Conclusions
This systematic review highlights the pivotal role of gut microbiota modulation in improving insulin resistance and mitigating complications in type 2 diabetes. The evidence from randomized controlled trials demonstrates that both nutritional and pharmacological strategies, ranging from supplementation with specific microbes and bioactive compounds to microbiome-informed personalized diets, can induce favorable shifts in microbial composition, increase short-chain fatty acid-producing taxa, and translate these changes into measurable metabolic benefits. While most studies were limited by short duration and modest sample sizes, the consistency of findings across diverse interventions underscores the potential of microbiome-targeted therapies as an adjunct to standard diabetes care. The significance of this review lies in its synthesis of clinical and mechanistic insights, providing a framework for integrating microbiome profiling into diabetes management and informing future large-scale, long-term trials. Ultimately, the gut-metabolic axis may represent a cornerstone in the move toward precision medicine in type 2 diabetes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Type 2 diabetes mellitus: new pathogenetic mechanisms, treatment and the most important complications Int J Mol Sci Młynarska E Czarnik W Dzieża N 26202510.3390/ijms 26031094 PMC 1181770739940862 · doi ↗ · pubmed ↗
- 2Deciphering the complex interplay of risk factors in type 2 diabetes mellitus: a comprehensive review Metabol Open Singh S Kriti M K SA 1002872220243881822710.1016/j.metop.2024.100287 PMC 11137529 · doi ↗ · pubmed ↗
- 3Current advances in the management of diabetes mellitus Biomedicines Aloke C Egwu CO Aja PM 10202210.3390/biomedicines 10102436 PMC 959936136289697 · doi ↗ · pubmed ↗
- 4Human gut microbiome: a connecting organ between nutrition, metabolism, and health Int J Mol Sci Valencia S Zuluaga M Florian Pérez MC Montoya-Quintero KF Candamil-Cortés MS Robledo S 26202510.3390/ijms 26094112 PMC 1207189740362352 · doi ↗ · pubmed ↗
- 5Functions of gut microbiota metabolites, current status and future perspectives Aging Dis Liu J Tan Y Cheng H Zhang D Feng W Peng C 110611261320223585534710.14336/AD.2022.0104 PMC 9286904 · doi ↗ · pubmed ↗
- 6Gut microbiota dysbiosis and its impact on type 2 diabetes: from pathogenesis to therapeutic strategies Metabolites Yu Y Ding Y Wang S Jiang L 15202510.3390/metabo 15060397 PMC 1219500740559421 · doi ↗ · pubmed ↗
- 7Gut microbiota-targeted therapeutics for metabolic disorders: mechanistic insights into the synergy of probiotic-fermented herbal bioactives Int J Mol Sci Fan Y Liu Y Shao C Jiang C Wu L Xiao J Tang L 26202510.3390/ijms 26125486 PMC 1219347240564947 · doi ↗ · pubmed ↗
- 8A critical perspective on the supplementation of Akkermansia muciniphila: benefits and harms Life (Basel) Chiantera V LaganàAS Basciani S Nordio M Bizzarri M 13202310.3390/life 13061247 PMC 1030119137374030 · doi ↗ · pubmed ↗