Salvage Reconstruction With Recycled Flap Pedicles in Head‐and‐Neck Surgery: A Report of Two Cases
Akatsuki Kondo, Hiroki Umezawa, Marie Taga, Rei Ogawa

TL;DR
This paper describes a surgical technique where previously used blood vessels are reused to reconstruct head and neck defects when traditional options are not available.
Contribution
The novelty lies in reusing the vascular pedicle of a prior free flap for salvage reconstruction in vessel-depleted necks.
Findings
Reusing the ALT flap pedicle successfully provided blood supply for new flaps in two patients.
Both salvage surgeries resulted in flap survival with no major complications.
The approach may simplify complex reconstructions when conventional vessels are unavailable.
Abstract
Free‐flap reconstruction of head‐and‐neck defects is often complicated by a vessel‐depleted neck after prior surgery or radiotherapy. Conventional alternatives—such as using contralateral vessels, distant recipient vessels, or interpositional vein grafts—are technically demanding and associated with additional risks. We present two salvage reconstructions in which the vascular pedicle of a previously transferred free flap was reused as recipient vessels when standard options were unavailable. A 79‐year‐old man developed exposure of a titanium mandibular plate 6 years after mandibular resection reconstructed with a free anterolateral thigh (ALT) flap. Preoperative ultrasonography and contrast‐enhanced computed tomography confirmed patency of the ALT flap pedicle despite dense fibrosis. After removal of the exposed plate, the pedicle was carefully dissected, and a scapular osteocutaneous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
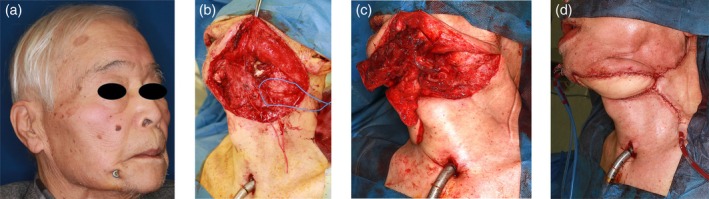 FIGURE 1
FIGURE 1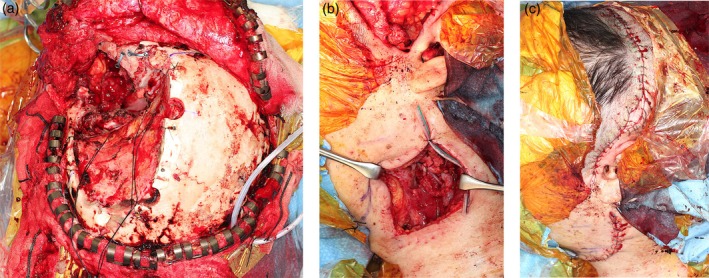 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Head and Neck Cancer Studies · Reconstructive Facial Surgery Techniques
Introduction
1
Free flap reconstruction in the head and neck critically depends on the availability of suitable recipient vessels. However, prior surgery and radiotherapy can cause vessel depletion due to fibrosis, vessel obliteration, or radiation‐induced vessel wall changes, resulting in a “vessel‐depleted neck.” Common synonyms include “hostile neck” and “frozen neck” (Ad‐El and Sichel 2004; Mulholland et al. 1993; Tan et al. 2014; Abouyared et al. 2019; Kushida‐Contreras et al. 2021).
When recipient vessels are limited, traditional strategies include using contralateral neck vessels, thoracoacromial or internal mammary vessels, or creating arteriovenous loops or vein grafts (Sakurai et al. 2016; Sadove and Kanter 1993; Ribuffo et al. 2004; Xiao et al. 2022).
While these options can be effective, they often require extensive dissection or additional anastomoses, potentially increasing operative time and complications. An alternative strategy is to reuse the vascular pedicle from a previously transferred free flap (Oswald et al. 1988; Pafitanis et al. 2020), though reports of this approach—particularly in head‐and‐neck salvage reconstruction—are rare. We describe two cases where pedicle reuse provided a safe and effective solution when no conventional recipient vessels were available.
Case Reports
2
Case 1
2.1
A 79‐year‐old man had previously undergone segmental mandibular resection and reconstruction for gingival squamous cell carcinoma using a titanium reconstruction plate and a free anterolateral thigh (ALT) flap, anastomosed to the facial artery and vein. Six years later, the plate became exposed (Figure 1a).
Intraoperative images of Case 1. (a) Preoperative view showing exposure of the mandibular plate on the right side. (b) Dissection of recipient vessels from the previous anterolateral thigh (ALT) flap pedicle following removal of the exposed titanium plate. (c) Microvascular anastomosis of the scapular osteocutaneous flap pedicle to the recipient vessels of the previous ALT flap. (d) Intraoperative view at wound closure.
Preoperative color Doppler ultrasonography and contrast‐enhanced computed tomography confirmed the patency of the pedicle vessels of the ALT flap, despite extensive fibrosis in the operative field. During salvage surgery, the exposed plate was removed. The pedicle of the ALT flap was carefully dissected through fibrotic tissue to expose the lateral circumflex femoral artery and vein (Figure 1b). To assess the viability of the existing flap, indocyanine green fluorescence angiography was performed after temporary clamping of the pedicle, confirming adequate perfusion of the ALT flap. A scapular osteocutaneous flap with a skin paddle measuring 9 × 12 cm and a bony segment measuring 2.5 × 11 cm was harvested. The flap was inset into the mandibular defect, and microvascular anastomosis was then performed between the scapular flap pedicle and the lateral circumflex femoral artery and vein of the previous ALT pedicle (Figure 1c). Bone fixation was achieved via miniplate fixation and then the wound was closed (Figure 1d). Postoperatively, the patient developed cholecystitis, which was managed with gallbladder drainage and antibiotics. The surgical wounds healed primarily, with no infection or necrosis of either flap. The patient was discharged on postoperative day 34, with restored mandibular contour and oral function.
Case 2
2.2
A 63‐year‐old man with recurrent meningioma of the left middle cranial fossa underwent tumor resection and reconstruction with a free ALT flap anastomosed to the superior thyroid artery and internal jugular vein. Two years later, the tumor recurred. Preoperative imaging confirmed patency of the previous ALT flap pedicle, while other ipsilateral vessels appeared compromised due to fibrosis. During salvage surgery, the recurrent tumor was removed and the pedicle of the previous ALT flap was carefully dissected (Figure 2a). A 9 × 20 cm free rectus‐abdominis flap was harvested from the left abdomen. The arterial supply of the rectus‐abdominis flap was anastomosed end‐to‐end to the artery of the previous ALT pedicle. As the venous caliber of the pedicle flap was insufficient, venous drainage was established by an end‐to‐side anastomosis to the internal jugular vein (Figure 2b). Flap perfusion was confirmed intraoperatively using indocyanine green fluorescence angiography. Part of the skin flap was externalized, and the wound was closed (Figure 2c). Both flaps survived without congestion or necrosis. The patient was discharged on postoperative day 39 with satisfactory functional and cosmetic outcomes.
Intraoperative images of Case 2. (a) Defect following tumor resection, with preservation of the previous anterolateral thigh (ALT) flap pedicle. (b) Microvascular anastomosis of the rectus abdominis flap artery to the arterial pedicle of the previous ALT flap. Venous anastomosis was performed to the internal jugular vein. (c) Intraoperative view at wound closure.
Discussion
3
These cases show that reusing the pedicle from a previously transferred free flap may be a viable salvage strategy when conventional recipient vessels are unavailable. In vessel‐depleted necks, conventional alternatives can be technically challenging—contralateral neck vessels may be difficult to access, and harvesting distant recipient vessels or creating arteriovenous loops can increase operative time and the risk of thrombosis (Millard 1969; Manrique et al. 2017).
In contrast, pedicle reuse harnesses an already accessible vascular conduit that has proven to be durable. Successful implementation of this approach depends on several considerations. First, preoperative imaging—such as Doppler ultrasonography and contrast‐enhanced computed tomography—should confirm patency of the previous pedicle. Second, intraoperative assessment using indocyanine green fluorescence angiography can verify whether the original flap has developed sufficient neovascularization to survive pedicle ligation. Third, meticulous dissection of fibrotic tissue and precise microsurgical technique are essential to avoid intimal injury; anastomotic sites should be chosen adjacent to, but not directly over, prior anastomoses. Finally, if the venous component of the pedicle is inadequate, an additional venous anastomosis to a nearby recipient vein, such as the internal jugular vein, may be necessary.
Some limitations should be acknowledged. The optimal interval between the initial flap transfer and pedicle reuse remains undefined. In our patients, pedicle reuse was undertaken after 6 years and 2 years, respectively; previous reports suggest neovascularization may develop within weeks, but consistent flap survival is not guaranteed (Fisher and Wood 1984). Moreover, radiation‐induced vessel fragility, dense fibrosis, and patient comorbidities can compromise outcomes (Yoon and Jones 2016; Herle et al. 2015).
Therefore, pedicle reuse may not be applicable in all cases, and careful patient selection is essential. Our experience with two patients suggests that pedicle reuse can reduce operative complexity and preserve the integrity of prior reconstructions, but larger studies are needed to further define its indications and long‐term outcomes.
Author Contributions
Akatsuki Kondo: conceptualization, study design, data collection, surgical procedures, and manuscript drafting. Hiroki Umezawa: manuscript review, surgical advice, and critical comments. Marie Taga: literature review and minor manuscript editing. Rei Ogawa: manuscript review, supervision, and final approval.
Consent
The patient consented to publishing their case details and photographs with eye masking.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abouyared, M. , A. P. Katz , L. Ein , et al. 2019. “Controversies in Free Tissue Transfer for Head and Neck Cancer: A Review of the Literature.” Head & Neck 41: 3457–3463.31286627 10.1002/hed.25853 · doi ↗ · pubmed ↗
- 2Ad‐El, D. D. , and J. E. Sichel . 2004. “Reversed‐Flow External Jugular Vein: An Optional Recipient Vessel in Microsurgical Head and Neck Reconstruction.” Plastic and Reconstructive Surgery 113: 1873–1875.15114172 10.1097/01.prs.0000119872.60605.90 · doi ↗ · pubmed ↗
- 3Fisher, J. , and M. B. Wood . 1984. “Late Necrosis of a Latissimus Dorsi Free Flap.” Plastic and Reconstructive Surgery 74: 274–281.6463151 10.1097/00006534-198408000-00018 · doi ↗ · pubmed ↗
- 4Herle, P. , L. Shukla , W. A. Morrison , and R. Shayan . 2015. “Preoperative Radiation and Free Flap Outcomes for Head and Neck Reconstruction: A Systematic Review and Meta‐Analysis.” ANZ Journal of Surgery 85: 121–127.25345755 10.1111/ans.12888 · doi ↗ · pubmed ↗
- 5Kushida‐Contreras, B. H. , O. J. Manrique , and M. A. Gaxiola‐García . 2021. “Head and Neck Reconstruction of the Vessel‐Depleted Neck: A Systematic Review of the Literature.” Annals of Surgical Oncology 28: 2882–2895.33550502 10.1245/s 10434-021-09590-y · doi ↗ · pubmed ↗
- 6Manrique, O. J. , S. H. Chen , P. Ciudad , and H. C. Chen . 2017. “Neovascularization Failure of an Interposed Free Intestinal Colon Flap 10 Years After Esophageal Reconstruction.” Journal of Reconstructive Microsurgery Open 2: e 35‐e 36.
- 7Millard, D. R. 1969. “The Crane Principle for the Transport of Subcutaneous Tissue.” Plastic and Reconstructive Surgery 43: 451–462.4889409 10.1097/00006534-196905000-00001 · doi ↗ · pubmed ↗
- 8Mulholland, S. , J. B. Boyd , S. Mc Cabe , et al. 1993. “Recipient Vessels in Head and Neck Microsurgery: Radiation Effect and Vessel Access.” Plastic and Reconstructive Surgery 92: 628–632.8356125 10.1097/00006534-199309001-00011 · doi ↗ · pubmed ↗