Differential Diagnosis in Patients Presenting With Peripheral Lymphadenopathy: Tuberculosis, Sarcoidosis, or Malignancy
Esma Tuğba Canlı, Merve Erçelik, Önder Öztürk, Hasan Yasan, İbrahim Metin Çiriş

TL;DR
This paper discusses the challenges in diagnosing two patients with neck swelling, highlighting the difficulty in distinguishing between tuberculosis, sarcoidosis, and cancer.
Contribution
The paper emphasizes the importance of microbiological evaluation in accurately diagnosing lymphadenopathy cases.
Findings
The female patient was diagnosed with tuberculous lymphadenitis despite initial suspicion of malignancy.
The male patient was diagnosed with sarcoidosis despite initial suspicion of tuberculosis reactivation.
Clinical, radiological, and histopathological findings alone are insufficient to distinguish between tuberculosis and sarcoidosis.
Abstract
Differential diagnosis of peripheral lymphadenopathies is important in terms of not missing infections or non-infectious diseases and early diagnosis of malignancies. Preliminary diagnoses of tuberculosis, sarcoidosis, and malignancy were considered for two clinically similar patients, a 33-year-old man and a 41-year-old woman, who presented to our clinic with neck swelling. The male patient's exposure to tuberculosis and the chest x-ray brought us closer to the diagnosis of tuberculosis reactivation. The female patient's multiple peripheral lymphadenopathies and metastasis-suspicious lesions seen on positron emission tomography increased our suspicion of malignancy. However, in the final diagnostic process, the female patient was diagnosed with tuberculous lymphadenitis, and the male patient was diagnosed with sarcoidosis. We presented these two cases to show that it isn't always easy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
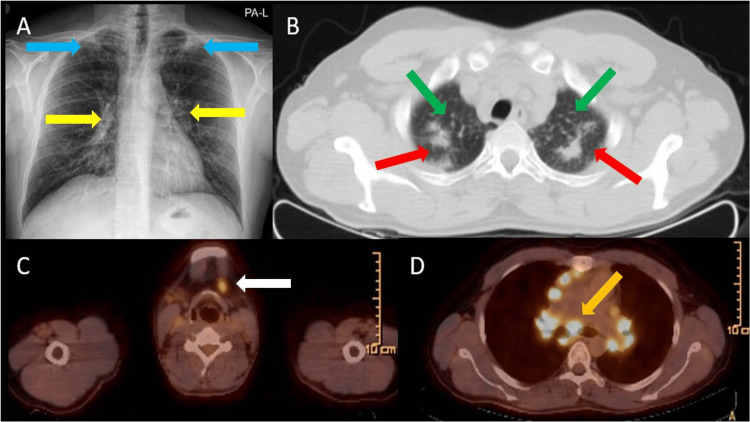 Figure 1
Figure 1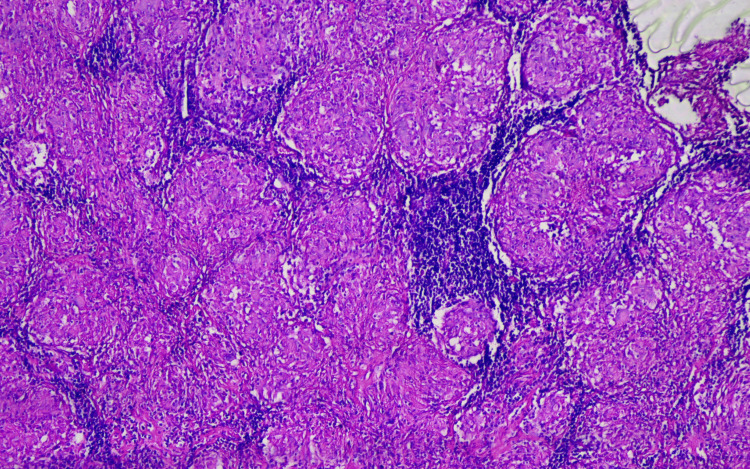 Figure 2
Figure 2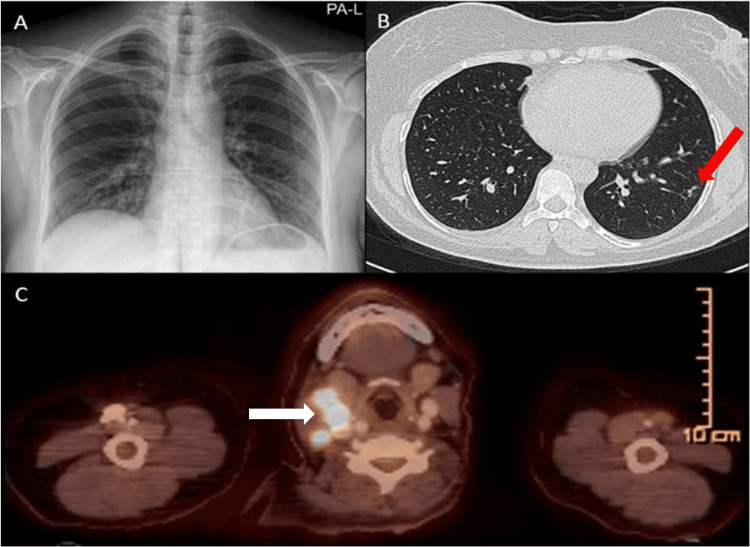 Figure 3
Figure 3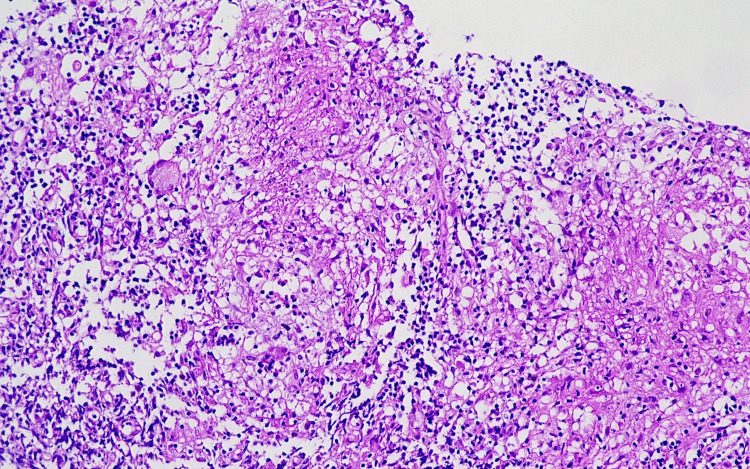 Figure 4
Figure 4| Parameter | Case 1 – Sarcoidosis | Case 2 – Tuberculous Lymphadenitis |
| Age, Sex | 33 years, Male | 42 years, Female |
| Main Symptoms | Fatigue, night sweats, productive cough, sputum | Fatigue, low-grade fever, rapidly enlarging lymph nodes |
| Family History | Father with history of pulmonary TB | No remarkable family history |
| Lymphadenopathy | Bilateral hilar, mediastinal, cervical | Cervical and mediastinal |
| Laboratory Findings | Elevated ACE, normal inflammatory markers, normal tumor markers | Normal ACE, mildly elevated inflammatory markers, normal tumor markers |
| Imaging (X-ray, CT, PET) | Centrilobular nodules, bilateral hilar LAD, moderate FDG uptake | Multiple hypermetabolic lymph nodes, moderate FDG uptake, no lung lesions |
| Histopathology (excisional lymph node biopsy) | Non-caseating granulomas | Non-caseating granulomas |
| Microbiology (tissue culture) | All cultures and PCR negative for TB | Culture positive for Mycobacterium tuberculosis |
| Final Diagnosis | Sarcoidosis | Tuberculous lymphadenitis |
| Timeline | Gradual onset, symptoms resolved spontaneously without anti-TB therapy | Progressive symptoms until anti-TB therapy initiated |
| Response to Therapy | Follow up without systemic corticosteroid therapy | Resolution after anti-TB therapy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Infectious Diseases and Tuberculosis · Diagnosis and treatment of tuberculosis
Introduction
The human body contains approximately 600 lymph nodes. Peripheral lymph nodes are located in the subcutaneous tissue and can be palpated when pathological processes cause them to enlarge. Lymphadenopathy (LAP) refers to conditions in which lymph nodes become abnormal in size, consistency, or number [1,2].
The differential diagnosis of peripheral LAP is crucial for the early detection and management of infectious and non-infectious diseases, and for not overlooking malignancies. LAP may result from a variety of causes, including tuberculosis (TB), sarcoidosis, and malignancies, all of which can present with overlapping clinical features. Initial evaluation typically includes a detailed clinical assessment and radiological examination of the head and neck. When findings suggest an inflammatory origin, further investigations such as microbiological and serological tests, as well as fine-needle aspiration biopsy or excisional biopsy, are required to establish a definitive diagnosis [1-3].
In this report, we present two patients from Türkiye with similar clinical complaints and a preliminary suspicion of TB, sarcoidosis, or malignancy, aiming to compare the diagnostic processes. Considering the global burden of TB and the relatively rare but increasingly recognized incidence of sarcoidosis in Türkiye, these cases highlight the challenges in differentiating between these conditions.
Case presentation
Case 1
A 33-year-old male patient presented with a swelling in his neck that he noticed two days ago. He also had symptoms of sputum, night sweats, and cough for five days. It was learned that the patient didn’t smoke and had no other disease, but his father had a history of TB. The patient was working as a teacher.
On physical examination of the patient, whose vital signs were normal, there was a firm, mobile lymphadenopathy in the right submandibular area measuring approximately 2 cm in diameter. The lymph node was not matted, and the overlying skin appeared normal. Crackles were heard in the lung apices on auscultation. Ophthalmologic examination was also performed and revealed no ocular involvement.
A chest x-ray was taken (Figure 1A). The patient's thorax computed tomography (CT) showed lymph nodes in the mediastinum and bilateral hilar regions, the largest of which was 31x19 mm, which could be compatible with an enlarged granulomatous lesion. Parenchymal changes were evaluated as post-TB fibrotic changes, predominantly affecting both upper lobes (Figure 1B).
Imaging findings in Case 1(A) Chest X-ray shows infiltrate areas in the upper regions (blue arrows) and bilateral hilar fullness (yellow arrows); (B) CT shows, at the apex level of both lungs, areas of post-tuberculosis fibrotic changes (red arrows) and millimetric centrilobular scattered nodules in the upper lobes of both lungs (green arrows); (C) PET/CT shows hypermetabolic lymph nodes in the deep cervical region bilaterally, the largest on the left being 1.5 cm (SUVmax: 4.54) (white arrow); (D) PET/CT shows many hypermetabolic lymph nodes; the largest in the subcarinal region is 4 cm (SUVmax: 13.1) (orange arrow).SUVmax: maximum standardized uptake value
The patient's blood values were normal except that the angiotensin-converting enzyme (ACE) level was 103 U/L (normal range 12-82 U/L). Tumor markers, including carcinoembryonic antigen (CEA), cancer antigen 125 (CA-125), and cancer antigen 19-9 (CA 19-9), were within normal limits. With the suspicion of TB, sputum culture, acid-fast bacilli (AFB), and tuberculin skin test (PPD) were performed. The PPD was positive, but AFB results were negative, and no growth was observed in the sputum culture.
Due to suspicion of malignancy, a positron emission tomography (PET)/CT scan was performed, which revealed multiple hypermetabolic lymph nodes in the head and neck region, thorax, abdomen, and inguinal area (Figures 1C, 1D). The patient declined bronchoscopy and endobronchial ultrasound (EBUS) procedures and was referred to the ear, nose, and throat clinic for a biopsy.
The excisional biopsy taken from the left cervical region resulted in non-caseating granulomatous lymphadenitis, and there was no growth in tissue culture (Figure 2).
Histopathological findings in Case 1Non-caseating granulomas are seen disrupting the normal structure of the lymph node. Multinucleated giant cells are visible. 200x, H&E.
The patient was diagnosed with Stage 1 sarcoidosis. Given the absence of progressive symptoms or significant organ involvement, the patient was followed up without systemic corticosteroid therapy. The patient was monitored every three months for 24 months, with no clinical or radiological progression observed.
Case 2
A 41-year-old female patient was admitted with complaints of neck swelling, joint pain, palpitations, weight loss, fatigue, night sweats, cough, and white sputum for a week. She had never smoked, didn't have any chronic diseases, and was working as a farmer.
On physical examination, multiple bilateral submandibular and cervical lymphadenopathies were palpated, ranging between 1.5 to 2 cm in size. The nodes were soft, discrete, and mobile, with no signs of matting or tenderness. Ophthalmologic examination showed normal findings, with no evidence of ocular involvement. X-ray (Figure 3A) and high-resolution CT (HRCT) of the lungs (Figure 3B) were done.
Imaging findings in Case 2(A) No pathological area observed in chest X-ray; (B) HRCT shows several millimetric nodules in the peripheral area (red arrow); (C) PET/CT shows multiple hypermetabolic lymph nodes; most notably 16 mm (SUVmax: 14.27) in the right level IIa (white arrow).HRCT: high-resolution computed tomography; SUVmax: maximum standardized uptake value
In the laboratory work-up, C-reactive protein (CRP) was 12.6 mg/L, and erythrocyte sedimentation rate (ESR) was 20 mm/hour. Tumor markers, including CEA, CA-125, and CA 19-9, were within normal limits. ACE level was measured at 44 U/L. The PPD was positive, but the sputum culture and AFB results were negative.
To investigate the malignancy, a PET/CT scan was performed, which revealed multiple hypermetabolic lymph nodes in the head and neck region with suspected metastasis (Figure 3C). The patient was referred to the ear, nose, and throat clinic for a biopsy, but she declined the bronchoscopy and EBUS.
The excisional biopsy result taken from the right submandibular region also resulted in lymphoid tissue accompanied by non-caseating granulomas. However, the patient's tissue culture resulted in Mycobacterium tuberculosis Complex (Figure 4). Histopathologically, a diagnosis of grade II (non-caseating epithelioid granulomatous reaction) tuberculous lymphadenitis was made.
Histopathological findings in Case 2Abortive granulomas in a trucut biopsy of the lymph node. A multinucleated giant cell is observed on the left. 200x, H&E.
Based on clinical findings and imaging, the patient was classified as having Stage 2 (uncomplicated) tuberculous lymphadenitis, as there were no signs of abscess formation, fistula, or sinus tract, and the disease was confined to peripheral lymph nodes. She was started on standard anti-tuberculosis therapy in accordance with the American Thoracic Society (ATS) guidelines, with an intensive phase of two months using isoniazid, rifampin, pyrazinamide, and ethambutol (HRZE), followed by a continuation phase of four months with isoniazid and rifampin (RH). Clinical improvement was noted after two months, including regression in lymph node size and resolution of systemic symptoms. A complete cure was achieved after the six-month standard anti-tuberculosis therapy. The patient was monitored monthly during treatment and subsequently every six months for a total of 24 months, with complete clinical and radiological resolution observed and no recurrence reported.
Comparison
For ease of comparison, Table 1 provides a side-by-side summary of the key clinical, laboratory, imaging, histopathological, and microbiological features of the two cases, highlighting the diagnostic decision-making process.
Discussion
TB and sarcoidosis are chronic, multi-systemic, granulomatous diseases that have similar pulmonary and extra-pulmonary manifestations. Since both diseases have common clinical, radiological, and histological features, differential diagnosis is not always easy [4]. Especially in countries with a high burden of TB, differential diagnosis from sarcoidosis is difficult clinically [5]. Our study highlights the importance of a comprehensive, multimodal approach combining clinical findings, imaging, pathological, and microbiological testing.
Systemic symptoms such as fever, night sweats, fatigue, and weight loss are commonly observed in both sarcoidosis and TB lymphadenitis; however, as these two diseases significantly overlap, distinguishing them based solely on clinical symptoms is impractical, and any differences should be considered only as a reference rather than a definitive means of differentiation. TB often presents with more pronounced infectious symptoms, including productive cough and purulent sputum [6], as in our first case. In contrast, sarcoidosis typically manifests with more subtle constitutional symptoms such as dry cough, fatigue, and occasionally arthralgia or erythema nodosum [7].
In Case 1, the presence of purulent sputum, chronic cough, and constitutional symptoms raised a strong suspicion of pulmonary TB. However, microbiological investigations, including AFB staining and culture, were negative, and the patient's symptoms gradually resolved without anti-TB treatment during follow-up, further supporting the diagnosis of sarcoidosis. Case 2, on the other hand, presented with similar constitutional symptoms but also had rapidly enlarging lymphadenopathy. Despite initial suspicion of malignancy, culture confirmed TB lymphadenitis. These contrasting presentations reflect the clinical ambiguity often encountered in differentiating the two entities.
Although elevated ACE levels are known to support the diagnosis of sarcoidosis, their diagnostic utility is limited by variable sensitivity and specificity [8]. Laboratory findings provided supportive, but not definitive, clues in differentiating between the two conditions. In Case 1, ACE was elevated while all other routine blood tests were within normal ranges; tumor markers were also normal, helping to exclude malignancy. In Case 2, inflammatory markers were mildly elevated, while the ACE level was within normal limits, and tumor markers were again unremarkable. Although none of these laboratory findings are pathognomonic, when interpreted alongside radiologic and histopathologic features, they contributed meaningfully to the diagnostic reasoning in both patients.
Tuberculin skin testing (PPD) and interferon-gamma release assays (IGRAs) are frequently used to support TB diagnosis, but both have limitations. PPD has reduced specificity in Bacillus Calmette-Guérin(BCG)-vaccinated populations and in regions with prevalent environmental mycobacteria. IGRA offers higher specificity (~95%) but variable sensitivity, particularly in extrapulmonary or latent TB [9]. Both patients in this report had positive PPD results, which were considered likely related to their residence in a TB-endemic region such as Türkiye. In our setting, IGRA was not available, which represents one of the limitations of our study. However, given the diagnostic limitations of both PPD and IGRA, and the absence of microbiological confirmation, these findings were not sufficient to establish a definitive diagnosis.
Imaging plays a crucial role in differential diagnosis, though findings may be nonspecific. In TB, reactivation typically manifests as centrilobular nodules, tree-in-bud opacities, and fibronodular infiltrates predominantly in the upper lobes [10]. In contrast, sarcoidosis commonly demonstrates bilateral hilar and mediastinal lymphadenopathy, perilymphatic nodules, and, in advanced stages, parenchymal fibrosis [11]. In Case 1, chest X-ray demonstrated bilateral hilar lymphadenopathy, while CT imaging revealed centrilobular nodules and fibrotic changes in the upper lobes. The parenchymal abnormalities were interpreted as post-TB fibrotic changes; however, the presence of bilateral hilar lymphadenopathy, in the absence of microbiological evidence of active infection, supported the diagnosis of sarcoidosis. In Case 2, the absence of significant parenchymal involvement but the presence of progressively enlarging peripheral lymph nodes necessitated further investigations to clarify the underlying pathology. Overall, these findings highlight that both chest X-ray and CT can suggest possible differential diagnoses, yet often pose diagnostic challenges without microbiological or histopathological confirmation.
It is known that FDG uptake seen in PET/CT is not disease specific and can be increased in both benign and malignant lymphoproliferative processes [12]. In Case 1, PET/CT showed hypermetabolic lymph nodes in the bilateral deep cervical region and additional hypermetabolic nodes in the mediastinal region. Although such FDG-avid lymphadenopathy can raise suspicion for malignancy, it is also well-documented in both TB and sarcoidosis. In Case 2, PET/CT demonstrated multiple hypermetabolic lymph nodes without pulmonary involvement, a pattern that can be seen in both sarcoidosis and extrapulmonary TB. These findings underscore the limited specificity of FDG uptake in distinguishing between granulomatous and malignant etiologies [13,14]. Thus, while PET/CT was valuable in lesion detection, it did not establish etiology without histopathological and microbiological correlation.
Histopathological analysis remains essential in evaluating granulomatous diseases. Granulomatous inflammation is a hallmark of both sarcoidosis and TB, yet they exhibit key histopathological differences. While non-caseating granulomas are characteristic of sarcoidosis, TB often presents with caseous necrosis. However, this distinction is not absolute. It is well-documented that up to 30% of TB lymphadenitis cases may demonstrate non-caseating granulomas, particularly in immunocompetent individuals [15]. As seen in our cases, both biopsies revealed non-caseating granulomas. The presence of multinucleated giant cells in both cases further highlights the shared immune-mediated nature of granulomatous inflammation in these diseases. In Case 1, despite clinical and radiological suspicion, all microbiological tests were negative, supporting a diagnosis of sarcoidosis. In Case 2, culture of biopsy material confirmed TB. Therefore, histopathology alone is insufficient for definitive diagnosis, and microbiological confirmation is indispensable [16]. These findings emphasize the importance of tissue diagnosis in combination with microbiological studies.
As extra-pulmonary manifestations, ocular involvement may occur in both TB and sarcoidosis, adding further complexity to the differential diagnosis. Ocular TB most commonly presents as chronic granulomatous uveitis, choroiditis, or retinal vasculitis, and can lead to significant visual morbidity if untreated [17]. Similarly, sarcoidosis is one of the leading causes of non-infectious uveitis worldwide and may present with anterior, intermediate, or posterior uveitis, keratoconjunctivitis sicca, or retinal periphlebitis [7]. In our cases, ophthalmologic examinations were within normal limits, and no ocular involvement was detected. Although the presence of ocular manifestations is not disease-specific, their recognition is important because ophthalmologic evaluation may provide additional diagnostic clues in patients presenting with peripheral lymphadenopathy and suspected granulomatous disease.
While sarcoidosis and TB are distinct granulomatous diseases, rare cases of their coexistence or sequential occurrence have been documented, particularly in TB-endemic regions. Kaur et al. described a patient with concurrent, microbiologically confirmed pulmonary TB and sarcoidosis, underscoring the diagnostic complexity of such presentations [18]. In another case, sarcoidosis was diagnosed during TB treatment, possibly reflecting immune reconstitution or the unmasking of a latent granulomatous process [19]. Furthermore, van Enschot and van Balkom suggested that sarcoidosis may develop as a post-infectious immunological response following TB infection, raising the question of whether sarcoidosis is, in selected cases, a consequence rather than a coincidence [20]. In light of these reports, our first case raises suspicion of a potential association between prior mycobacterial infection and subsequent sarcoidosis. The second case is currently under follow-up for the same reason. To draw more comprehensive conclusions on this topic, further multicenter studies involving larger cohorts are needed. In this report, all diagnoses were supported by both microbiological and histopathological findings, emphasizing the importance of a meticulous differential diagnosis-particularly in TB-endemic settings.
Conclusions
These two cases illustrate the diagnostic challenges in distinguishing TB from sarcoidosis, especially in regions where TB is endemic. Despite overlapping clinical, radiological, and histopathological features, accurate diagnosis requires microbiological confirmation. Clinicians should consider both diseases in the differential diagnosis of peripheral lymphadenopathy and integrate all diagnostic modalities to avoid misdiagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lymphadenopathy: differential diagnosis and evaluation Am Fam Physician Ferrer R 13131320581998 https://www.aafp.org/pubs/afp/issues/1998/1015/p 1313.html 9803196 · pubmed ↗
- 2Peripheral lymphadenopathy: approach and diagnostic tools Iran J Med Sci Mohseni S Shojaiefard A Khorgami Z 158170392014 https://pmc.ncbi.nlm.nih.gov/articles/PMC 3993046/24753638 PMC 3993046 · pubmed ↗
- 3Lymphadenopathy Stat Pearls [Internet] Freeman AM Matto P Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 513250/
- 4Tuberculosis or sarcoidosis: opposite ends of the same disease spectrum?Tuberculosis (Edinb) Agrawal R Kee AR Ang L 21269820162715661410.1016/j.tube.2016.01.003 · doi ↗ · pubmed ↗
- 5Sarcoidosis in tuberculosis-endemic regions: India J Ophthalmic Inflamm Infect Babu K 53320132380355810.1186/1869-5760-3-53PMC 3698001 · doi ↗ · pubmed ↗
- 6Peripheral tuberculous lymphadenitis: epidemiology, diagnosis, treatment, and outcome Medicine (Baltimore) Polesky A Grove W Bhatia G 3503628420051626741010.1097/01.md.0000189090.52626.7a · doi ↗ · pubmed ↗
- 7The clinical features of sarcoidosis: a comprehensive review Clin Rev Allergy Immunol Judson MA 63784920152527445010.1007/s 12016-014-8450-y · doi ↗ · pubmed ↗
- 8Performance of serum angiotensin-converting enzyme in diagnosing sarcoidosis and predicting the active status of sarcoidosis: a meta-analysis Biomolecules Hu X Zou L Wang S Zeng T Li P Shen Y Chen L 14001220223629160910.3390/biom 12101400 PMC 9599650 · doi ↗ · pubmed ↗