Are rural adolescent girls in Senegal more likely to use family planning? DHS 2023 analysis
Ndeye M. Sougou, Cheikh T. Diop

TL;DR
This study finds that rural adolescent girls in Senegal are less likely to use modern contraception, highlighting the need for targeted health interventions.
Contribution
The study identifies rural residence as a key determinant of contraceptive use among Senegalese adolescent girls using 2023 DHS data.
Findings
Only 2.05% of surveyed adolescent girls in Senegal reported using contraception.
Rural residence was associated with lower odds of contraceptive use (AOR = 0.58).
Married adolescents were significantly more likely to use contraception (AOR = 20.61).
Abstract
In Senegal, adolescent reproductive health is a public health priority. The objective of this research is to identify and analyse the key determinants of modern contraceptive uptake among Senegalese adolescents in 2023. The study focused on adolescent family planning in Senegal in 2023. The study draws on secondary data from the 2023 Senegal Demographic and Health Survey. The sample comprised 16 583 women aged 15–49 years. Adolescent girls aged 15–19 years represented 4024 individuals. The analysis included descriptive, comparative and multivariable statistical approaches. The outcome variable was binary, indicating whether or not a modern contraceptive method was used. All analyses were conducted using STATA version 15. Among the adolescent girls surveyed, 19.33% reported having initiated sexual intercourse, with the earliest reported age at sexual debut being 9 years.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
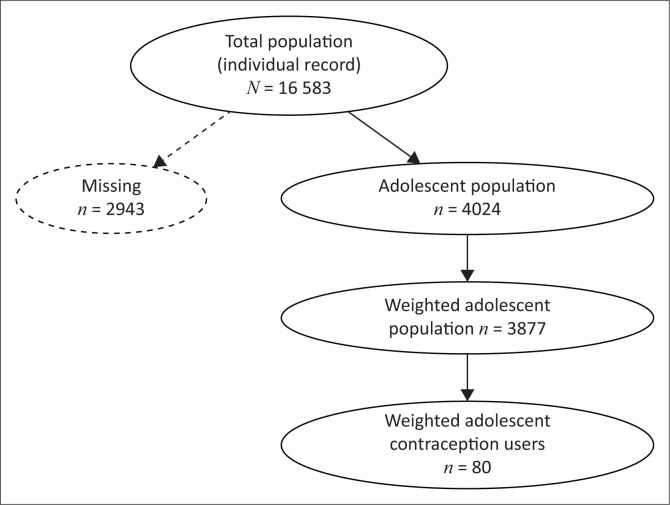 FIGURE 1
FIGURE 1| Age at 1st sexual intercourse (years) |
| % |
|---|---|---|
| No sexual intercourse | 3122 | 80.54 |
| 9 | 1 | 0.03 |
| 10 | 3 | 0.09 |
| 11 | 12 | 0.30 |
| 12 | 13 | 0.34 |
| 13 | 41 | 1.06 |
| 14 | 92 | 2.37 |
| 15 | 161 | 4.15 |
| 16 | 154 | 3.97 |
| 17 | 150 | 3.88 |
| 18 | 97 | 2.51 |
| 19 | 25 | 0.63 |
| Recent sexual activity |
| % |
|---|---|---|
| Never had sex | 3122 | 80.54 |
| Active in the last 4 weeks | 417 | 10.77 |
| Not active in the last 4 weeks – postpartum | 107 | 2.76 |
| Not active in the last 4 weeks – not postpartum | 230 | 5.94 |
| Variable |
| % |
|---|---|---|
|
| ||
| No | 3797 | 97.95 |
| Yes | 80 | 2.05 |
|
| ||
| Pills | 3 | 0.09 |
| Intrauterine device | 2 | 0.04 |
| Injections | 27 | 0.70 |
| Male condom | 3 | 0.07 |
| Interrupted coitus | 2 | 0.04 |
| Traditional method of contraception | 5 | 0.13 |
| Implants or Norplant | 45 | 1.15 |
| Variable | No ( | Yes ( |
| ||
|---|---|---|---|---|---|
|
| % |
| % | ||
|
| - | - | - | - | 0.0214 |
| Urban | 1886 | 48.60 | 28 | 0.07 | - |
| Rural | 1912 | 49.31 | 52 | 1.34 | - |
|
| - | - | - | - | 0.0013 |
| No instruction | 886 | 22.86 | 39 | 1.00 | - |
| Primary | 806 | 20.79 | 17 | 0.43 | - |
| Secondary | 2082 | 53.70 | 24 | 0.61 | - |
| Superior | 23 | 0.59 | 0 | 0.00 | - |
|
| - | - | - | - | < 0.001 |
| The poorest | 580 | 14.97 | 13 | 0.34 | - |
| The poorer | 689 | 17.77 | 28 | 0.73 | - |
| The middle | 800 | 20.63 | 26 | 0.67 | - |
| The richer | 815 | 21.02 | 8 | 0.20 | - |
| The richest | 913 | 23.56 | 3 | 0.09 | - |
|
| - | - | - | - | < 0.001 |
| Has never been in union | 3103 | 80.03 | 12 | 0.31 | - |
| Married | 661 | 17.05 | 66 | 1.69 | - |
| Cohabitation | 1 | 0.03 | 0 | 0.00 | - |
| Widow | 1 | 0.03 | 0 | 0.00 | - |
| Divorced | 25 | 0.64 | 0 | 0.00 | - |
| No longer living with partner/separated | 6 | 0.16 | 2 | 0.04 | - |
|
| - | - | - | - | 0.8355 |
| Muslim woman | 3665 | 94.54 | 78 | 2.00 | - |
| Christian | 129 | 3.33 | 2 | 0.04 | - |
| Animist | 3 | 0.06 | 0 | 0.00 | - |
| Variable | No ( | Yes ( |
| ||
|---|---|---|---|---|---|
|
| % |
| % | ||
|
| - | - | - | - | < 0.001 |
| Does not know any method | 1156 | 29.80 | 0 | 0.00 | - |
| Knows only traditional methods | 8 | 0.25 | 0 | 0.00 | - |
| Knows modern methods | 2631 | 67.87 | 80 | 2.05 | - |
|
| - | - | - | - | < 0.001 |
| No | 3229 | 83.29 | 54 | 1.40 | - |
| Yes | 568 | 14.65 | 25 | 0.65 | - |
|
| - | - | - | - | 0.0450 |
| No | 3057 | 78.85 | 56 | 1.45 | - |
| Yes | 740 | 19.10 | 23 | 0.60 | - |
|
| - | - | - | - | 0.9400 |
| No | 3603 | 92.94 | 76 | 1.95 | - |
| Yes | 194 | 5.01 | 4 | 0.10 | - |
|
| - | - | - | - | 0.1900 |
| No | 3641 | 93.91 | 74 | 1.91 | - |
| Yes | 156 | 4.03 | 6 | 0.14 | - |
|
| - | - | - | - | 0.5600 |
| No | 3456 | 89.15 | 71 | 1.82 | |
| Yes | 341 | 8.80 | 9 | 0.23 | |
|
| - | - | - | - | 0.0062 |
| No | 3425 | 88.36 | 61 | 1.56 | - |
| Yes | 372 | 9.59 | 19 | 0.48 | - |
|
| - | - | - | - | < 0.001 |
| No | 3336 | 86.06 | 55 | 1.41 | - |
| Yes | 461 | 11.89 | 25 | 0.63 | - |
| Characteristics | AOR | 95% CI |
|
|---|---|---|---|
|
| 1.00 | - | - |
|
| |||
| Urban | 1.00 | - | - |
| Rural | 0.58 | 0.34–0.96 | 0.037 |
|
| |||
| No instruction | 1.00 | - | - |
| Primary | 0.94 | 0.54–1.63 | 0.830 |
| Secondary | 1.16 | 0.67–1.99 | 0.580 |
|
| |||
| The poorest | 1.00 | - | - |
| The poorer | 2.35 | 1.35–4.08 | 0.002 |
| The middle | 1.63 | 0.84–3.18 | 0.140 |
| The richer | 1.10 | 0.47–2.58 | 0.810 |
| The richest | 0.68 | 0.19–1.96 | 0.410 |
|
| |||
| Has never been in union | 1.00 | - | - |
| Married | 20.61 | 11.43–37.14 | < 0.001 |
| No longer living with partner or separated | 105.00 | 23.6–467.21 | < 0.001 |
|
| |||
| Muslim woman | 1.00 | - | - |
| Christian | 3.41 | 2.52–18.19 | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Adolescent Sexual and Reproductive Health · Global Health Care Issues
Introduction
Family planning is a proven public health intervention that contributes significantly to reducing maternal and child mortality and enhancing the overall quality of life. Ensuring access to modern contraception for women and girls is not only vital for the health and well-being of individuals but also instrumental in achieving sustainable development, unlocking the economic potential of nations and safeguarding the health of future generations.^1^ Modern contraceptive methods constitute a cornerstone of both primary and reproductive health care. They are essential for enhancing health outcomes among mothers, newborns and children by decreasing disease burden and death rates within these populations, and by helping to limit the spread of human immunodeficiency virus (HIV) and/or acquired immunodeficiency syndrome (AIDS).^2^ Among available interventions, contraception is the principal tool enabling women and girls to exercise control over their reproductive lives, including the timing and spacing of pregnancies.
As of recent estimates, approximately 705 million women in low- and lower-middle-income countries are using contraceptive methods, thereby preventing an estimated 376m unintended pregnancies each year. These preventive measures, in turn, help avert approximately 39m miscarriages, 2m stillbirths, and 131 000 maternal deaths each year.^3^
In Senegal, the legal and policy framework surrounding contraception has evolved significantly over the past few decades. The 1980 abolition of the 1920 law prohibiting the promotion and use of contraception represented a turning point in reproductive health policy,^4^ followed by the integration of family planning services into maternal and child health programmes. In 1988, the government adopted a national population policy with the explicit goals of reducing fertility rates and population growth. Key strategies included the promotion of contraceptive use, the dissemination of family planning methods, and the introduction of population education programmes to prevent adolescent pregnancies.^5^
Despite these efforts, the uptake of modern contraception has shown signs of stagnation in recent years. After rising to 26.3% in 2017, the modern contraceptive prevalence rate (mCPR) fell to 25.4% in 2018, following a plateau in 2016 at 23.7%.^6^ Several studies have identified persistent barriers to contraceptive use, notably sociocultural constraints and weaknesses in the health system.^7,8,9^ However, these studies often overlook other key determinants of health that may influence contraceptive adoption, particularly among adolescents, such as limited knowledge, decision-making autonomy, peer and partner influence, perceived quality of services, and financial accessibility.
Adolescent girls remain a vulnerable population with substantial unmet needs in sexual and reproductive health.^10^ They face numerous obstacles in accessing contraceptive services, including social stigma, limited autonomy, and inadequate youth-friendly services.^11^ While early sexual debut and child marriage remain prevalent among adolescent girls in Senegal, as in many sub-Saharan African countries,^12^ the literature remains limited regarding their specific access to contraception.
It is within this context that the present study aims to examine the determinants of modern contraceptive use among adolescent girls in Senegal in 2023. The findings are expected to inform the development of targeted strategies and interventions tailored to this particularly vulnerable population group.
Research methods and design
Type of study
This was a descriptive cross-sectional study using data from the 2023 Demographic Health Survey (DHS).
Study population
These were teenage girls aged 15–19 years, living in Senegal in 2023.
Inclusion criteria
Teenage girls aged between 15 years and 19 years, residing in Senegal, who were present in the household on the night before the survey.
Eligibility limitations
Individuals who refused to be interviewed were not considered eligible for inclusion.
Survey design
Following DHS standards, a two-stage stratified sampling approach was used to ensure national, regional, and urban and rural representativeness across all 14 regions of Senegal. Sampling was implemented separately within each stratum. During the initial phase of the Senegal DHS sampling process, 400 primary sampling units (PSUs) were systematically selected from Enumeration Zones defined by the Recensement Général de la Population, de l’Habitat, de l’Agriculture et de l’Élevage (RGPHAE) census, using a probability proportional to size method based on the number of households per zone. A count of households in each of these clusters provided a list of households from which a sample of 22 households per cluster was drawn in the second stage, in both urban and rural areas, using a systematic draw with equal probability.
The analysis was based on the Individual Recode dataset, which includes women aged 15–49 years who were present in the household on the night preceding the survey interview.
Variables
The target population for this study consisted of female adolescents aged 15–19 years. The outcome variable analysed was the use of a modern contraceptive method, recorded in the DHS as a binary variable (yes or no).
Several explanatory variables were considered, encompassing individual characteristics, sociodemographic attributes, and economic conditions.
Individual factors
These included the teenager’s marital status (divorced, married, widowed) and her religion.
Sociodemographic and economic factors
The mother’s educational attainment was categorised into four levels: no formal education (referring to those who never attended the French formal school system), primary, secondary, and higher education. The wealth index, a measure of relative economic well-being based on household assets, was classified into quintiles (lowest, second, middle, fourth, highest) and derived from the wealth score. Place of residence (urban versus rural) was also taken into account.
Analysis
Data analysis was performed using STATA/SE version 15.1. As previously described in the data sources section, the study employed a two-stage sampling strategy. To address the complexity of the sampling design, weighting adjustments were applied to correct for unequal selection probabilities and non-response bias.
In the descriptive phase, data were summarised using proportions and absolute counts. The Chi-square test (χ^2^) was employed to evaluate associations between categorical variables. A p-value below 0.05 was considered statistically significant, with 95% confidence intervals [CI] used for precision estimates. Variables with a p-value less than 0.25 in the bivariate analysis were included in the multivariate model, in line with the recommendations of Hosmer and Lemeshow, to avoid excluding potentially important variables that may become significant after adjustment for confounder.^13^
In order to identify factors linked to modern contraceptive use among adolescents, a multivariable logistic regression was conducted, adjusting for potential confounders. Adjusted odds ratios (s) were estimated along with their 95% CIs. Given the survey’s complex design – incorporating stratification, weighting, and clustering – the analysis specified design variables for weights, strata, and PSUs using the svy prefix in STATA.
The survey also identified 16 583 women aged 15–49 years. Teenage girls aged 15–19 years accounted for 4024 individuals. After allocation of the survey weight, they numbered 3077 (see Figure 1 [data flow diagram]).
Diagram of study flow.
Ethical considerations
Ethical clearance to conduct this study was obtained from the ICF Macro Institutional Review Board (No. 31561.00.000.00).
Results
The results presented below provide an overview of the sociodemographic characteristics of the study population and describe patterns of sexual activity and modern contraceptive use among adolescent girls in Senegal. This section also highlights the key factors statistically associated with contraceptive use, based on both descriptive and multivariate analyses.
Sexual behaviour and practices
Adolescent girls who had sexual intercourse accounted for 19.33% (see Table 1). The youngest age recorded for sexual initiation was 9 years (Table 1). A total of 10.77% of adolescent girls had been sexually active in the past 4 weeks (see Table 2).
Method of contraception
Adolescents using a method of contraception accounted for 2.05% (80 adolescents). Of those who were using contraception, more were using long-acting methods such as implants or norplants (1.15%, or 45 adolescents) and injections (0.70%, or 27 adolescents). To a lesser extent, some adolescents were using traditional methods of contraception (0.13%, or 5 adolescents) (see Table 3).
Profile of sociodemographic characteristics by modern contraceptive use
The number of adolescents using family planning is higher in rural areas than in urban areas (52 adolescents, or 1.34%). The proportion of married adolescents using contraception was 1.69%, or 66 out of 80.
Adolescents in the poor and middle wealth quintiles used the most contraceptive methods, with 28 (0.73%) and 26 (0.67%) adolescents, respectively (Table 3).
Adolescents who did not know any method of contraception accounted for 29.8%, or 1156 adolescents. Most participants reported having accessed family planning information through mass media channels such as television and radio as well as printed materials and community-based events (Table 4).
Teenage girls who were unaware of any method of contraception accounted for 29.8%, or 1156 girls. The majority of respondents had obtained information about family planning from television, radio, brochures, or community meetings (Table 5).
Factors associated with the use of contraception by adolescents
Living in a rural area was a protective factor for contraceptive use: AOR = 0.58; 95% CI: 0.34–0.96). Girls living in rural areas were less likely to use a contraceptive method than those living in urban areas. According to the results presented in Table 6, adolescents who were married had significantly higher odds of using modern contraceptive methods compared to their unmarried peers (AOR = 20.61; 95% CI: 11.43–37.14). Similarly, girls who were no longer living with their partners showed an even stronger association with contraceptive use (AOR = 105; 95% CI: 23.6–467.21). In addition, adolescents belonging to the lower economic quintile were more than twice as likely to adopt modern contraception (AOR = 2.35; 95% CI: 1.35–4.08). The likelihood of contraceptive use was also higher among Christian adolescents compared to Muslim girls (AOR = 3.41; 95% CI: 2.52–18.19).
Discussion
The findings of this study underscore a significant gap between the sexual activity of adolescent girls in Senegal and their use of modern contraceptive methods. Although nearly one in five adolescents reported having initiated sexual intercourse – with some as young as age 9 years – current utilisation of modern contraceptive methods was reported by only 2.05% of the adolescents. This discrepancy reflects a broader trend in sub-Saharan Africa, where a growing number of adolescents, particularly from disadvantaged backgrounds, become sexually active at an early age, often without access to adequate reproductive health services.^14^
Compared to other African countries, the level of contraceptive use among Senegalese adolescents remains markedly low. While prevalence among adolescents varies greatly across the continent – from 4% in Chad to over 60% in Namibia – the majority of countries still report rates below 50% among sexually active adolescents.^15^ This indicates persistent structural and social barriers that hinder adolescent access to contraception despite global and national commitments to reproductive health rights.
Notably, in this study, long-acting methods such as implants and injectables were more commonly used among adolescents than oral contraceptives, a pattern that differs from trends in many Western countries where pills remain the preferred method.^16^ This divergence may reflect differences in access, provider preferences, or programmatic emphasis in method provision.
The role of knowledge and perceptions also merits attention. While most respondents reported exposure to family planning messages via mass media and community-based platforms, previous studies have shown that such knowledge alone does not necessarily translate into use.^17^ Access to reliable and youth-adapted information, including discussions about contraceptive options and their side effects, is essential. In Senegal, efforts have been made to include adolescents in national communication strategies, notably through the establishment of a dedicated reproductive health division. However, bridging the gap between awareness and practice remains a challenge.^18,19^
Several factors were found to be associated with contraceptive use. Adolescents residing in rural areas were significantly less likely to use modern contraceptives (AOR = 0.58; 95% CI: 0.34–0.96]). This finding aligns with evidence from other contexts showing greater barriers to access in rural compared to urban settings, including geographic distance, limited availability of youth-friendly services, and provider bias.^20^ Interestingly, adolescents in the lowest wealth quintile were more likely to use contraception (AOR = 2.35; 95% CI: 1.35–4.08), a finding that contrasts with previous studies in older populations where higher socioeconomic status is often linked to increased use.^21^ This may suggest successful targeting of the poorest by public health programmes, but it also raises concerns about potential disparities in method quality and informed choice.
Marital status also played a key role. Married adolescents and those who were separated from their partners were significantly more likely to use modern contraceptives (AOR = 20.61; 95% CI: 11.43–37.14 and AOR = 105; 95% CI: 23.6–467.21, respectively). Similar trends have been observed in other studies, which attribute this to stronger social networks and community structures that facilitate access to services among married adolescents.^22,23^
Religious affiliation appeared as another important factor. Christian adolescents were more likely to use contraception than their Muslim peers (AOR = 3.41; 95% CI: 2.52–18.19). While religion itself may not directly oppose family planning, the interpretation of religious norms and their perceived compatibility with contraceptive use often shape individual behaviour.^24,25^ In this context, engaging religious leaders and integrating culturally sensitive messaging into health promotion efforts may help reduce resistance and misperceptions.
In sum, these findings highlight the multifactorial nature of contraceptive use among adolescent girls. Addressing the unmet need for contraception in this population requires tailored interventions that are sensitive to social, economic, cultural, and geographic determinants. Programmes should not only ensure the availability of contraceptive methods but also create enabling environments where adolescents can make informed and autonomous decisions about their reproductive health.
Strengths and limitations
One notable strength of this study is the use of data from the Senegal DHS, which provides nationally representative estimates. This enhances the external validity of the findings, allowing for generalisation to the broader population of adolescent girls of reproductive age in Senegal. Nonetheless, the study is subject to certain limitations.
Given that the analyses were based on cross-sectional data, the findings reflect associations rather than causal relationships. To deepen the understanding of factors influencing adolescents’ use of modern contraception, a complementary qualitative study could help capture the social dynamics and contextual realities that shape their behaviours.
Conclusion
This study provides critical insights into the persistently low use of modern contraceptive methods among adolescent girls in Senegal, despite early sexual debut and relatively widespread exposure to family planning information. The findings emphasise the need for a nuanced and multidimensional approach to adolescent reproductive health, one that goes beyond awareness campaigns to address deeper sociocultural, economic and systemic barriers. Tailored interventions should prioritise equitable access to youth-friendly contraceptive services, particularly for unmarried adolescents, those living in rural areas, and those from disadvantaged backgrounds. Efforts to engage communities – including parents, partners and religious leaders – are essential to fostering an environment that supports adolescent autonomy and informed decision-making.
By centring adolescent girls in the design and delivery of reproductive health programmes, Senegal can accelerate progress towards its national and international commitments on sexual and reproductive health while also advancing gender equity and health outcomes for future generations. In addition to programmatic responses, future research should incorporate qualitative socio-anthropological approaches to explore and better understand the sociocultural norms, perceptions and community-level dynamics that hinder contraceptive uptake among adolescents. Such perspectives are essential to designing interventions that are not only evidence-based but also socially acceptable and culturally embedded.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lancet T. Family planning: Accelerating the way ahead. Lancet. 2017;390(10112): 2527. 10.1016/S 0140-6736(17)33247-629231824 · doi ↗ · pubmed ↗
- 2Titiyos A, Mehretie Y, Alemayehu YK, et al. Family planning integration in Ethiopia’s primary health care system: A qualitative study on opportunities, challenges and best practices. Reprod Health. 2023;20(1):176. 10.1186/s 12978-023-01709-638041131 PMC 10693018 · doi ↗ · pubmed ↗
- 3Askew I, Raney L, Kerrigan M, Sridhar A. Family planning saves maternal and newborn lives: Why universal access to contraception must be prioritised in national maternal and newborn health policies, financing, and programs. Int J Gynecol Obstetr. 2024;164(2):536–540. 10.1186/s 12978-023-01709-637740702 · doi ↗ · pubmed ↗
- 4Government of Senegal. LOI N° 1980 49 DU 24 DÉCEMBRE 1980.pdf [Law No. 1980-49 of 24 December 1980] [homepage on the Internet]. [cited 2024 Jan 09]. Available from: https://www.dri.gouv.sn/loi-n°-198049-du-24-décembre-1980
- 5WHO, USAID. Repositioning family planning: Advocacy guidelines [homepage on the Internet]. Geneva; 2008 [cited 2015 Feb 04]. Available from: www.who.int/reproductive-health/family_planning/index.html
- 6Senegal. EDS Report 20189 [homepage on the Internet]. 2018 [cited 2024 Jan 16]. Available from: https://dhsprogram.com/pubs/pdf/FR 367/FR 367.pdf
- 7Kaur S, Blumenthal PD. Global myth busting in family planning. Curr Opin Obstet Gynecol. 2021;33(6):458–462. 10.1097/GCO.000000000000075734747882 · doi ↗ · pubmed ↗
- 8Cohen N, Mendy FT, Wesson J, et al. Behavioral barriers to the use of modern methods of contraception among unmarried youth and adolescents in eastern Senegal: A qualitative study. BMC Public Health. 2020;20(1): 1025. 10.1186/s 12889-020-09131-432600290 PMC 7325306 · doi ↗ · pubmed ↗