A Tragic Case of Orbital Cellulitis in an Immunocompromised Patient
Chin Ling Tan, Nur Afzan Mohd Jaffar

TL;DR
A 42-year-old man with undiagnosed HIV developed severe orbital cellulitis and died despite treatment, highlighting the risks in immunocompromised patients.
Contribution
This case report emphasizes the importance of recognizing orbital cellulitis as a potential sign of disseminated HIV infection.
Findings
The patient presented with orbital cellulitis and sepsis, later diagnosed with HIV.
Immunocompromised status was indicated by low white cell count and neutropenia.
Despite treatment, the patient experienced multiorgan failure and died.
Abstract
Immunocompromised patients are prone to opportunistic infections. Orbital infections are most likely to occur in advanced stages of acquired immunodeficiency syndrome (AIDS) and are associated with a high mortality rate, making prompt diagnosis and intervention critical. This case report describes a 42-year-old man, previously without known medical conditions, who presented to the Ophthalmology Department with a two-day history of swelling in his right eye. Additional symptoms included a productive cough with greenish sputum for two weeks and constitutional symptoms for one week. Examination revealed features of right orbital cellulitis and diminished optic nerve function. In addition, he had multiple tattoos all over his body with numerous pustules appearing on the forehead and lower limbs. He was clinically septic with rapidly deteriorating vital signs. Laboratory findings indicated a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1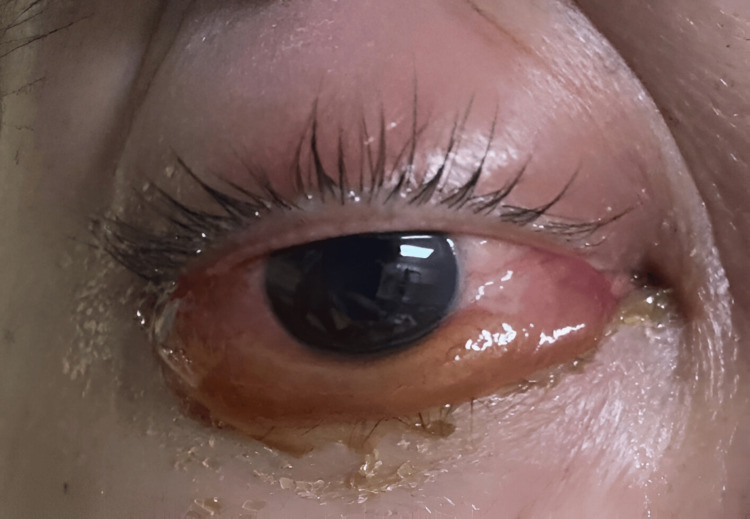 Figure 2
Figure 2 Figure 3
Figure 3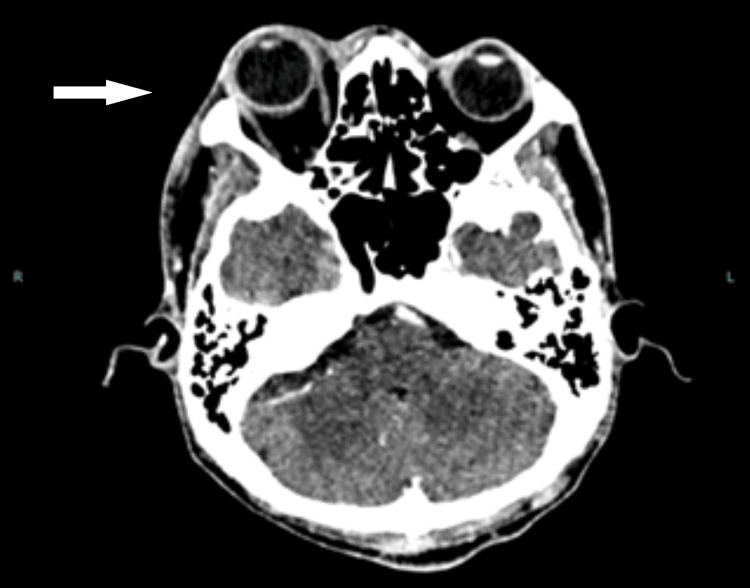 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Sinusitis and nasal conditions · Otitis Media and Relapsing Polychondritis
Introduction
Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) are major public health issues globally. According to the latest updates from the World Health Organization (WHO), approximately 40.8 million people were living with HIV at the end of 2024 globally. Of these, there were approximately 630,000 deaths. In 2024 alone, 1.3 million people were diagnosed with HIV [1].
Orbital manifestations in AIDS patients are infrequent [2-5]. The most common presentations include orbital cellulitis, Kaposi sarcoma, and non-Hodgkin lymphoma [3]. The prevalence of these conditions is highly dependent on the CD4 count of patients. Orbital infections are most likely to occur in advanced stages of AIDS and are associated with a high mortality rate [2].
Case presentation
A 42-year-old man, previously without known medical conditions, presented to the Ophthalmology Department of Sarawak General Hospital with a two-day history of swelling in his right eye (RE) (Figure 1). Additional symptoms included a productive cough with greenish sputum for two weeks and constitutional symptoms such as loss of weight and loss of appetite for a week.
Right eye periorbital swelling with proptosis and skin pustule over the forehead
The presenting visual acuity of the RE was 6/18 and 6/12 with pinhole, while that of the left eye (LE) was 6/9. RE had relative afferent pupillary defect. The anterior segment of the RE showed erythematous and swollen lid and injected conjunctiva with generalized chemosis, which was more prominent inferiorly (Figure 2). There was no anterior chamber cellular activity. The anterior segment of the LE was unremarkable. Intraocular pressure of the RE was raised (32 mmHg), whereas it was normal over the LE. The Ishihara test revealed a color defect over the RE. RE extraocular movement was limited at all gazes, while it was normal over the LE. Fundus examination of both eyes was unremarkable. There was no optic disc swelling or choroidal folds detected. The diagnosis of right orbital cellulitis was made in keeping with these clinical ocular features.
Right eye generalized chemosis which was more prominent inferiorly
Systemic examination revealed multiple tattoos all over his body with numerous pustules on the forehead (Figure 1) and lower limbs. There were whitish patches on the tongue. Lung auscultation revealed coarse crepitus over the bilateral midzone. The chest X-ray (CXR) showed generalized ground-glass opacities (Figure 3).
Chest X-ray showing generalized ground-glass opacities over both lung fields
The patient was found to be tachypneic and tachycardic the next day. He was immediately referred to the medical team in view of rapidly declining clinical signs and suspicion of a systemic immunocompromised state. Despite these alarming signs, the patient was not treated adequately.
Laboratory findings indicated a low total white cell count of 0.57 (10^3^/µL), neutropenia, and lymphopenia, undoubtedly confirming the immunocompromised state. A rapid HIV test yielded a positive result. He was subsequently referred to the infectious disease team. The diagnosis was revised to severe HIV infections with multiple organ involvement, including orbital cellulitis, pneumonia, oral candidiasis, and skin infections. He was then commenced on intravenous piperacillin/tazobactam, cloxacillin, and fluconazole to treat the polymicrobial infections.
Contrast-enhanced computed tomography (CECT) of the brain and orbit during the initial presentation showed thickening and enhancement of the right globe wall with pre-scleral fat streakiness. The fat stranding was also observed in the pre- and post-septal regions and the retroorbital fat, all of which were suggestive of right orbital cellulitis and posterior scleritis. There was minimal mucosal thickening over the bilateral ethmoid and maxillary sinuses (Figure 4). There were no focal brain lesions or features of cavernous sinus thrombosis.
Thickening and enhancement of the right globe wall with pre-scleral fat streakiness. Right eye proptosis. Ethmoid sinuses were clear
Nasal endoscopy by the otolaryngologist (ear, nose, and throat (ENT)) team revealed clear sinuses, ruling out sinusitis as the cause of orbital cellulitis.
Subsequent investigations revealed a CD4 count of 6 cells/µL, and syphilis serology was positive. Other infectious screenings, such as cytomegalovirus polymerase chain reaction (CMV PCR), hepatitis B, and hepatitis C, were negative. Blood culture grew Staphylococcus aureus. Serum cryptococcal antigen was positive.
Despite aggressive treatment, the patient's clinical status rapidly declined. Eventually, he succumbed to multiorgan failure.
Discussion
AIDS patients are prone to opportunistic infections, which frequently involve the anterior and posterior segments of the eye. They rarely involve the orbit [2]. A study by Moraes found that around 25% of untreated HIV patients presented with adnexal and orbital manifestations [3]. Another study by Hothi et al. showed that the prevalence of ocular manifestations in HIV patients receiving highly active antiretroviral therapy (HAART) was 39%. Among these patients, 20% had adnexal involvement, 28% anterior segment involvement, 33% posterior segment involvement, 11% neuro-ophthalmic abnormalities, and 4% orbital involvement [4]. Orbital cellulitis accounts for less than 1% of the cases, which is a rare condition [3,5].
The commonest cause of orbital cellulitis in immunocompetent patients is bacterial sinusitis, which often originates from the ethmoid and maxillary sinuses [2]. Other predisposing factors include recent facial trauma, a history of dental procedures, and hematogenous spread from opportunistic infections [5,6]. Common causative organisms include Staphylococcus aureus (50%) [5], Streptococcus pyogenes, and Streptococcus pneumoniae. Others include fungi such as Aspergillus and mycobacteria [2,5]. Based on a case series by Mansour, Staphylococcus aureus infection is twice as common in HIV patients as compared to healthy individuals [7]. This patient most likely acquired orbital cellulitis through hematogenous spread from Staphylococcus aureus infection, evidenced by a positive blood culture. Sinusitis was ruled out by the nasal endoscope.
According to Meyer and Smit, polymicrobial infections are present in 38.1% of cases, often spreading via the hematogenous route (25.4%) [5]. Half of the patients with orbital cellulitis died within one year of the infection, usually due to invasive Aspergillus fumigatus infection with intracranial extension [2,5]. They typically have a low CD4 lymphocyte count, which is less than 100 cells/mm³, and are often associated with neutropenia [2,5]. This patient had a very low CD4 count with neutropenia. He was suspected of having polymicrobial infections in view of his severe immunocompromised state.
Broad-spectrum antibiotics should be considered, including antibacterials, such as vancomycin, ceftriaxone, cefotaxime, ampicillin-sulbactam, piperacillin-tazobactam, and metronidazole, and anti-fungal, such as fluconazole [5,8]. This patient was given intravenous piperacillin/tazobactam, cloxacillin, and fluconazole. Clinically, the orbital cellulitis responded well to the antibiotic regimes, and the chemosis and proptosis resolved by the second day of treatment.
Conclusions
Orbital cellulitis is a rare presentation of opportunistic infection in immunocompromised patients. Prompt recognition of orbital cellulitis in immunocompromised patients is imperative, as it may signify disseminated HIV infection and carry substantial morbidity and mortality risks. This case underscores the importance of early and appropriate intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1HIV 7 2025 2025 https://www.who.int/data/gho/data/themes/hiv-aids
- 2Orbital infections in patients with human immunodeficiency virus infection Ophthalmology Kronish JW Johnson TE Gilberg SM Corrent GF Mc Leish WM Scott KR 148314921031996884131010.1016/s 0161-6420(96)30479-x · doi ↗ · pubmed ↗
- 3Ocular manifestations of HIV/AIDS Curr Opin Ophthalmol Moraes HV Jr 3974031320021244184410.1097/00055735-200212000-00010 · doi ↗ · pubmed ↗
- 4A prevalence study of ocular manifestations in HIV positive patients on highly active anti-retroviral therapy Biomed Res Clin Prac Hothi HS Gohil NR Parekh NV Patel SS 42019
- 5Eyelid and orbital involvement in HIV infection - an African perspective Ocul Immunol Inflamm Meyer D Smit DP 10221030282020 https://pubmed.ncbi.nlm.nih.gov/32058857/3205885710.1080/09273948.2019.1705987 · doi ↗ · pubmed ↗
- 6Common orbital infections ~ state of the art ~ part IJ Ophthalmic Vis Res Hamed-Azzam S Al Hashash I Briscoe D Rose GE Verity DH 175182132018 https://pubmed.ncbi.nlm.nih.gov/29719647/2971964710.4103/jovr.jovr_199_17PMC 5905312 · doi ↗ · pubmed ↗
- 7Adnexal findings in AIDS Ophthalmic Plast Reconstr Surg Mansour AM 27327991993830537510.1097/00002341-199312000-00008 · doi ↗ · pubmed ↗
- 8Orbital cellulitis Stat Pearls [Internet] Danishyar A Sergent SR Treasure Island (FL)Stat Pearls Publishing 2023 http://pubmed.ncbi.nlm.nih.gov/2993967829939678 · pubmed ↗