A Case of Severe Refractory Immune Thrombocytopenia Exacerbated by Respiratory Syncytial Virus Infection
James Kim, Vicken Khazar, Rebecca E McIver, Benjamin Ascherman, Maria J Nieto

TL;DR
A healthy adult developed severe, treatment-resistant immune thrombocytopenia possibly worsened by a respiratory syncytial virus infection.
Contribution
This is a rare case report of severe ITP exacerbated by RSV in an otherwise healthy adult.
Findings
The patient's thrombocytopenia was refractory to standard treatments like IV immunoglobulin and steroids.
Platelet counts normalized only after cyclosporine treatment.
RSV infection may have played a role in exacerbating the ITP.
Abstract
Immune thrombocytopenia (ITP) is an immunological phenomenon in which antibodies target platelet surface proteins, resulting in platelet destruction, as well as platelet opsonization and clearance by splenic and hepatic macrophages. Antibodies and cytotoxic T cells may also directly target megakaryocytes in the bone marrow, thereby compromising platelet production and further lowering platelet counts. This disease is largely idiopathic but may also result secondary to autoimmune disorders, malignancies, medication side effects, and recent infections. Currently, the understanding of infections and thrombocytopenia is poorly understood. There are no current well-described reports of severe ITP exacerbations due to respiratory syncytial virus (RSV) infection, especially in a relatively healthy adult with no significant hematologic or oncologic history. This case report describes a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
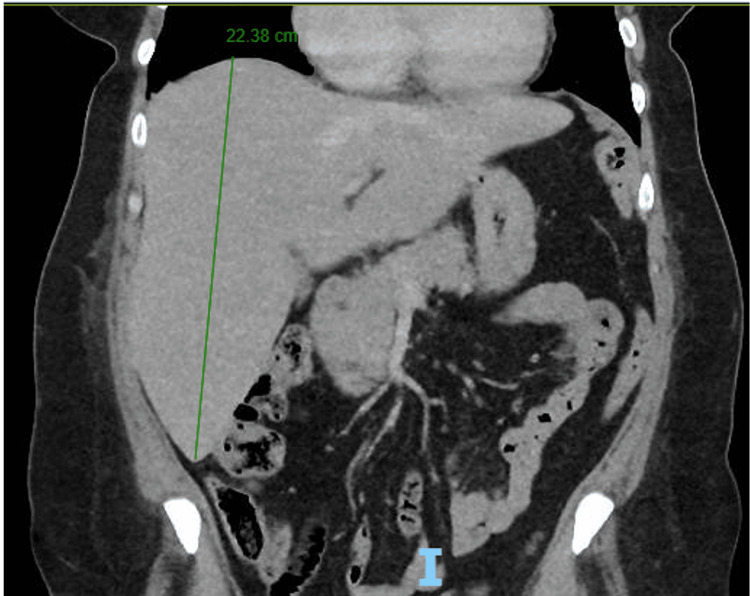 Figure 1
Figure 1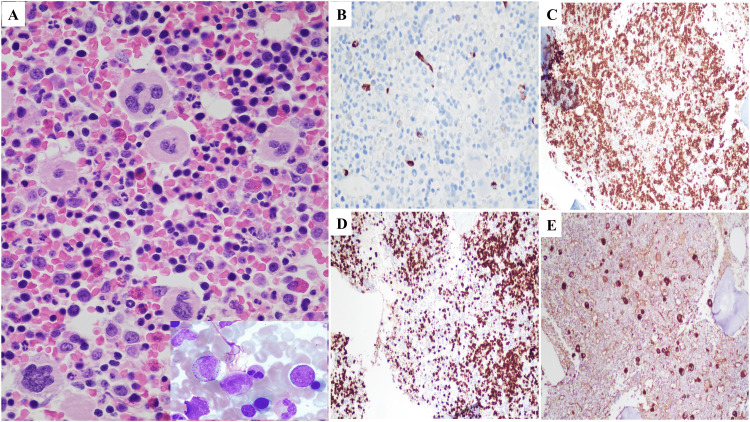 Figure 2
Figure 2| Laboratory test parameter | Value | Reference range |
| WBC | 20.01 | 3.8-10.5 K/μL |
| Neutrophil (%) | 82.10 | 43%-77% |
| Hemoglobin | 2.5 | 11.5-15.5 g/dL |
| Hematocrit | 10.90 | 34.5%-45% |
| Mean cell volume | 67.3 | 80-100 fL |
| Platelets | 7 | 150-400 K/μL |
| Uric acid | 8.2 | 2.5-7 mg/dL |
| LDH | 566 | 50-242 U/L |
| AST | 252 | 10-40 U/L |
| ALT | 222 | 10-45 U/L |
| Iron | 24 | 30-160 µg/dL |
| TIBC | 334 | 220-430 µg/dL |
| % saturation, iron | 7 | 14%-150% |
| Ferritin | 22 | 13-330 ng/mL |
| Haptoglobin | 86 | 34-200 mg/dL |
| Reticulocyte percent | 11.20 | 0.5%-2.5% |
| Absolute reticulocytes | 170.9 | 25-125 K/μL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPlatelet Disorders and Treatments · Blood groups and transfusion · Immunodeficiency and Autoimmune Disorders
Introduction
Immune thrombocytopenia (ITP) has an estimated global prevalence of 10 per 100,000 persons in the USA and mostly affects adults aged >55 years [1]. It is an immunological phenomenon in which antibodies target platelet surface proteins, such as GP IIb/IIIa, Ib/IIa, and VI [2]. The formation of antibodies remains somewhat unclear, although current literature suggests molecular mimicry, somatic mutations, or defects in autoreactive B cell elimination as probable causes [3]. It is also sometimes associated with viral infections such as HIV, hepatitis C, cytomegalovirus, and varicella-zoster virus. Antibody binding to platelet surface proteins results in platelet sequestration within the spleen and destruction by splenic macrophages, as well as peripheral destruction via complement [3]. This leads to thrombocytopenia and may result clinically in recurrent, easily forming ecchymoses and petechiae. Other findings include mucosal bleeding such as gingival bleeds, epistaxis, menorrhagia, and occult gastrointestinal bleeding. Feared, severe complications include intracranial hemorrhage or severe gastrointestinal bleeds [4]. Other complications include frequent infections, such as candidiasis and various gram-positive and gram-negative bacteria, as ITP is primarily managed with immunosuppressive therapies, including corticosteroids, intravenous immunoglobulin (IVIG), rituximab, thrombopoietin receptor agonists (TPO-RAs), and, in severe cases, splenectomy [5]. This case report represents a unique case of a respiratory syncytial virus (RSV) infection associated with acute ITP. Furthermore, the patient interestingly remained refractory to many of the first-line management options for ITP, such as corticosteroids, IVIG, and rituximab.
Case presentation
A 57-year-old woman with no known past medical history presented to the ED with epistaxis of three days' duration, intermittent dyspnea, and a mild cough. She reported having episodes of epistaxis once a month for the past year, but these episodes were mild and self-resolving. She also reported easy bruising for the last few months. Of note, she had not sought medical care for several years. Her vital signs included a temperature of 99.3°F, a heart rate of 100 beats per minute, blood pressure of 127/67 mmHg, a respiratory rate of 16 breaths per minute, and an oxygen saturation level of 97% on room air. On physical examination, she had dried blood present in her left naris. Her initial lab work (Table 1) was remarkable for leukocytosis (WBC count: 20.01 K/μL with 82.1% neutrophils), severe microcytic anemia (hemoglobin: 2.5 g/dL, hematocrit: 10.9%, and mean cell volume: 67.3 fL), thrombocytopenia (platelets: 7 K/μL), elevated uric acid (8.2 mg/dL), elevated lactate dehydrogenase (566 U/L), and transaminitis (aspartate aminotransferase: 252 U/L and alanine aminotransferase: 222 U/L). CT scan of the chest, abdomen, and pelvis was remarkable for hepatomegaly (22.38 cm) (Figure 1). Iron studies demonstrated low iron levels (24 µg/dL), a normal total iron-binding capacity (334 µg/dL), a low percent saturation (7%), and a normal ferritin level (22 ng/mL). Her severely low hemoglobin and hematocrit levels prompted further workup to rule out hemolysis; her haptoglobin level was 86 mg/dL. To rule out paroxysmal nocturnal hemoglobinuria (PNH), phosphatidylinositol-linked antigen testing was performed, demonstrating normal immunophenotyping results with no PNH clone detected in RBCs, granulocytes, or monocytes. The peripheral smear showed severely microcytic and hypochromic RBCs, no schistocytes, a few atypical monocytes with no blasts or Auer rods, and 0-1 platelets per high-power field. Bone marrow biopsy and aspirate of the right iliac bone demonstrated a hypercellular marrow with erythroid predominant trilineage hematopoiesis with maturation, mild megakaryocytosis, and decreased iron compatible with a diagnosis of ITP (Figure 2). The myeloperoxidase staining was performed to help exclude myeloid neoplasms and rule out ITP mimickers such as acute myeloid leukemia and myelodysplastic syndrome, especially given the history of anemia, bruising, and epistaxis. Flow cytometry of the bone marrow aspirate showed no diagnostic abnormalities, and fluorescence in situ hybridization was normal. Furthermore, FLT3-ITD and FLT3-TKD mutations were both negative. BCR-ABL1 fusion transcripts (P210 and P190) were not detected.
CT scan of the chest, abdomen, and pelvis for hepatomegalyCoronal view of the chest, abdomen, and pelvis. Liver measuring 22.38 cm (green line)I, Inferior
Composite photomicrograph of bone marrow biopsy and aspirateA. Bone marrow biopsy with inset of bone marrow aspirate smear (showing hypercellular marrow with erythroid predominant trilineage hematopoiesis, maturation, and mild megakaryocytosis)B. CD34 stainC. CD71 stain for erythroid cellsD. Myeloperoxidase stain for erythroid cellsE. Factor VIII stain for megakaryocytes
The patient received six units of packed RBCs and three units of platelets. After transfusion, the hemoglobin increased to 7.9 g/dL; however, the platelet count remained critically low at 2 K/μL, indicating persistent thrombocytopenia. The patient initially received IVIG 1 g/kg for two days and dexamethasone 40 mg for four days to treat suspected ITP, given the lack of improvement with platelet transfusions. She also received iron sucrose for severe iron-deficiency anemia. Despite IVIG and steroids, she remained refractory with a platelet count of 2 K/μL. She then received Promacta 50 mg once daily, but her platelet count did not improve after four days of treatment. Patient was subsequently switched to Nplate 1 mcg/kg weekly. Her platelet count remained at 1 K/μL, so rituximab was started. Of note, the patient was also experiencing a cough for three days and a mild headache that resolved with over-the-counter acetaminophen approximately 1.5 weeks after her initial presentation. A respiratory panel using polymerase chain reaction to detect influenza A, influenza B, SARS-CoV-2, and RSV was performed. The patient tested positive for RSV, which was thought to potentially contribute to her refractory ITP. She developed lower extremity petechiae and mild, bright red blood per rectum, so she was started on Amicar. Her bloody stool likely was due to a lower tract gastrointestinal bleed, given her severely low platelet count, along with the absence of anal fissures or external hemorrhoids on physical examination. Her platelet count remained between 1 K/μL and 6 K/μL, so her Nplate dose was increased to 3 mcg/kg weekly, and prednisone 1 mg/kg daily was added. Her platelet count remained at 3 K/μL, so she was started on cyclosporine 150 mg twice daily. After four days of cyclosporine, her platelet count steadily increased to 22 K/μL, and she was discharged. She was then continued on 150 mg of cyclosporine twice a day after discharge. A repeat platelet count approximately one month after discharge was 30.6 K/μL.
Discussion
This case highlights a rare and clinically significant instance of severe, refractory ITP in an otherwise healthy adult, likely triggered or exacerbated by acute RSV infection. Although RSV has previously been associated with thrombocytopenia in pediatric patients, the role of ITP as a potential mechanism has not been described in either the pediatric or adult population [6]. Thus, this report expands the clinical spectrum of RSV infection in being a potential immune trigger for severe autoimmune thrombocytopenias, even in immunocompetent adults.
Thrombocytopenia in adults is commonly implicated in hematologic malignancies. However, a previous case described a 28-year-old male patient with a history of acute lymphoblastic leukemia (ALL)-induced thrombocytopenia successfully treated with a double umbilical cord blood transplant. Subsequent cytogenetic analysis revealed a normal karyotype and resolution of thrombocytopenia. However, he presented 19 months later with a new onset of severe thrombocytopenia in the setting of confirmed active RSV infection. Prompt bone marrow evaluation was performed, given the history of ALL, and a new cytogenetic abnormality was detected, involving a translocation between chromosomes 1 and 14. Seven months later, repeat cytogenetic analysis and hematologic workup revealed no apparent chromosomal abnormalities and resolution of thrombocytopenia [7]. Thus, this rare case may suggest a potential etiology of RSV-related thrombocytopenia, although the exact relationship between RSV and autoimmune thrombocytopenia remains unclear.
The patient presented with profound thrombocytopenia, microcytic anemia, and mucocutaneous bleeding. Proposed mechanisms of virus-induced ITP include molecular mimicry, immune complex deposition, and impaired immune tolerance [8]. Despite early administration of standard therapies such as IVIG, corticosteroids, rituximab, and TPO-RAs, this patient remained refractory. Only after initiating cyclosporine, an immunosuppressant not routinely used in early ITP management, did platelet counts begin to improve from three to 22 over the course of four days. While most ITP cases respond to these standard therapies, this patient’s eventual improvement with cyclosporine suggests an alternative pathway of immune dysregulation, potentially amplified by RSV-mediated activation of autoreactive lymphocytes [8]. Refractoriness to multiple lines of therapy further emphasizes the complexity of this immune response.
Of note, our patient also demonstrated acute, severe microcytic anemia, with a hemoglobin count of 2.5 g/dL, a hematocrit of 10.9%, and a mean cell volume of 67.3 fL. Her anemic presentation was improved drastically with six units of packed RBCs. The most common etiology of microcytic anemia is iron deficiency with either blood loss (e.g., gastrointestinal bleeds), dietary lack, or defective iron-absorptive capacities [9]. Other potential causes include inherited thalassemias and anemia of chronic illness. There is currently an unclear relationship between RSV and microcytic anemias. Although certain viral infections may trigger aplastic anemia, as with the case of human parvovirus B19, the relationship between RSV and microcytic anemia remains to be further elucidated [10]. As mentioned previously, a proposed mechanism for thrombocytopenia in the setting of viral illness is molecular mimicry, in which viral antigens may share common epitopes with platelet antigens, leading to their destruction via cross-reacting antibody generation [8]. However, this study did not specifically research RSV. Another study suggested that platelets are specifically used in the clearance of RSV infection via reduced monocyte infection and activation [11]. They also found RSV viral particles within platelets, suggesting the internalization of RSV by platelets. They concluded that thrombocytopenia can predispose patients to worsened RSV infections; however, they did not note resultant thrombocytopenia as a result of RSV infection. Thus, although our case report is consistent with the limited available literature demonstrating a correlation between thrombocytopenia and RSV, further research is needed to infer causality and elucidate the mechanism behind thrombocytopenia.
This single case limits generalizability, and further investigation is needed to elucidate RSV’s role in ITP pathogenesis. Larger systematic studies on virus-associated ITP may help identify risk factors and inform more targeted treatment approaches, including the consideration of alternative agents such as cyclosporine in refractory cases. Clinicians should consider viral triggers, including RSV, in cases of new onset or worsening acute ITP, particularly those unresponsive to standard therapies. In such refractory cases, cyclosporine may serve as a viable salvage therapy.
Conclusions
This case report represents an unusual, severe exacerbation of ITP potentially due to an underlying RSV infection. RSV infections are typically mild in healthy adults with no concurrent comorbidities such as diabetes, chronic obstructive pulmonary disease, or an immunocompromised state. Severe RSV complications seldom occur, and there are few reports of severe ITP exacerbations associated with underlying RSV infections. ITP may be asymptomatic in nature but can present with skin and mucosal petechiae and bruising, occult gastrointestinal bleeds, and, in severe cases, may lead to intracranial hemorrhage. Thus, severe ITP, especially cases that are refractory to first-line treatments such as corticosteroids and IVIG, must be carefully managed to achieve optimal patient outcomes. Furthermore, a better understanding of the relationship between RSV infection and ITP is critical, as RSV is a common infection globally.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Immune thrombocytopenic purpura: epidemiology and implications for patients Eur J Haematol Suppl Michel M 3720091920030110.1111/j.1600-0609.2008.01206.x · doi ↗ · pubmed ↗
- 2Immune thrombocytopenia Pietras NM Gupta N Justiz Vaillant AA Pearson-Shaver AL Treasure Island, FL Stat Pearls [Internet], Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 562282/32965953 · pubmed ↗
- 3Pathogenesis of immune thrombocytopenia Autoimmun Rev Audia S Mahévas M Samson M Godeau B Bonnotte B 6206321620172842812010.1016/j.autrev.2017.04.012 · doi ↗ · pubmed ↗
- 4Bleeding complications in immune thrombocytopenia Hematology Am Soc Hematol Educ Program Arnold DM 237242201520152663772810.1182/asheducation-2015.1.237 · doi ↗ · pubmed ↗
- 5Recent advances in the management of immune thrombocytopenic purpura (ITP): a comprehensive review Medicine (Baltimore) Madkhali MA 0103202410.1097/MD.0000000000036936 PMC 1079871238241567 · doi ↗ · pubmed ↗
- 6Hematologic complication of respiratory virus infection Korean J Pediatr Infect Dis Park IH Lee SH You ST Choi DY 178202013
- 7RSV-related thrombocytopenia associated with transient cytogenetic abnormalities in a recipient of umbilical cord blood transplantation Case Rep Hematol Pokhrel SD Persons DL Aljitawi OS 8628507201620162694955310.1155/2016/8628507 PMC 4754480 · doi ↗ · pubmed ↗
- 8Virus-associated idiopathic thrombocytopenic purpura Transfus Sci Rand Ph DML Fraser Wright Ph DJ 2532591919981035113710.1016/s 0955-3886(98)00039-3 · doi ↗ · pubmed ↗