The Effect of Adhesive Systems on the Bond Strength of Directly Bonded Fixed Partial Dentures Using Artificial Teeth: An In Vitro Study
Adityakrisna Yoshi Putra Wigianto, Yuichi Ishida, Megumi Watanabe, Tetsuo Ichikawa

TL;DR
This study compared two adhesives for bonding artificial teeth and found one provided significantly stronger and more reliable bonds.
Contribution
The study introduces a direct comparison of self-curing and light-curing adhesives for bonding artificial teeth in fixed dentures.
Findings
Self-curing resin cement showed significantly higher shear bond strength than light-curing flowable resin composite.
Self-curing resin cement exhibited no adhesive failure, while light-curing composite primarily failed adhesively.
The presence of a retentive groove had no significant effect on bond strength with self-curing resin cement.
Abstract
Objective This study aimed to evaluate the effect of different adhesive systems on the bond strength of a directly bonded fixed partial denture (DBFPD) utilizing artificial teeth through shear bond strength (SBS) testing and a DBFPD model experiment. Materials and methods Two different adhesive systems: self-curing resin cement (SRC) (Super Bond Universal; Sun Medical, Moriyama, Japan) and light-curing flowable resin composite (LFRC) (G-Fix; GC, Tokyo, Japan) were applied to two different hybrid resin artificial teeth: Duracross Physio (Nissin, Kyoto, Japan) and Endura Posterio (Shofu, Kyoto, Japan). The SBS of the adhesive systems to artificial teeth was evaluated using a universal testing machine (AGX-1kN, Shimadzu, Kyoto, Japan). Subsequently, the failure modes were assessed using a stereomicroscope (VHX-970F, Keyence, Osaka, Japan). An experimental model comprising a lower…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
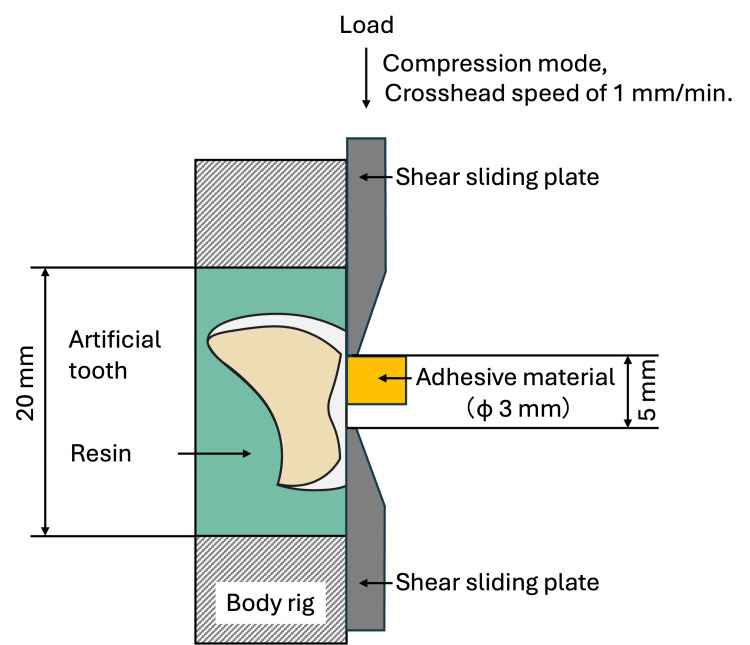 Figure 1
Figure 1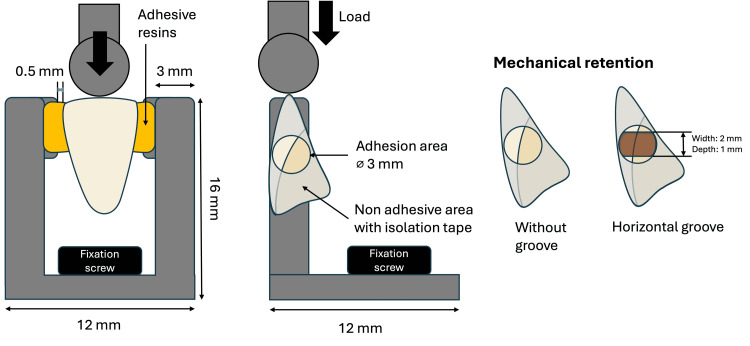 Figure 2
Figure 2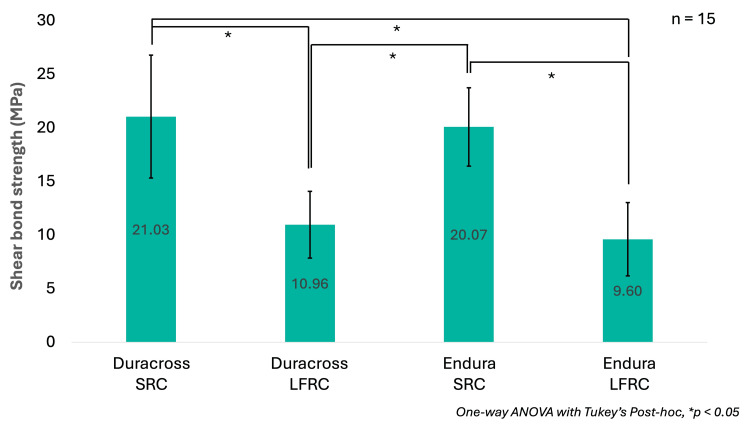 Figure 3
Figure 3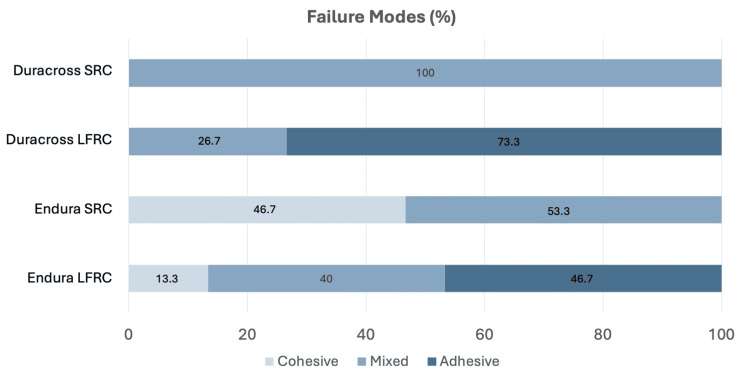 Figure 4
Figure 4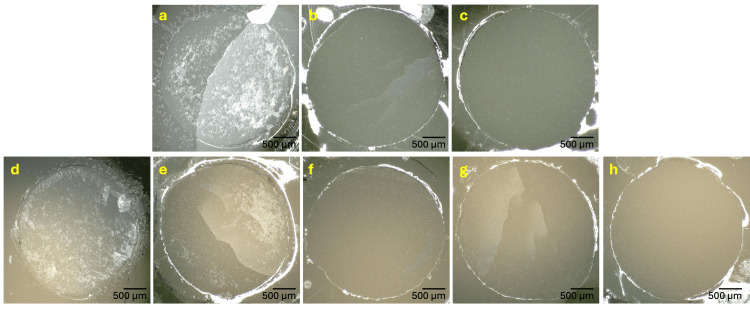 Figure 5
Figure 5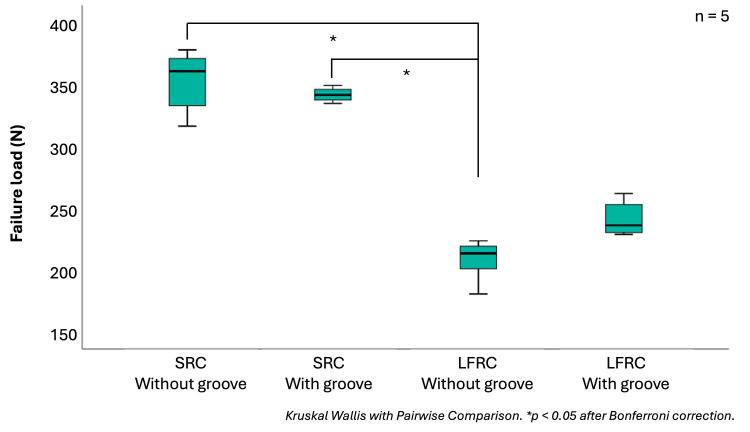 Figure 6
Figure 6| Material type | Identification | Composition | Manufacturer | |
| Artificial tooth | Duracross | Composite resin (68% filler content) | Nissin Dental Products, Kyoto, Japan | |
| Endura | Composite resin (47% filler content) | Shofu, Kyoto, Japan | ||
| Surface treatment | M&C Primer | Primer A: MMA, MDP, VBATDT, Acetone Primer B: MMA, γ-MPTS | Sun Medical, Moriyama, Japan | |
| GC Ceramic Primer-II | γ-MPTS (γ-methacryloxypropyl trimethoxysilane), 10-MDP (10-methacryloyloxydecyl dihydrogen phosphate), MDTP (methacryloyloxydecyl dihydrogen thiophosphate), BisGMA (bisphenol A-glycidyl methacrylate), TEGDMA (triethylene glycol dimethacrylate), ethanol | GC, Tokyo, Japan | ||
| Fixation material | Self-cure resin cement (SRC): Super Bond Universal | Quick monomer: methyl methacrylate (MMA), 4-methacryloxyethyl trimellitate anhydride (4-META). Catalyst V: tri-n-butylborane (TBB). Powder: polymethyl methacrylate (PMMA) | Sun Medical, Moriyama, Japan | |
| Light-cure flowable resin composite (LFRC): G-Fix | Resin paste: barium glass silane-treated filler (26%), methacrylate ester, phosphate ester monomers, photoinitiator | GC, Tokyo, Japan | ||
| Material | Application procedure | |||
| M&C Primer | Dispense equal drops of primer A and primer B into a disposable mixing well, mix with a microbrush, then apply to a clean adhesion surface | |||
| Super Bond Universal (Brush-dip technique) | Prepare a polymer powder in the dispensing dish, flatten the surface, and prepare the activated liquid by mixing an appropriate amount of quick monomers and catalyst V with a 4:1 drops ratio. Afterward, wet a brush tip with the activated liquid, then touch the polymer powder with the brush tip, forming a small polymer ball. Finally, transfer and apply the polymer balls onto the isolated bonding surface adequately | |||
| GC Ceramic Primer-II | Dispense one drop of ceramic primer II into a dispensing dish, then apply as a thin layer to a clean adhesion surface using a microbrush | |||
| G-Fix | Dispense the flowable resin paste onto the adhesion surface. Light cure for 10 seconds | |||
| Groups | Mean ± SD (N) | Median | Lower quartile | Upper quartile |
| SRC without groove | 345 ± 26a | 354 | 338 | 367 |
| SRC with groove | 342 ± 16a | 336 | 331 | 346 |
| LFRC without groove | 203 ± 17b | 209 | 187 | 217 |
| LFRC with groove | 237 ± 14ab | 232 | 225 | 252 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental materials and restorations · Dental Implant Techniques and Outcomes · Orthodontics and Dentofacial Orthopedics
Introduction
The resin-bonded fixed partial denture (RBFPD) has been widely used in prosthodontic treatment thanks to the sustained development of adhesive materials. In contrast to the conventional fixed partial denture (CFPD), which requires extensive abutment tooth preparation, RBFPD can be fixed with minimal enamel reduction or even without any reduction. Consequently, it is advantageous, especially in preserving the integrity of adjacent tooth surfaces. Reported survival rates range from 84.8 to 95.01% after five years, depending on the materials and number of retainers [1].
Although the RBFPD is more cost-effective than CFPDs or fixed implant prostheses, this indirect technique still requires laboratory work to manufacture using materials such as ceramics, metals, or fiber-reinforced composite [2]. As an alternative, a directly bonded fixed partial denture (DBFPD) technique has been introduced, offering a simplified procedure that can be completed entirely chairside without the need for impressions or additional laboratory steps [3]. Initially, this method was used as a temporary prosthodontic method, where an artificial tooth or extracted natural tooth was bonded to the pontic portion with an adhesive material. Consequently, the DBFPD is particularly beneficial for cases requiring same-day treatment or for dentists working in settings with limited facilities, such as rural areas without access to dental laboratories or in countries where health insurance does not cover fixed dental prostheses (FDPs).
Clinical studies on the use of DBFPD are limited. Previously reported pontic options include an extracted natural tooth [4], a composite resin artificial tooth [5], or an acrylic resin artificial tooth [6]. Methyl methacrylate-based resin and composite resin luting agents have been used to fix DBFPD to adjacent teeth [3]. The success of DBFPD treatment is dependent on several key factors, including the appropriate selection of pontic material, the surface properties of the bonding areas, the choice of adhesive, and the bonding procedure itself. However, in vitro studies evaluating the bond strength of artificial teeth primarily focus on analyzing their adhesion to the denture base [7].
The 4-methacryloyloxylethyl trimellitate anhydride (4-META)/methyl methacrylate (MMA)-tri-n-butyl borane (TBB) resin luting agent has been frequently used for distal base-free posterior fixed dental prostheses (DBFPD) and the splinting of mobile teeth, demonstrating satisfactory bond strength and clinical outcomes. Recently, a Bis-EMA and phosphoric ester monomer-based flowable resin paste has been evaluated in a study as a potential resin-based material for posterior FDPs [8]. Although clinical applications of DBFPDs using artificial teeth have been reported in a few studies [5,6,9], the optimal conditions for bonding artificial teeth to adjacent natural teeth remain unclear. Factors such as artificial tooth type and composition, surface treatment, and adhesive material selection require further investigation.
Previous research has explored the use of both 4-META/MMA-TBB resin and Bis-EMA-based resin in adhesive dentistry. However, a systematic literature search conducted to identify previous studies comparing the bond strength of these two adhesive materials for DBFPDs with artificial teeth returned no relevant results. Therefore, this study aimed to evaluate the bond strength and failure modes of two adhesive systems applied to different artificial teeth compositions and the presence of a retentive groove to determine an effective adhesive system for DBFPD.
Materials and methods
Materials
Two types of hybrid composite resin artificial teeth were used in this study: Duracross Physio (Nissin Dental Products; Kyoto, Japan) and Endura (Shofu, Kyoto, Japan). Two different adhesive resin systems were utilized: a self-cure resin cement, Super Bond Universal (Sun Medical, Moriyama, Japan), and a light-cure flowable resin composite, G-Fix (GC, Tokyo, Japan), hereinafter abbreviated as SRC and LFRC, respectively. The chemical surface treatments applied were M&C Primer (Sun Medical, Moriyama, Japan) and GC Ceramic Primer II (GC; Tokyo, Japan). The detailed compositions of these materials are provided in Table 1, while the specific application procedures, based on the manufacturers' instructions, are outlined in Table 2.
Shear bond strength (SBS)
The SBS of the artificial tooth enamel equivalent and the adhesive material was evaluated. The in vitro experiment setting is shown in Figure 1. The substrate in this study was prepared by initially flattening the artificial teeth surface with a carborundum bur (Shofu; Kyoto, Japan) using a micromotor, then embedding it in a specimen embedding resin - Technovit 4071 (Kulzer, Hanau, Germany) - by using a cylindrical mold that fits the size of the shear bond strength (SBS) testing jig. Subsequently, the embedded artificial tooth underwent polishing with a #600-grit silicon carbide paper using a specimen preparation polishing machine to ensure a flush surface.
Illustration of shear bond strength evaluation test performed in this study
Before the adhesion procedures, the surfaces of embedded artificial teeth were sandblasted with 50 μm aluminium oxide at 2 MPa, cleaned in an ultrasonic cleaner with ethanol, and thoroughly dried. Afterwards, the adhesion area was isolated into a 3 mm diameter using a tape with a 3 mm punched hole. The chemical surface treatments were then applied as per the manufacturer’s instructions on the isolated area. A mold was then placed on the isolated surface, and then the adhesive materials were prepared and applied onto the substrate inside the mold. The SRC was applied by applying resin balls made from picking the polymer using a brush dipped in their activated liquid, then chemically polymerized after six minutes. On the other hand, the LFRC system was applied by dispensing the resin in the form of a flowable resin paste continuously, then polymerized using a visible blue LED light with 2000 mW/cm^2^ at 460 nm wavelength Pencure 2000 (Morita, Kyoto, Japan) for 10 seconds. Subsequently, the samples were stored in distilled water for 24 hours at 37 °C.
The SBS tests were performed using an SBS testing jig installed on a universal testing machine AGX-1kN (Shimadzu, Kyoto, Japan) with a crosshead speed of 1 mm/min. The surface of debonded samples following the SBS test was evaluated using a digital stereomicroscope (VHX-970F, Keyence, Osaka, Japan) to assess the failure types into the following three categories: adhesive: fracture occurred at the interface between the adhesive material and the artificial tooth; cohesive: occurred within the artificial tooth without any adhesive material failure; and mixed: occurred on both artificial tooth and adhesive material. Fifteen specimens were prepared in each condition.
Model experiment
The model experiment samples were prepared using lower incisor Duracross Physio as a pontic in two groups, based on the adhesive materials (SRC and LFRC). Each group was further subdivided into two based on the presence and absence of a retentive groove (a 2 mm-wide, 1 mm-deep horizontal groove was made on the proximal surface using a ⌀2 mm carbide bur) (Figure 2). In total, there were four groups evaluated (SRC without groove; SRC with groove; LFRC without groove; LFRC with groove). Subsequently, the proximal surfaces were sandblasted, cleaned with ethanol using an ultrasonic machine, and then isolated using tape as described in the SBS test to control the adhesion area. Custom metal jigs made of cobalt chromium were fabricated, referring to a method reported by Nakajima et al. [10].
Illustration of the model experiment configurations performed in this study and the artificial tooth mechanical retention structure explanation
To ensure an identical position of the pontic toward the metal jig, a silicone rubber, Labocone putty (GC; Tokyo, Japan) was utilized as the pontic holder in all samples during the adhesive procedures until complete polymerization. Afterwards, the adhesive materials were applied to adhere the pontic to the jig as per the manufacturer's instructions. Following 24-hour immersion in distilled water, the samples were fixed onto the universal testing machine by using a bolt screw, then an axial load was applied to the center of the incisal surface using a compression mode with a crosshead speed of 1 mm/min (Figure 2). The maximum load required to detach the artificial tooth from the model was recorded as a failure load in Newton (N), along with the failure locations: metal-jig or artificial tooth side. Five specimens were prepared in each condition.
Statistical analysis
The Shapiro-Wilk test was conducted to verify the normality of the collected datasets, and then parametric statistical analysis was carried out. One-way analysis of variance (ANOVA) with Tukey’s post-hoc was performed to investigate the significant differences between groups in SBS evaluation. The Kruskal-Wallis test was conducted with pairwise comparisons to investigate the significant differences between groups in model bond strength evaluations. Afterwards, a Bonferroni correction was performed to adjust the p-values. The significance level was set at 0.05, and the statistical analysis software IBM SPSS Statistics version 25 (IBM Corp., Armonk, NY) was utilized.
Results
SBS results
Figure 3 shows the means and standard deviations (SD) of SBS in each condition. The highest SBS was found on the Duracross SRC group (21.03 ± 5.73 MPa), followed by Endura SRC (20.07 ± 3.65 MPa), Duracross LFRC (10.96 ± 3.11 MPa), and Endura LFRC (9.6 ± 3.42 MPa), respectively. The One-way ANOVA result on SBS evaluation revealed that there was a statistically significant difference in SBS between groups (p = 0.000). Based on Tukey’s post-hoc results, the significant SBS differences were only evident between the different adhesive materials (p = 0.000), whereas no significance was observed based on different artificial teeth (p = 0.967 within Duracross SRC and Endura SRC; p = 0.841 within Duracross LFRC and Endura LFRC).
Shear bond strength comparison between different artificial tooth and fixation materialsNumbers inside the bars represent the mean, while the T-bars indicate the standard deviationSRC: self-curing resin cement; LFRC: light-curing flowable resin composite
Failure modes
The failure mode distributions from all groups after SBS evaluation are provided in Figure 4, with representative stereomicroscopic images provided in Figure 5. When fixing an artificial tooth with SRC, no adhesive failure was observed. In the Duracross SC group, mixed failures were observed in all samples (100%), whereas 53.3% mixed failures and 46.5% cohesive failures on SRC were seen on the Endura artificial tooth. In contrast, adhesive failures were observed in the LFRC groups. The adhesive failure of LFRC-fixed Duracross was 73.3%, followed by 26.7% of mixed failures. Similarly, failure modes of LFRC-fixed Endura were dominantly adhesive (46.7%), followed by mixed (40%), and cohesive on LFRC (13.3%), respectively.
Failure mode distribution percentage in all groups following shear bond strength evaluationSRC: self-curing resin cement; LFRC: light-curing flowable resin composite
Representative stereomicroscopic images at 50× magnification of each failure modesUpper panel (Duracross): a. SRC mixed, b. LFRC mixed, and c. LFRC adhesive. Lower panel (Endura): d. SRC cohesive, e. SRC mixed, f. LFRC cohesive, g. LFRC mixed, and h. LFRC adhesiveSRC: self-curing resin cement; LFRC: light-curing flowable resin composite
Model experiment
Figure 6 shows the box plots of the model experiment results, and the descriptive data are provided in Table 3. SRC-fixed artificial tooth without groove demonstrated the highest bond strength (345 ± 26 N), followed by SRC with groove (342 ± 16 N), LFRC with groove (237 ± 14 N), and LFRC without groove (204 ± 17 N). Similar to the SBS results, the bond strengths of SRC without and with groove were significantly higher than those of the LFRC without groove (p = 0.005, p = 0.006, respectively). The presence of a groove in the LFRC group resulted in a slightly higher bond strength, but it was not statistically significant (p = 1.000). Moreover, the bond strength of the LFRC with groove also did not significantly differ from either SRC without groove (p = 0.253) or SRC with groove (p = 0.288). Regarding failure locations, all LFRC without groove models failed on the artificial tooth surface, whereas LFRC with groove demonstrated 60% tooth and 40% metal side. The SRC without a groove failed more likely in the metal side (60%) than the tooth side (40%), whereas the groove presence demonstrated more tooth side failure (80%) than metal (20%).
Box plots of failure loads measured in the model experiment representing median, upper quartile, lower quartile, maximum, and minimum value of each datasetSRC: self-curing resin cement; LFRC: light-curing flowable resin composite
Table 3: Model experiment resultsDifferent superscript characters (a, b, ab) indicate a statistically significant difference between groups (p<0.05). Groups sharing a common superscript letter (e.g., a and ab) are not significantly different from each otherSD: standard deviation; SRC: self-curing resin cement; LFRC: light-curing flowable resin composite
Discussion
In recent years, treatment methods that minimize invasiveness and are completed chairside as much as possible have been promoted. There are various options in providing fixed partial dentures directly, such as fiber-reinforced [11], metal wire-reinforced composites in which the pontics are built manually [12], injecting flowable composite into a custom mold technique [13], and utilizing an artificial tooth as a pontic in DBFPD. DBFPD utilizing artificial tooth provides several advantages, such as minimum effort, unlike manually sculpting pontic morphology, which relies on individual skills, thus saving time and number of visits. DBFPD is considered a simple method that makes it easier to ensure both aesthetic and functional qualities. Artificial teeth are also very stable in terms of materials science.
The DBFPD technique is indicated for cases where the pontic space between abutment teeth is narrow, such as in a mandibular anterior tooth. However, in cases like when highly characterized morphologies or tooth shades are desired and large interproximal spaces exist, this method may not address those demands appropriately, as the shape and shades of the artificial teeth are prefabricated. Although factors such as occlusal equilibration, patient cooperation, and adequate posterior occlusal support should be carefully considered [3], particular attention must also be given to the bond strength and the condition at the fixation sites, as these are critical aspects that warrant thorough investigation. The two adhesive materials used in this study have been previously reported to bond with natural teeth favorably. The SBS of SRC to enamel with prior surface acid-etching was reported to be around 30 MPa [14,15], whereas the LFRC was reported at 24 MPa [16]. Both materials are considered potential for DBFPD with artificial tooth owing to their simple application procedures, but differ in application and polymerization method. On the other hand, there have not been enough reports on their adhesion to artificial teeth.
The present study suggested that the SBS of both adhesives to artificial teeth evaluated in this study was lower than their reported SBS to enamel. Therefore, DBFPD with artificial teeth utilizing these adhesives would be more likely to fail on the hybrid-resin artificial tooth side than the abutment side, which is clinically desirable as it leaves the abutment tooth undamaged [17]. Currently, there is no consensus on a clinically acceptable SBS range for FPDs. Previous studies reported a wide range of SBS as it varies with adhesive materials and procedures, substrates, and adherends evaluated. For example, the SBS of various ceramic RBFPDs to enamel ranges from 6 to 31 MPa [18]. Another study reported the SBS of fiber-reinforced composite resin FPDs within 12-21 MPa [19]. The SBS values of 10-20 MPa indicated in this study are speculated to be a clinically acceptable range.
The higher SBS of SRC groups than that of LFRC groups corroborates previous studies, reporting that MMA-based resin cements exhibited stronger bond strength than composite resins due to their ability to penetrate polymer chain interspaces, forming a semi-interpenetrating polymer network [20]. The SRC used in this study is a self-curing resin initiated by TBB, resulting in a long polymerization time, allowing longer infiltration on the artificial tooth surface [21]. In contrast, LFRC relies on a photo/light-initiated polymerization process, increasing the risk of polymerization shrinkage stress on the adhesive interface, reducing the bond strength [22]. Moreover, G-Fix has higher flexural strength (239 MPa) and modulus of elasticity (25 GPa) than Super Bond (159 MPa; 16 GPa, respectively) [23,24]. These mechanical properties have been reported to affect SBS [25], which may explain the findings of this study. As addressed by Tanoue et al. [3], despite its lower mechanical properties, plastic deformations in MMA-based resins may be advantageous in DBFPD applications. Within the same adhesive system applied to different artificial teeth, there was no significant difference in the SBS. This result might indicate that the filler content difference between Duracross Physio (68%) and Endura Posterio (47%)’s outermost hybrid resin layer does not affect SBS, which aligns with the study by Han et al. (2020) [26].
Further investigation on the failure mode revealed that no adhesive failure was observed in the SRC groups, whereas most of the LFRC groups failed adhesively. Adhesive failures observed in LFRC groups may be attributed to weak bonding at the adhesion interface. Despite no SBS difference, the failure mode characteristics differed between Duracross and Endura. When adhered with SRC, mixed failure was evident on all debonded Duracross samples, whereas both mixed and cohesive failure of SRC were observed on Endura. Similarly, Han et al. (2020) also reported more cohesive failures of resin cement in Endura, without a significant difference in SBS [26]. The lower filler percentage of Endura might allow for greater penetration of adhesive resins into the matrix, resulting in these findings.
The bond strength of the DBFPD was examined in a more clinically relevant model experiment. The model experiment results (204-345 N) suggest that the adhesive systems tested in this study exhibited potential load resistance that exceeds the average reported functional forces loaded to the anterior region (108 to 185 N) [27,28]. It is also comparable to previous anterior RBFPD reports, which vary widely from 210 to 724 N [29,30], which mostly employed solid connector structures, whereas the connector in this study was merely adhesive resins. Although not statistically significant, the presence of a horizontal groove slightly reduced the bond strength in SRC, whereas it increased the bond strength in the LFRC group. Therefore, the presence of an additional retentive groove on an artificial tooth may be beneficial when fabricating DBFPDs using composite resin, but not with the MMA-based resin cements.
Similarly, a study by Nakajima et al. reported that the presence of holes, grooves, rest, and pins did not significantly affect the bond strength of 4-META/MMA-TBB compared to a silane-treated artificial tooth without mechanical reinforcement [10]. Clinicians should meticulously consider material selection to achieve successful treatment. Composite materials with higher mechanical properties may be more suitable when utilized as the main component of composite FPDs, as it was reported to perform well in an in vitro evaluation for a fiber-reinforced molar inlay retained FPD [8]. Based on the results from this in-vitro study, the characteristics of MMA-based resins appear more effective for achieving bond integrity on hard resin artificial teeth, as they provided consistently higher bond strength values and more favorable failure modes than the LFRC.
There are some limitations in this in vitro study that need to be considered when interpreting the results. As an in vitro investigation, this study is inherently limited by the challenges of fully simulating the dynamic and complex oral environment. The bond strength and failure load were measured after 24-hour immersion in distilled water, only representing a short-term condition without the durability aspects simulating more extensive clinical conditions, such as cyclic loading and thermal cycling. In the model experiment, a metal jig was utilized as abutment teeth instead of natural extracted incisors to minimize uncontrollable anatomical variations of extracted natural teeth; thus, the estimated failure load values might differ when bonded to enamel clinically. The scope of this study was limited by the small number of specific adhesive systems and artificial tooth compositions tested, which may restrict the broad generalizability of our findings. Further in vitro and rigorous clinical studies on DBFPD utilizing artificial teeth should be conducted to clarify these aspects.
Conclusions
The present in vitro study highlights the impact of the adhesive material selection on DBFPD using an artificial tooth as a pontic. The 4-META/MMA-TBB self-curing resin cement demonstrated better bond strength to hybrid resin artificial teeth than the light-curing flowable resin composite for tooth splinting material. This better performance was observed under static laboratory testing conditions, irrespective of the differences in artificial tooth filler percentages or the presence of a retentive groove. These results should be interpreted with caution when extrapolating to long-term clinical outcomes, which are subject to factors such as dynamic fatigue, thermal changes, and material degradation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Five-year success rate of resin-bonded fixed partial dentures: a systematic review J Esthet Restor Dent Alraheam IA Ngoc CN Wiesen CA Donovan TE 40503120193030290910.1111/jerd.12431 · doi ↗ · pubmed ↗
- 2Survival rates of anterior-region resin-bonded fixed dental prostheses: an integrative review Eur J Dent Mendes JM Bentata AL de SáJ Silva AS 7887971520213442885010.1055/s-0041-1731587 PMC 8630935 · doi ↗ · pubmed ↗
- 3Direct bonded fixed partial denture with an artificial denture tooth as a pontic Jpn Dent Sci Rev Tanoue N Takeuchi Y Furuchi M Yamamori T Ohkawa S 1541575720213453994010.1016/j.jdsr.2021.08.003PMC 8441073 · doi ↗ · pubmed ↗
- 4Eleven-year clinical performance of a mandibular natural tooth pontic bonded with modified tri-n-butylborane initiated adhesive resin J Oral Sci Nakamura M Nogawa H Matsumura H 3853885720152666686410.2334/josnusd.57.385 · doi ↗ · pubmed ↗
- 5A direct bonded fixed partial dental prosthesis: a clinical report J Prosthet Dent Tanoue N Tanaka T 81111320152527703310.1016/j.prosdent.2014.07.014 · doi ↗ · pubmed ↗
- 6A two-stage resin-bonded fixed partial denture seated in conjunction with postextraction healing of the alveolar socket: a clinical report J Prosthet Dent Monya Y Matsumura H Atsuta M 48801998965617010.1016/s 0022-3913(98)70083-6 · doi ↗ · pubmed ↗
- 7The shear bond strength between milled denture base materials and artificial teeth: a systematic review Dent J (Basel) Prpic V Catic A Kraljevic Simunkovic S Bergman L Cimic S 23251120233697556410.3390/dj 11030066 PMC 10046986 · doi ↗ · pubmed ↗
- 8Load-bearing capacity of novel resin-based fixed dental prosthesis materials Dent Mater J Cekic-Nagas I Egilmez F Ergun G Vallittu PK Lassila LV 49583720182908144510.4012/dmj.2016-367 · doi ↗ · pubmed ↗