Robot-Assisted Laparoscopic Radical Prostatectomy in a Patient With Ectopic Ureter
Junji Yatsuda, Hideaki Nishizawa, Toshiki Anami, Kurahashi Ryoma, Murakami Yoji, Tomomi Kamba

TL;DR
A rare case of robot-assisted prostate surgery in a patient with an ectopic ureter is reported, highlighting the importance of preoperative diagnosis to avoid complications.
Contribution
This case report highlights the challenges and outcomes of robot-assisted prostatectomy in a patient with an ectopic ureter.
Findings
Preoperative diagnosis of ectopic ureter is crucial to avoid surgical complications.
The patient developed biochemical recurrence after surgery and required additional treatments.
Unexpected urinary structures or leakage may indicate an ectopic ureter.
Abstract
An ectopic ureter is a rare male anomaly. We report a case of robot-assisted radical prostatectomy for prostate cancer in a patient with an ectopic ureter and a duplicated collecting system. A 71-year-old man was diagnosed with prostate cancer. Preoperative evaluation identified a left ectopic ureter opening into the bladder neck. During robot-assisted radical prostatectomy, an attempt to preserve the ectopic orifice resulted in an extensive positive surgical margin. The patient subsequently developed biochemical recurrence and was treated with androgen deprivation therapy and salvage radiotherapy. His prostate-specific antigen level is now undetectable. Preoperative diagnosis of an ectopic ureter is crucial for surgical planning to avoid positive margins and complications. This anomaly should be considered if an unexpected tubular structure is encountered intraoperatively or if…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
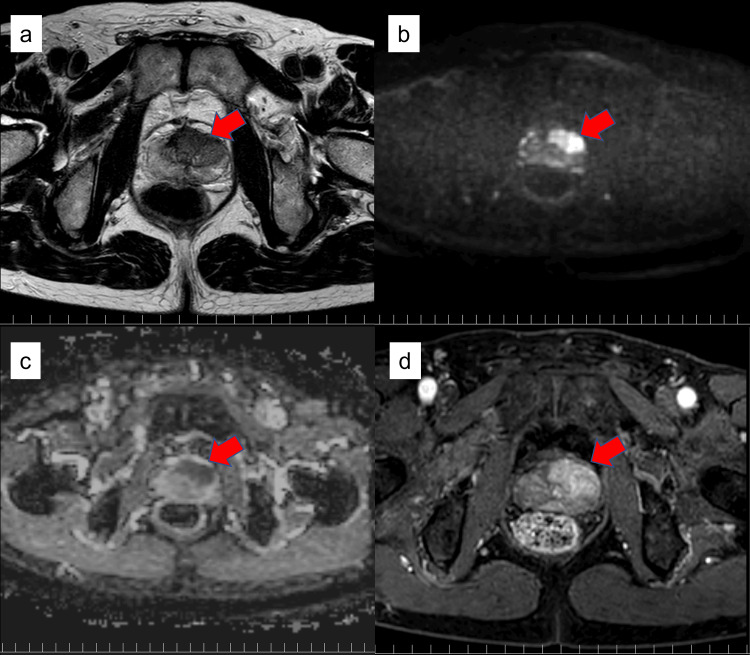 Figure 1
Figure 1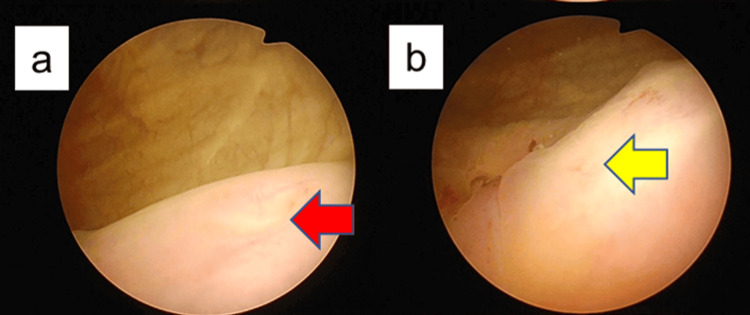 Figure 2
Figure 2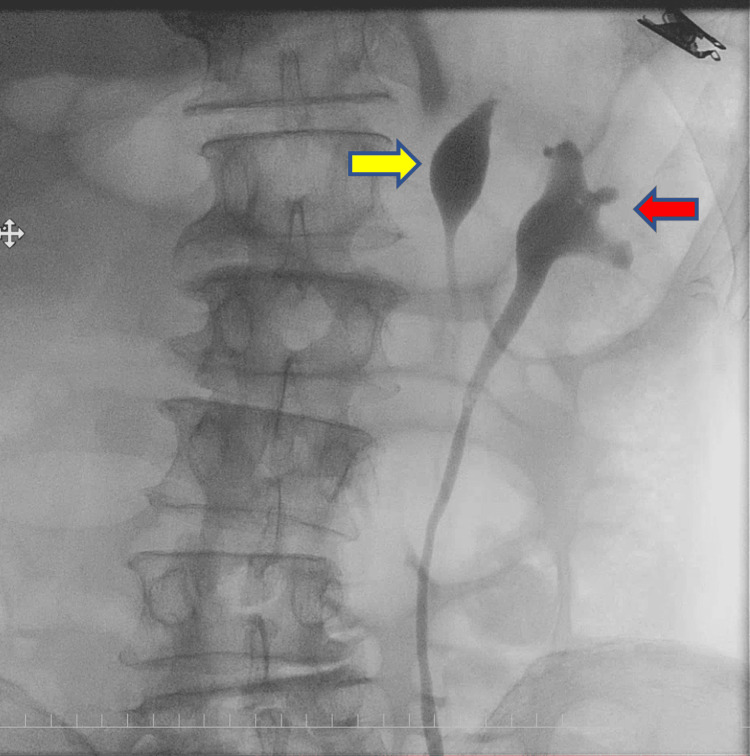 Figure 3
Figure 3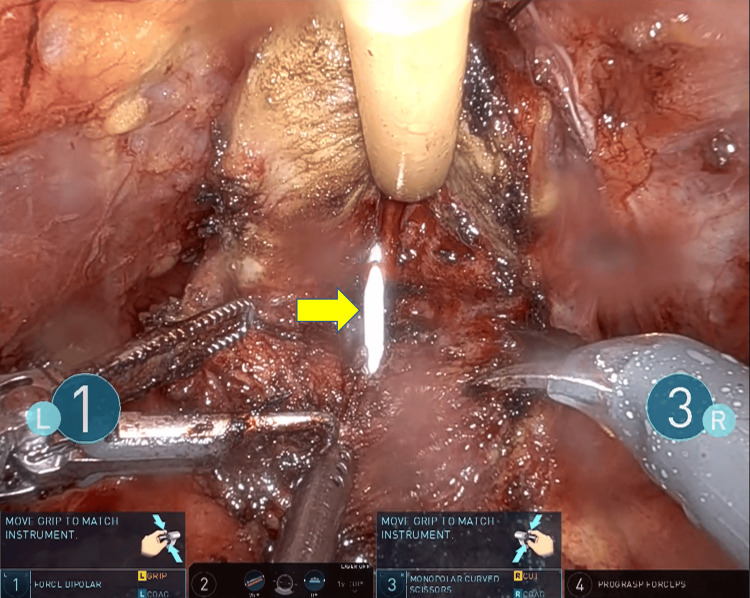 Figure 4
Figure 4| Timing of the diagnosis of ectopic ureter | Authors | Diagnostic trigger | Management of ectopic ureter | Site of ectopic ureteral insertion |
| Preoperative | Hubosky et al. (2007) [ | - | Ureteroureterostomy and ureteroneocystostomy | Prostatic urethra |
| Preoperative | Funahashi et al. (2007) [ | - | Ureteroureterostomy | Prostatic urethra |
| Preoperative | Marien et al. (2008) [ | - | Ureteroureterostomy | Prostatic urethra |
| Preoperative | Matsumoto et al. (2016) [ | - | Ureteral ligation | Seminal vesicle |
| Preoperative | Nakai et al. (2009) [ | - | Nephroureterectomy | Seminal vesicle |
| Preoperative | Miyago et al. (2012) [ | - | Upper pole heminephrectomy | Prostatic urethra |
| Preoperative | Spinos et al. (2023) [ | - | Ureteral ligation | Seminal vesicle |
| Preoperative | Present case | - | No treatment | Bladder neck |
| Intraoperative | Shariat et al. (2005) [ | - | Nephroureterectomy | Seminal vesicle |
| Intraoperative | Singhal et al. (2015) [ | - | Ureteral ligation | Prostatic urethra |
| POD 2 | Didier et al. (2017) [ | Persistent urinary leakage | Ureteroureterostomy and ureteroneocystostomy | Prostatic urethra |
| POD 3 | Hampton et al. (2008) [ | Persistent urinary leakage | Ureteroureterostomy | Unknown |
| POD 3 | Polo-Alonso et al. (2022) [ | Fever up | Ureteroneocystostomy | Seminal vesicle |
| POD 8 | Ghazi et al. (2011) [ | Persistent urinary leakage | Nephrostomy and ureteroureterostomy | Bladder neck |
| POD 15 | Minh et al. (2013) [ | Fever up | Nephrostomy and ureteral stenting | Bladder neck |
| POM 6 | Petrella et al. (2020) [ | Frank pain | Selective arterial embolization | Prostatic urethra |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrologic and reproductive health conditions · Urological Disorders and Treatments · Ureteral procedures and complications
Introduction
An ectopic ureter is a rare congenital anomaly that predominantly affects females, while in males it typically drains into the prostatic urethra, seminal vesicle, or vas deferens [1]. Radical prostatectomy remains the gold standard for the treatment of prostate cancer, and robot-assisted surgery, in particular, is widely utilized in numerous countries and institutions due to its precise maneuverability and other advantages. In patients with an ectopic ureter, prostatectomy can lead to severe complications if the condition is not diagnosed and addressed preoperatively or intraoperatively, as this may leave a patent ureter in the surgical field. Herein, we report a case of robot-assisted laparoscopic radical prostatectomy (RARP) performed on a patient with an ectopic ureter opening into the bladder neck.
Case presentation
The patient was a 71-year-old man with no significant medical history. In February 2022, a routine health check-up revealed an elevated prostate-specific antigen (PSA) level of 35.83 ng/mL, for which he consulted a physician. A prostate magnetic resonance imaging (MRI) was performed, showing findings suggestive of prostate cancer with extraprostatic extension in the left lobe (Figure 1). Consequently, a prostate biopsy was conducted in March of the same year. The biopsy detected adenocarcinoma with a Gleason score of 4+3=7 in five cores from the left lobe. He was subsequently referred to our department for surgical management. Staging with contrast-enhanced computed tomography (CT) and bone scintigraphy showed no evidence of distant metastasis. However, bilateral complete ureteral duplication was incidentally suspected, prompting a detailed investigation.
Preoperative multiparametric magnetic resonance imaging of the prostateAn extensive lesion suspicious for malignancy, indicated by red arrows, was identified in the ventral aspect of the left prostatic lobe (a: T2-weighted image; b: diffusion-weighted image; c: apparent diffusion coefficient map; and d: contrast-enhanced image).
Cystoscopy identified two right ureteral orifices, one in the orthotopic position and the other in the vesical trigone near the internal urethral orifice. On the left side, only the orthotopic orifice was initially visualized. Suspecting an additional ectopic orifice on the left, a further examination was performed under anesthesia. This revealed an ectopic left ureteral orifice located near the bladder neck, in close proximity to the prostatic urethra (Figure 2). Retrograde pyelography performed through each of the two left orifices opacified two separate renal pelves, confirming complete duplication (Figure 3).
Preoperative cystoscopyRed arrowhead indicates the normal left ureteral orifice (a: trigone of the urinary bladder), and yellow arrowhead indicates the ectopic left ureteral orifice (b: bladder neck).
Preoperative retrograde pyelographyRed arrowhead indicates the left lower-pole renal pelvis (normal kidney), and yellow arrowhead indicates the left upper-pole renal pelvis (atrophic kidney).
Based on these findings, a decision was made to proceed with RARP following the preoperative placement of ureteral stents. Following the preoperative placement of a stent in the left ectopic ureter, the patient underwent RARP with extended pelvic lymph node dissection. The total operative time was eight hours and one minute, with a console time of five hours and 31 minutes. The estimated blood loss was minimal at 20 mL. During the procedure, the indwelling ureteral stent was used as a landmark to guide the bladder neck dissection and avoid injury to the left ectopic ureteral orifice (Figure 4). However, in an effort to carefully preserve this orifice, the dissection plane inadvertently extended into the prostate itself. This resulted in an extensive positive surgical margin at the bladder neck on final pathology. The patient experienced immediate postoperative biochemical recurrence and was subsequently treated with androgen deprivation therapy and salvage radiation therapy. Currently, his PSA level remains at an undetectable level.
A ureteral stent was placed during bladder neck dissectionThe yellow arrowhead indicates a ureteral stent inserted transurethrally into the ectopic ureteral orifice.
Discussion
An ectopic ureter is a congenital anomaly in which the ureter inserts outside the vesical trigone. The incidence is reported to be one in 2,000 to 4,000 individuals, with a significant female predominance at a 7:1 ratio. In males, the ectopic ureteral orifice is always located proximal to the external sphincter, most commonly in the prostatic urethra (54%). Other sites of insertion include the seminal vesicle (28%), vas deferens (10%), and the ejaculatory duct (8%) [1]. In 80-85% of cases, an ectopic ureter is associated with a duplicated renal collecting system [2]. Generally, the orifice of an ectopic ureter originating from a duplicated system follows the Weigert-Meyer rule. In the present case, the presence of a duplicated ureter led to the diagnosis of an ectopic ureter. However, since ectopic orifices can also occur in a single ureteral system, preoperative diagnosis in such cases can be challenging.
RARP is widely established as the standard procedure for prostate cancer treatment due to its precision. However, performing RARP in patients with a coexisting ectopic ureter, a rare anatomical anomaly, poses a risk of postoperative complications such as intraperitoneal urine leakage [3-5] if the condition is not diagnosed preoperatively. Therefore, preoperative diagnosis is crucial for the surgical management of prostate cancer with a concomitant ectopic ureter. Although the ectopic ureter was identified on CT in this case, a report suggests that MRI is also effective for its detection [6]. In our case, the ectopic ureter opened into the bladder neck and was therefore preserved, but this resulted in a positive surgical margin. Given that the upper pole of the kidney on the affected side was atrophic, sacrificing the ureter might have been a better option from an oncological control perspective.
To the best of our knowledge, a literature review revealed 14 previously reported cases of radical prostatectomy in patients with an ectopic ureter (Table 1). Seven cases were diagnosed preoperatively, two intraoperatively, and five were identified postoperatively due to urinary leakage. No postoperative problems were reported in the preoperatively diagnosed cases, whereas all cases identified postoperatively required reoperation, underscoring the critical importance of preoperative diagnosis. The most common site of the ectopic orifice was the prostatic urethra [3,7-12] (seven cases), followed by the seminal vesicle [13-17] (five cases), the bladder neck [5,18] (two cases), and one case in which the location was unknown [4]. Surgical management included urinary tract reconstruction, such as ureteroureterostomy [4,5,17] in three cases, ureteroureterostomy and ureteroneocystostomy [3,8] in two cases, nephroureterectomy [11,13] in two cases (for non-functioning or hypoplastic kidneys), and simple ureteral ligation [7,10,12] in three cases. One case, identified six months postoperatively, was managed with selective arterial embolization of the kidney [9].
Conclusions
We report a case of radical prostatectomy in a patient with prostate cancer and a concomitant ectopic ureter. Preoperative diagnosis of an ectopic ureter allows for careful planning of the surgical approach. A primary objective is to achieve complete tumor resection with negative surgical margins to ensure oncologic control. Concurrently, it is essential to consider the appropriate method for urinary tract reconstruction if it becomes necessary. This anomaly should be suspected if an unexpected tubular structure is encountered intraoperatively or if unexpected urinary leakage occurs postoperatively.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A single-system ectopic ureter in a child: a challenge for early diagnosis Cureus Reinig BA Silva BM Fernandes M Onofre AL Veruska Paiva Ortolan E 016202410.7759/cureus.51834 PMC 1084817738327937 · doi ↗ · pubmed ↗
- 2Ectopic ureter: a concise narrative review with anatomical and clinical commentaries Transl Res Anat Balawender K Wawrzyniak A Pliszka A 100220292022
- 3Robotic assisted common sheath ureteroneocystostomy of an injured ectopic ureter diagnosed in the acute post-operative setting after robotic assisted radical prostatectomy Urol Case Rep Rohloff M Christensen C Maatman T 27291420172870236410.1016/j.eucr.2017.06.004PMC 5496459 · doi ↗ · pubmed ↗
- 4Robot-assisted laparoscopic ipsilateral ureteroureterostomy for injury of an ectopic duplicated ureter following robotic prostatectomy J Robot Surg Hampton L Kawachi M 253255220082763779610.1007/s 11701-008-0113-7 · doi ↗ · pubmed ↗
- 5Delayed detection of injury to an ectopic ureter of a duplicated collecting system following laparoscopic radical prostatectomy for early organ-confined prostate cancer Urol Int Ghazi A Zimmermann R Janetschek G 1211248620112107191810.1159/000321240 · doi ↗ · pubmed ↗
- 6The duplicated collecting system of the urinary tract: embryology, imaging appearances and clinical considerations Pediatr Radiol Didier RA Chow JS Kwatra NS Retik AB Lebowitz RL 152615384720172904342110.1007/s 00247-017-3904-z · doi ↗ · pubmed ↗
- 7Robotically assisted radical laparoscopic prostatectomy in a patient with ectopic ureteral insertion into the prostate J Robot Surg Hubosky SG Davis JW Given RW Fabrizio MD 8588120072548494110.1007/s 11701-006-0005-7PMC 4247429 · doi ↗ · pubmed ↗
- 8Radical prostatectomy for prostate carcinoma with ectopic ureter; a case report Nihon Hinyokika Gakkai Zasshi Funahashi Y Kamihira O Kasugai S Kimura K Fukatsu A Matsuura O 5805829820071741937010.5980/jpnjurol 1989.98.580 · doi ↗ · pubmed ↗