Long‐Term Survival of Two Versus Three Courses of Preoperative Cisplatin and Fluorouracil Plus Docetaxel for Locally Advanced Esophageal Cancer: A Multicenter Randomized Phase II Trial
Takahito Sugase, Hiroshi Miyata, Takashi Kanemura, Norihiro Matsuura, Tomoki Makino, Makoto Yamasaki, Koji Tanaka, Kotaro Yamashita, Kota Momose, Osamu Shiraishi, Keijiro Sugimura, Masaaki Motoori, Kazumasa Fujitani, Atsushi Takeno, Motohiro Hirao, Yutaka Kimura, Taroh Satoh

TL;DR
This study compares two versus three chemotherapy cycles before surgery for esophageal cancer and finds no significant difference in long-term survival.
Contribution
The study provides evidence that two cycles of preoperative chemotherapy may be as effective as three cycles for locally advanced esophageal cancer.
Findings
No significant difference in 5-year overall survival between two and three chemotherapy cycles.
Subgroup analysis showed better outcomes for younger patients and responders in the three-cycle group.
Non-responders in the three-cycle group had worse survival outcomes.
Abstract
Preoperative chemotherapy with cisplatin, fluorouracil, and docetaxel (DCF) is one of the neoadjuvant treatments for locally advanced esophageal squamous cell carcinoma (ESCC). However, the optimal number of DCF cycles remains unknown. This multi‐institutional, randomized, phase II trial aimed to investigate the long‐term survival outcomes of two versus three courses of DCF. A total of 180 patients with locally advanced ESCC from six institutions were randomly assigned to receive either two (N = 91) or three (N = 89) courses of DCF administered every 3 weeks prior to surgery. Long‐term survival outcomes were compared between the two regimens. Baseline characteristics were well balanced between the two groups. The 5‐year overall survival (OS) and progression‐free survival (PFS) rates for the three and two course groups were 70.7% vs. 63.8% (hazard ratio (HR) = 0.91, p = 0.717) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
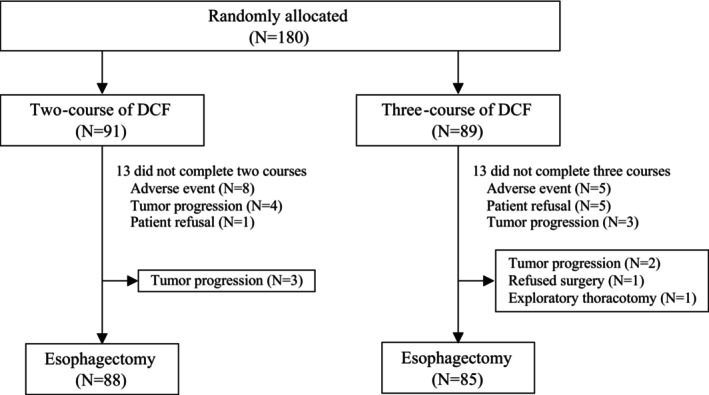 FIGURE 1
FIGURE 1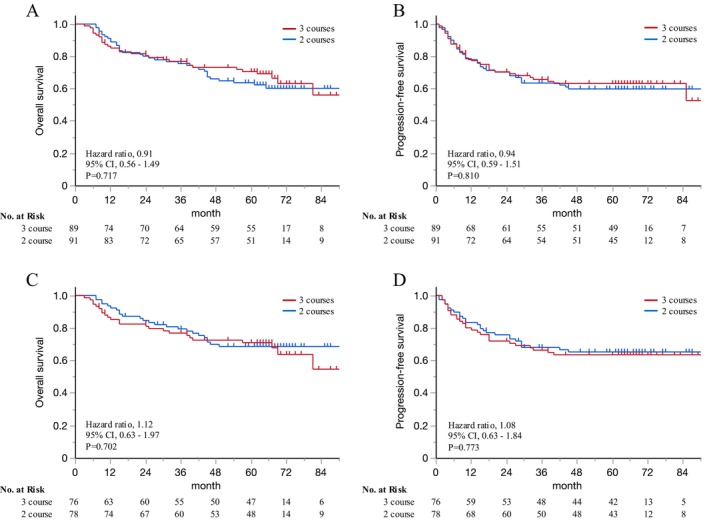 FIGURE 2
FIGURE 2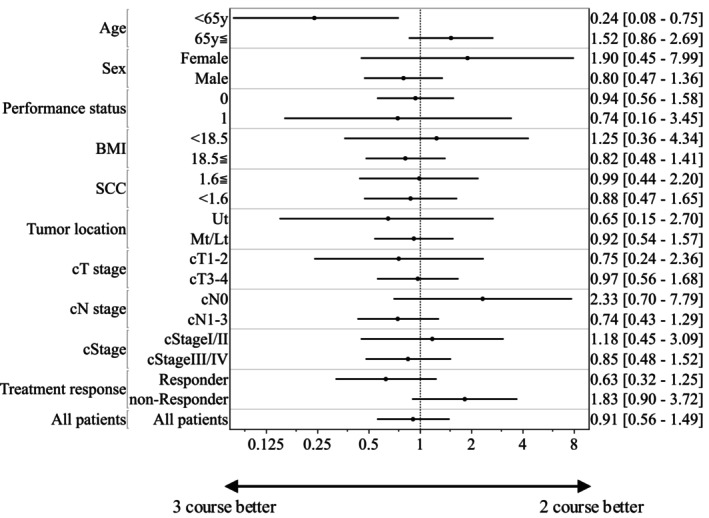 FIGURE 3
FIGURE 3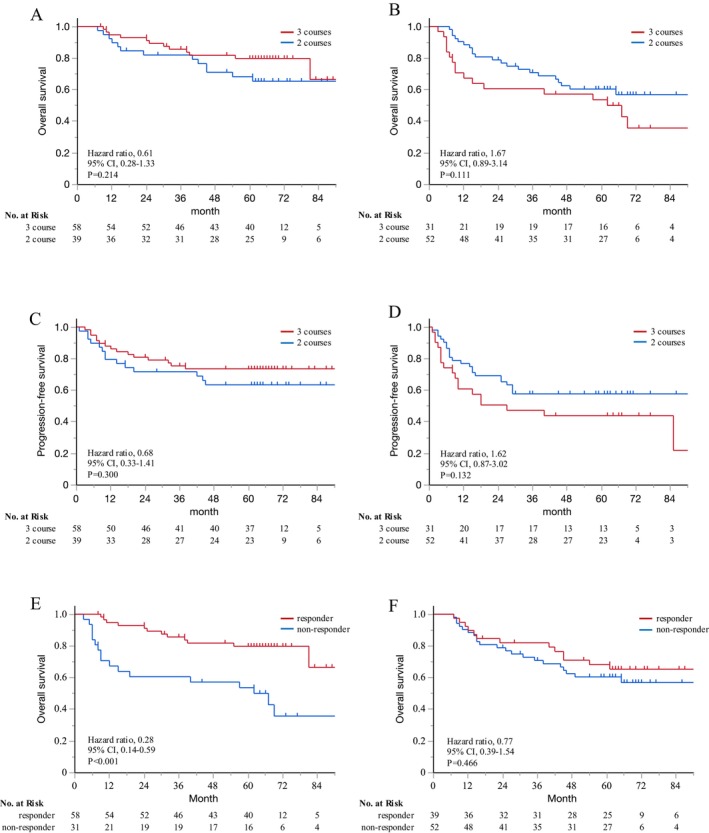 FIGURE 4
FIGURE 4| 2‐course DCF | 3‐course DCF |
| |||
|---|---|---|---|---|---|
|
|
| ||||
|
| |||||
| Age, years, median (range) | 67 | (37–79) | 67 | (44–79) | 1.000 |
| Sex, | 0.786 | ||||
| Male | 78 | (86) | 75 | (84) | |
| Female | 13 | (14) | 14 | (16) | |
| Performance status (ECOG), | 0.836 | ||||
| 0 | 82 | (90) | 81 | (91) | |
| 1 | 9 | (10) | 8 | (9) | |
| BMI, kg/m2, median (range) | 20.9 | (16.0–30.1) | 21.6 | (14.2–30.9) | 0.349 |
| Tumor marker (SCC 1.6≦), | 31 | (34) | 32 | (36) | 0.791 |
| Tumor location, | 0.587 | ||||
| Upper | 16 | (18) | 13 | (15) | |
| Middle/Lower | 75 | (82) | 76 | (85) | |
| cT stage, | 0.920 | ||||
| 1–2 | 28 | (31) | 28 | (31) | |
| 3–4 | 63 | (69) | 61 | (69) | |
| cN stage, | 0.908 | ||||
| 0–1 | 73 | (80) | 72 | (81) | |
| 2–3 | 18 | (20) | 17 | (19) | |
| cStage, | 0.465 | ||||
| I—II | 32 | (35) | 36 | (41) | |
| III—IV | 59 | (65) | 44 | (59) | |
|
| |||||
| Completion of planned courses, | 78 | (86) | 76 | (85) | 0.951 |
| Dose reduction during planned courses, | 63 | (69) | 70 | (79) | 0.150 |
| Overall adverse events, | |||||
| ≧ grade 4 | 68 | (75) | 71 | (80) | 0.419 |
| Clinical treatment response, | |||||
| CR | 0 | (0) | 1 | (1) | |
| PR | 39 | (43) | 57 | (64) | |
| SD | 49 | (54) | 29 | (33) | |
| PD | 3 | (3) | 2 | (2) | |
| RR | 39 | (43) | 58 | (65) | 0.003 |
|
| |||||
| ypStage, | 0.077 | ||||
| 0 | 5 | (6) | 11 | (12) | |
| I | 19 | (21) | 12 | (14) | |
| II | 33 | (36) | 24 | (27) | |
| III | 28 | (31) | 29 | (33) | |
| IV | 3 | (3) | 9 | (10) | |
| Not resected | 3 | (3) | 4 | (4) | |
| Histopathological response, | 0.898 | ||||
| Grade 0 | 3 | (3) | 2 | (2) | |
| Grade 1a | 27 | (30) | 31 | (35) | |
| Grade 1b | 23 | (25) | 18 | (20) | |
| Grade 2 | 27 | (30) | 21 | (24) | |
| Grade 3 | 8 | (9) | 13 | (15) | |
| Not resected | 3 | (3) | 4 | (4) | |
| All | 2‐course DCF | 3‐course DCF |
| |||
|---|---|---|---|---|---|---|
|
|
| |||||
| Overall | 52 | 27 | (31%) | 25 | (30%) | 0.494 |
| Locoregional recurrence | 16 | 9 | (10%) | 7 | (8%) | 0.426 |
| Distant recurrence | 42 | 21 | (24%) | 21 | (25%) | 0.518 |
| Lymph node | 18 | 10 | (11%) | 8 | (10%) | 0.433 |
| Lung | 11 | 6 | (7%) | 5 | (6%) | 0.525 |
| Bone | 8 | 5 | (6%) | 3 | (4%) | 0.380 |
| Liver | 6 | 4 | (5%) | 2 | (2%) | 0.358 |
| Brain | 3 | 0 | (0%) | 3 | (4%) | 0.116 |
| Pleura | 3 | 2 | (2%) | 1 | (1%) | 0.513 |
| Others | 4 | 1 | (1%) | 3 | (4%) | 0.297 |
| 2‐couse DCF | 3‐couse DCF | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | ||||||||||
| OR | 95%CI |
| OR | 95%CI |
| OR | 95%CI |
| OR | 95%CI |
| ||
| Age | < 65 y vs. 65 y ≦ | 1.47 | [0.73–2.97] | 0.285 | 0.22 | [0.08–0.64] | 0.005 | 0.08 | [0.02–0.35] | < 0.001 | |||
| Sex | female vs. male | 0.54 | [0.16–1.77] | 0.308 | 1.45 | [0.55–3.81] | 0.454 | ||||||
| Performance status | 0 vs. 1 | 0.91 | [0.32–2.59] | 0.860 | 1.17 | [0.34–4.01] | 0.809 | ||||||
| Pretreatment BMI | < 18.5 vs. 18.5 ≦ | 0.46 | [0.19–1.25] | 0.136 | 0.65 | [0.25–1.72] | 0.386 | ||||||
| Tumor marker SCC | < 1.6 vs. 1.6 ≦ | 0.88 | [0.43–1.78] | 0.716 | 0.8 | [0.38–1.67] | 0.554 | ||||||
| Tumor location | Upper vs. Middle/Lower | 0.77 | [0.30–1.99] | 0.589 | 0.73 | [0.25–2.09] | 0.554 | ||||||
| cT stage | 1–2 vs. 3–4 | 0.5 | [0.22–1.15] | 0.103 | 0.38 | [0.15–0.99] | 0.049 | 0.12 | [0.03–0.51] | 0.004 | |||
| cN stage | Negative vs. positive | 0.47 | [0.16–1.33] | 0.154 | 1.36 | [0.60–3.05] | 0.459 | ||||||
| cStage | I‐II vs. III‐IV | 0.47 | [0.21–1.05] | 0.066 | 0.85 | [0.29–2.49] | 0.773 | 0.64 | [0.29–1.41] | 0.269 | |||
| Dose reduction | Full dose vs. reduce/stop | 0.14 | [0.02–1.06] | 0.057 | 0.34 | [0.04–2.67] | 0.306 | 0.29 | [0.04–2.16] | 0.228 | |||
| Completion of planned courses | Completed vs. not completed | 0.24 | [0.11–0.50] | < 0.001 | 0.30 | [0.12–0.76] | 0.010 | 0.76 | [0.31–1.88] | 0.552 | |||
| Clinical treatment response | Responder vs. non‐responder | 0.84 | [0.43–1.64] | 0.606 | 0.3 | [0.14–0.61] | 0.001 | 0.22 | [0.09–0.51] | < 0.001 | |||
| Surgical curability | R0 vs. non‐R0/unresectable | 0.1 | [0.04–0.28] | < 0.001 | 0.32 | [0.63–5.12] | 0.202 | 0.06 | [0.02–0.16] | < 0.001 | 0.26 | [0.04–1.67] | 0.155 |
| pT stage | 1–2 vs. 3–4 | 0.22 | [0.10–0.50] | < 0.001 | 0.56 | [0.20–1.59] | 0.274 | 0.47 | [0.22–1.02] | 0.056 | 0.85 | [0.25–2.83] | 0.790 |
| pN stage | 0–1 vs. 2–3 | 0.26 | [0.13–0.54] | < 0.001 | 0.41 | [0.15–1.14] | 0.088 | 0.36 | [0.16–0.81] | 0.013 | 0.26 | [0.08–0.87] | 0.029 |
| pStage | I‐II vs. III‐IV | 0.2 | [0.10–0.43] | < 0.001 | 0.60 | [0.19–1.93] | 0.393 | 0.41 | [0.18–0.94] | 0.034 | 0.88 | [0.22–3.52] | 0.854 |
| Histopathological response | Grade 2–3 vs. 0–1 | 0.29 | [0.12–0.70] | 0.006 | 0.60 | [0.23–1.55] | 0.291 | 0.44 | [0.18–1.05] | 0.065 | 0.48 | [0.17–1.32] | 0.155 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes · Esophageal and GI Pathology
Introduction
1
Esophageal cancer ranks tenth among the most commonly diagnosed cancers and sixth as a leading cause of cancer‐related mortality worldwide [1]. Despite advancements in multidisciplinary treatments, including surgery, radiotherapy, chemotherapy, and immunotherapy [2, 3, 4, 5, 6, 7, 8, 9], the prognosis of patients with esophageal cancer remains poor. Preoperative treatment followed by surgery has been employed to manage advanced esophageal cancer, aiming to achieve a higher R0 resection rate, eliminate micrometastases, and reduce the risk of recurrence [2, 3, 5, 10].
Since the CROSS trial, neoadjuvant chemoradiotherapy has become the standard treatment for patients with resectable esophageal cancer in Western countries [3, 4]. The JCOG9907 trial demonstrated that preoperative chemotherapy with two courses of cisplatin and 5‐fluorouracil (CF) improved long‐term survival compared with postoperative CF in patients with locally advanced esophageal squamous cell carcinoma (ESCC). Consequently, neoadjuvant chemotherapy (NAC) has emerged as an alternative treatment [10]. To improve treatment outcomes, including addressing microscopic metastatic disease, achieving tumor downstaging, and increasing resectability, triplet NAC regimens and CF plus docetaxel (DCF) have been introduced. Our multicenter randomized phase II trial (OGSG1003) revealed that two courses of NAC with DCF prolonged the recurrence‐free survival (RFS) and overall survival (OS) in patients with resectable advanced ESCC [11, 12]. Recently, a randomized phase III trial (JCOG1109) focused on preoperative treatment for resectable ESCC and compared preoperative DCF with CF (standard arm) and CF plus radiotherapy (RT). This study confirmed that three courses of DCF followed by esophagectomy resulted in statistically significant improvements on OS compared to that of the two courses of CF. Conversely, neoadjuvant treatment with two courses of CF plus RT did not demonstrate a significant survival advantage over two courses of CF [5]. Based on the findings of the JCOG1109 trial, the Japan Esophageal Society has strongly recommended three courses of DCF as the new standard treatment for locally advanced ESCC.
In daily clinical practice, protocols involving two cycles of cisplatin‐based NAC have been frequently used in several clinical trials [2, 3, 4, 11, 12]. By contrast, the JCOG1109 trial compared three courses of DCF, two courses of CF (standard arm), and two courses of CF plus RT [5]. However, the optimal number of NAC cycles for ESCC has not yet been established, and the effect of an additional course of NAC on the response rate or survival compared with that of the two standard courses remains unclear.
Hence, this multi‐institutional, randomized phase II trial aimed to compare two and three courses of NAC with a DCF regimen to determine the optimal number of NAC cycles required for treating resectable advanced ESCC. Our previous studies indicated that two and three courses of DCF regimens in the NAC setting were similarly feasible. Additional courses of DCF improved NAC responses without increasing the incidence of adverse events or postoperative morbidity. However, the short‐term survival rates were comparable between the two groups [13, 14]. The present study compared the long‐term survival outcomes between the two arms of this randomized phase II trial.
Methods
2
Patients
2.1
The eligibility criteria and results of pretreatment evaluations have been described in detail in previous studies [13, 14]. Patients aged ≥ 20 years, with a performance status score of 0–1, who were histologically diagnosed with ESCC, and who exhibited adequate primary organ function were considered eligible for the study. The ESCC stages included cT1‐4a N0‐3 M0 and/or M1LYM metastases confined to the supraclavicular lymph nodes, based on the seventh edition of the Union for International Cancer Control TMN classification [15]. Patients who achieved a complete response (CR) or partial response (PR) were classified as responders, whereas those with stable disease (SD) or progressive disease (PD) were classified as non‐responders [14]. All patients provided written informed consent to participate in the study. The study was approved by the institutional review boards of the six participating hospitals prior to patient enrollment. The study was conducted in accordance with the principles of the Helsinki Declaration and registered with the University Hospital Medical Information Network Clinical Trials Registry (identification number: UMIN 000015788).
Study Treatment
2.2
In this open‐label randomized phase II trial, all eligible patients were randomly assigned to receive either two or three courses of DCF. Each DCF course included docetaxel 70 mg/m^2^ (1 h intravenous infusion) plus cisplatin 70 mg/m^2^ (1 h intravenous infusion) on day 1, followed by 5‐fluorouracil 700 mg/m^2^ (continuous intravenous infusion) for 5 days. The courses were administered every 3 weeks [16, 17, 18, 19, 20]. Randomization was stratified according to institution, cT stage, and cN stage using the least‐squares method.
To manage adverse effects, the doses of the likely causal agents were adjusted in subsequent cycles as follows [12, 13]: for grade 4 leukopenia or neutropenia, febrile neutropenia, or grade 3 thrombocytopenia, the doses of all chemotherapy agents were reduced by 20%; for grade 3 stomatitis or diarrhea, the 5‐FU and docetaxel doses were reduced by 20%; and for grade 2 nephrotoxicity, the cisplatin dose was reduced by 20%. A second cycle was administered unless disease progression or unacceptable toxicity occurred.
Surgery was scheduled 3–6 weeks after the last chemotherapy cycle. Patients underwent subtotal esophagectomy with either two‐ or three‐field lymphadenectomy with curative intent, performed via the right thoracotomy or thoracoscopic approach [16, 18, 20, 21, 22]. Transhiatal esophagectomy was not permitted. Regional lymphadenectomy included the mediastinal, perigastric, and celiac nodes, whereas distant lymphadenectomy included the cervical nodes.
Evaluation of Clinical Responses
2.3
The clinical evaluation of tumor response after chemotherapy was performed using contrast‐enhanced 64‐slice computed tomography (CT) or esophagoscopy when tumors were undetectable or unmeasurable by CT. The primary tumor size was assessed bi‐dimensionally by measuring the greatest diameter and its perpendicular length. Lymph node response was evaluated by measuring the minor axis of metastatic lymph nodes with a diameter of ≥ 10 mm, and the total sum was calculated according to the Response Evaluation Criteria in Solid Tumors (RECIST) guidelines. The chemotherapeutic response was determined based on the percentage reduction in the primary tumor area and the sum of the minor axes of metastatic lymph nodes [13]. Clinical responses were classified as follows: CR, defined as complete regression of the disease confirmed by CT and endoscopy; PR, defined as a reduction of more than 50% in the primary tumor size and more than 30% in the size of metastatic lymph nodes; PD, defined as an increase of more than 25% in the primary tumor size or the appearance of new lesions, or an increase of more than 20% in metastatic lymph nodes; and SD, defined as cases not meeting the criteria for PR or PD. The overall clinical response was determined based on the worst outcome observed in either the primary tumor or the lymph nodes.
Follow‐Up
2.4
Patients were followed up every 3 months for the first 2 years after random assignment, every 6 months for the next 3 years, and annually [22, 23, 24]. Disease recurrence was categorized as locoregional (in the esophageal bed, anastomotic site, or regional lymph nodes) or distant (in non‐regional lymph nodes, excluding supraclavicular lymph nodes, or distant organs) [18, 25]. The histopathological tumor response was evaluated based on the Japanese Society for Esophageal Disease criteria. Briefly, the evaluations were classified into five categories according to the proportion of tumors affected by degeneration or necrosis [20, 26].
Statistical Analysis
2.5
The sample size for this study was calculated as follows: 164 patients were required to detect an increase in the 2‐year PFS, from 55% in the two course group to 70% in the three course group, with 80% power to identify a significant difference between the groups and a 10% type I error. Assuming an approximate dropout rate of 10%, 180 patients were enrolled. Continuous variables were expressed as medians and ranges. Nonparametric variables were compared between the groups using the Mann–Whitney U test. Categorical data were expressed as frequencies (percentages) and compared between the groups using Fisher's exact test or Pearson's χ ^2^ test. The level of significance was set at a p value of 0.05. Progression‐free survival (PFS) and OS were calculated from the date of random assignment, estimated using the Kaplan–Meier method, and compared using the log‐rank test on an intent‐to‐treat basis. To assess the effects of the contributing factors, we calculated the hazard ratios (HR) and 95% confidence intervals (CI).
Results
3
Patient Characteristics and Chemotherapy Outcomes
3.1
The clinicopathological characteristics, treatment outcomes, and histopathological findings have been reported in previous studies [13, 14]. A total of 180 patients from six institutions were randomly assigned to receive either two (N = 91) or three (N = 89) courses of DCF between July 2014 and December 2018. The number of patients enrolled in each hospital ranged from 4 to 73, with a mean of 30. In the two course DCF group, 78 (86%) patients completed both courses of preoperative DCF. The reasons for not completing both chemotherapy courses included severe adverse effects (N = 8), PD (N = 4), and patient refusal (N = 1). In the three course DCF group, 76 patients (85%) completed all three courses. The reasons for the non‐completion of planned NAC courses in this group were severe adverse effects (N = 5), patient refusal (N = 5), and PD (N = 3) (Figure 1).
The Consolidated Standards of Reporting Trials diagram presents the patient allocation, treatment, and outcomes. DCF, Docetaxel, cisplatin, and 5‐fluorouracil.
The patients were predominantly men (85%), with a median age of 67 years (range, 37–79 years). Most patients developed tumors in the middle or lower thorax (84%), with the majority classified as having cStage III disease (53%). The treatment groups were well‐matched in terms of baseline characteristics, including age, sex, performance status, body mass index, tumor markers, tumor location, and cStage. The groups exhibited comparable overall rates of grade ≥ 4 adverse events (75% vs. 80%, p = 0.419). At the end of the scheduled chemotherapy, the three course DCF group showed significantly higher rates of overall clinical response compared with the two course DCF group (43% vs. 65%, p = 0.003). Although the three course DCF group showed a relatively higher pathological CR rate than the two course DCF group (6% vs. 12%), the two groups showed similar histological responses for the primary tumor (p = 0.898) (Table 1).
Long‐Term Survival
3.2
The intention‐to‐treat (ITT) analysis showed 5‐year OS rates of 70.7% in the three course DCF group and 63.8% in the two course DCF group (HR: 0.91, 95% CI: 0.56–1.49, p = 0.717; Figure 2A). The 5‐year PFS rates were similar between the two groups: 63.3% in the three course DCF group and 60.0% in the two course DCF group (HR: 0.94, 95% CI: 0.59–1.51, p = 0.810; Figure 2B). The per‐protocol analysis revealed similar 5‐year OS rates between the three course (n = 76) and two course (n = 78) DCF groups (71.1% and 68.8%, respectively; HR: 0.90, 95% CI: 0.51–1.58, p = 0.702; Figure 2C), as well as comparable 5‐year PFS rates (63.6% and 65.4%, respectively; HR: 0.92, 95% CI: 0.54–1.58, p = 0.773; Figure 2D).
Survival analysis: Intention‐to‐treat analysis of the (A) overall survival and (B) progression‐free survival, and per‐protocol analysis of the (C) overall survival and (D) progression‐free survival.
Recurrences
3.3
The two groups showed similar overall disease recurrence rates (31% vs. 30%, p = 0.494). No significant differences were observed in the locoregional or distant recurrence rates between the two groups (locoregional: 10% vs. 8%, p = 0.426; distant: 24% vs. 25%, p = 0.518). Additionally, the proportion of patients who developed distant metastases was similar between the two groups (Table 2).
Subgroup Analysis
3.4
Figure 3 presents the results of the subgroup analysis of the baseline characteristics and clinical treatment responses of 180 patients with ESCC. No significant difference was found between the two and three course DCF regimens across subgroups defined by sex, performance status, body mass index, tumor markers, tumor location, cT stage, cN stage, cStage, or treatment response. However, in the subgroup of patients aged ≤ 65 years, the three course DCF regimen provided a survival benefit over the two course regimen (HR: 0.24, 95% CI: 0.08–0.75, p = 0.014; Figure 3).
The forest plot illustrates hazard ratios (dots) and 95% confidence intervals (lines) for factors that may influence the overall survival. The analysis included 180 patients with esophageal cancer, and the factors represent baseline characteristics.
Next, long‐term survival was compared based on clinical treatment responses, categorizing patients as responders or non‐responders. Among the responders, the 5‐year OS rates were 79.8% in the three course DCF group and 68.2% in the two course DCF group (HR: 0.61, 95% CI: 0.28–1.33, p = 0.214; Figure 4A). In contrast, among non‐responders, the 5‐year OS tended to be worse in the three course DCF group compared to the two course DCF group (5‐year OS: 53.7% vs. 60.4%, HR: 1.67, 95% CI: 0.89–3.14, p = 0.111; Figure 4B). PFS showed a similar trend to OS: the responders exhibited an HR of 0.68 (95% CI: 0.33–1.41, p = 0.300; Figure 4C), whereas the non‐responders showed an HR of 1.62 (95% CI: 0.87–3.02, p = 0.132; Figure 4D). Among patients receiving three courses of DCF, non‐responders had significantly worse 5‐year OS compared with responders (5‐year OS: 79.8% vs. 50.7%, HR: 0.28, 95% CI: 0.14–0.59, p < 0.001; Figure 4E). By contrast, no significant differences were found in long‐term survival between responders and non‐responders in the two course DCF group (5‐year OS: 68.2% vs. 60.4%, HR: 0.77, 95% CI: 0.39–1.54, p = 0.466; Figure 4F).
The results of survival analysis based on clinical treatment responses, categorizing patients into responders and non‐responders and comparing two versus three courses of DCF, are presented as follows: (A) overall survival among responders, (B) overall survival among non‐responders, (C) progression‐free survival among responders, and (D) progression‐free survival among non‐responders. A comparison between responders and non‐responders in each group is presented as follows: (E) overall survival in the three course DCF group and (F) overall survival in the two course DCF group.
The potential factors for OS were investigated in each group. In the three course DCF group, multivariate analysis identified age, cT stage, clinical response, and pN stage as independent factors for OS (p < 0.001, p = 0.004, p < 0.001, and p = 0.029, respectively). In the two course DCF group, multivariate analysis revealed the completion of planned courses as an independent factor for OS (p = 0.010) (Table 3).
Discussion
4
Preoperative treatment followed by surgery has become a widely accepted strategy for treating locally advanced esophageal cancer. Preoperative chemotherapy with the DCF regimen is considered a standard neoadjuvant treatment for locally advanced ESCC [5, 11, 12]. However, the optimal number of NAC cycles for the DCF regimen has not yet been established. This multi‐institutional, randomized phase II trial is the first to demonstrate comparable 5‐year OS and PFS rates between two and three courses of DCF in both ITT and per‐protocol analyses. The pattern of postoperative recurrence was similar between the two groups. Subgroup analysis revealed that non‐responders to three courses of DCF had significantly worse long‐term survival outcomes, whereas this tendency was less pronounced in the two course group. Conversely, three courses of DCF may confer favorable long‐term survival outcomes in patients aged < 65 years or in those with clinical treatment responses. This randomized trial is the first to compare long‐term survival outcomes across different cycles of neoadjuvant DCF therapy for locally advanced esophageal cancer.
Previous studies have demonstrated the long‐term survival benefits of preoperative chemotherapy followed by radical esophagectomy. A large randomized clinical trial (JCOG9907) previously demonstrated that two courses of CF administered preoperatively significantly improved long‐term survival compared with two courses of CF administered postoperatively for locally advanced ESCC. This trial reported a 5‐year OS rate of 43% in patients with preoperative CF [10]. To further enhance the response rate to NAC and improve survival outcomes, the OGSG1003 trial compared two courses of triplet NAC regimens: DCF and CF combined with adriamycin (ACF) [12]. This trial found that DCF was associated with better long‐term survival compared with ACF in patients with resectable ESCC, with 5‐year OS rates of 63.5% for DCF and 49.4% for ACF [11]. Based on these findings, we hypothesized that an additional course of DCF could further improve survival outcomes by eradicating micrometastases beyond the surgical field. In this study, the 5‐year OS rates of the two course DCF were 63.8% in the ITT analysis and 68.8% in the per‐protocol analysis, which were comparable to the OGSG1003 trial results. Although the three course DCF exhibited slightly better long‐term survival outcomes compared with the two course DCF (5‐year OS: 70.7% vs. 63.8%), the additional course of DCF did not lead to a statistically significant improvement in long‐term survival (HR: 0.91, p = 0.717). Recently, a randomized, controlled, open‐label, phase 3 trial (JCOG1109) compared the efficacy and safety of two courses of CF, three courses of DCF, and two courses of CF combined with RT in locally advanced ESCC. This study demonstrated a statistically significant OS benefit for three courses of DCF followed by esophagectomy compared with two courses of CF. Although the study did not report the 5‐year survival rates, 3‐year OS rates were 72.1% for three courses of DCF and 62.6% for two courses of CF [5]. In this study, the 3‐year OS rates were 76.9% for three courses of DCF and 75.6% for two courses of DCF. Thus, the long‐term survival outcomes of the three courses of DCF in the present study appear comparable to those reported in the JCOG1109 trial.
Our previous study on short‐term outcomes found that two and three courses of DCF in the NAC setting were equally feasible. An additional course of DCF was associated with a better clinical response rate and a relatively higher pathological CR rate for the primary tumor [13]. By contrast, the pT stage, pN stage, lymphatic invasion, venous invasion, surgical outcomes, and overall pathological responses to NAC were similar between the two groups [14]. Miyata et al. investigated the impact of pathological tumor regression and the number of involved lymph nodes on survival and the occurrence of systemic disease in 405 patients with ESCC who received NAC. This study demonstrated that the post‐treatment nodal status is a useful predictor of prognosis and systemic disease occurrence [20]. Additionally, numerous studies have shown that patients with lymph node metastasis experience poorer survival outcomes [27, 28, 29]. Although three courses of DCF resulted in better clinical treatment responses compared with that of the two courses, the absence of differences in pathological results, including lymph node metastasis [14], between the two groups may explain the similar long‐term prognoses and recurrence patterns in both groups.
In the present study, a subgroup analysis showed that non‐responders to three courses of DCF tended to have worse long‐term survival compared with those who received two courses of DCF. Furthermore, among patients who received three courses of DCF, non‐responders exhibited significantly worse long‐term survival compared with responders (HR: 0.28, p < 0.001). Multivariate analysis of the three course DCF group demonstrated that clinical response was an independent factor for OS. However, this trend was less pronounced in the two course group. These findings suggest that administering an additional course of DCF chemotherapy to non‐responders may negatively affect long‐term survival. Our previous exploratory analysis examined the association between tumor response and survival outcomes in patients receiving three courses of DCF chemotherapy. Approximately 40% of the patients exhibited less than 10% tumor reduction during the third course, which was independently associated with poorer survival outcomes compared with those with more than 10% tumor reduction. The reduction rate of the primary tumor after the first two courses (tumor reduction rate < 50%) was most strongly correlated with poor tumor response during the third course (reduction rate < 10%) [30]. These results suggest that continuation of NAC until the three courses may worsen the survival of patients who experienced a tumor reduction rate of < 50% after the first two courses.
In contrast to the general findings, certain subgroups showed long‐term survival benefits after receiving three courses of DCF chemotherapy. Specifically, patients aged ≤ 65 years who received three courses of DCF had significantly better long‐term survival compared with those who received two courses. These results are consistent with the findings of our previous study [14]. Multivariate analysis of OS in the three course DCF group further supported these results. These findings suggest that patients aged < 65 years may be suitable candidates for receiving three courses of DCF. Based on these results and our previous study [13, 14, 30], two courses of preoperative DCF followed by radical esophagectomy may be one of the treatment approaches for patients with locally advanced ESCC. Furthermore, DCF therapy as neoadjuvant therapy has the potential to be individualized and optimized by age and accurate assessment of imaging after the first two courses of DCF.
This study was a phase II trial with a small sample size, which limited the ability to establish definitive standards for preoperative treatment. Recently, the JCOG1109 trial provided robust evidence supporting favoring three courses of DCF over two courses of CF. Exploratory analyses of the JCOG1109 data are expected to help refine the optimal number of courses of neoadjuvant chemotherapy.
In conclusion, this study is the first to demonstrate that two courses of preoperative DCF achieve long‐term survival outcomes comparable to those of three courses. For patients with locally advanced ESCC, two courses of preoperative DCF followed by radical esophagectomy can be one of the potential treatment strategies.
Author Contributions
Takahito Sugase: data curation, writing – original draft. Hiroshi Miyata: data curation, writing – review and editing. Takashi Kanemura: data curation. Norihiro Matsuura: data curation. Tomoki Makino: data curation, project administration, resources. Makoto Yamasaki: data curation. Koji Tanaka: data curation. Kotaro Yamashita: data curation. Kota Momose: data curation. Osamu Shiraishi: data curation, project administration. Keijiro Sugimura: data curation. Masaaki Motoori: data curation. Kazumasa Fujitani: data curation. Atsushi Takeno: data curation. Motohiro Hirao: data curation. Yutaka Kimura: data curation. Taroh Satoh: data curation. Masahiko Yano: data curation. Yuichiro Doki: conceptualization, project administration. Takushi Yasuda: conceptualization, project administration.
Ethics Statement
The study was approved by the institutional review boards of the six participating hospitals prior to patient enrollment. The study was conducted in accordance with the principles of the Helsinki Declaration and registered with the University Hospital Medical Information Network Clinical Trials Registry.
Conflicts of Interest
Yuichiro Doki is an Editorial Board member of the Annals of Gastroenterological Surgery. All remaining authors declare no conflict of interests for this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. Sung , J. Ferlay , R. L. Siegel , et al., “Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA: A Cancer Journal for Clinicians 71, no. 3 (2021): 209–249.33538338 10.3322/caac.21660 · doi ↗ · pubmed ↗
- 2K. M. Sjoquist , B. H. Burmeister , B. M. Smithers , et al., “Survival After Neoadjuvant Chemotherapy or Chemoradiotherapy for Resectable Oesophageal Carcinoma: An Updated Meta‐Analysis,” Lancet Oncology 12, no. 7 (2011): 681–692.21684205 10.1016/S 1470-2045(11)70142-5 · doi ↗ · pubmed ↗
- 3P. van Hagen , M. C. Hulshof , J. J. van Lanschot , et al., “Preoperative Chemoradiotherapy for Esophageal or Junctional Cancer,” New England Journal of Medicine 366, no. 22 (2012): 2074–2084, 10.1056/NEJ Moa 1112088.22646630 · doi ↗ · pubmed ↗
- 4J. Shapiro , P. van Hagen , H. F. Lingsma , et al., “Prolonged Time to Surgery After Neoadjuvant Chemoradiotherapy Increases Histopathological Response Without Affecting Survival in Patients With Esophageal or Junctional Cancer,” Annals of Surgery 260, no. 5 (2014): 807–814.25379852 10.1097/SLA.0000000000000966 · doi ↗ · pubmed ↗
- 5K. Kato , R. Machida , Y. Ito , et al., “Doublet Chemotherapy, Triplet Chemotherapy, or Doublet Chemotherapy Combined With Radiotherapy as Neoadjuvant Treatment for Locally Advanced Oesophageal Cancer (JCOG 1109 N Ex T): A Randomised, Controlled, Open‐Label, Phase 3 Trial,” Lancet 404, no. 10447 (2024): 55–66.38876133 10.1016/S 0140-6736(24)00745-1 · doi ↗ · pubmed ↗
- 6K. Sugimura , H. Miyata , K. Tanaka , et al., “Multicenter Randomized Phase 2 Trial Comparing Chemoradiotherapy and Docetaxel Plus 5‐Fluorouracil and Cisplatin Chemotherapy as Initial Induction Therapy for Subsequent Conversion Surgery in Patients With Clinical T 4b Esophageal Cancer: Short‐Term Results,” Annals of Surgery 274, no. 6 (2021): e 465–e 472.33065643 10.1097/SLA.0000000000004564 · doi ↗ · pubmed ↗
- 7J. M. Sun , L. Shen , M. A. Shah , et al., “Pembrolizumab Plus Chemotherapy Versus Chemotherapy Alone for First‐Line Treatment of Advanced Oesophageal Cancer (KEYNOTE‐590): A Randomised, Placebo‐Controlled, Phase 3 Study,” Lancet 398, no. 10302 (2021): 759–771.34454674 10.1016/S 0140-6736(21)01234-4 · doi ↗ · pubmed ↗
- 8Y. Doki , J. A. Ajani , K. Kato , et al., “Nivolumab Combination Therapy in Advanced Esophageal Squamous‐Cell Carcinoma,” New England Journal of Medicine 386, no. 5 (2022): 449–462.35108470 10.1056/NEJ Moa 2111380 · doi ↗ · pubmed ↗