Disparities in minimally invasive surgery for elective inguinal hernia repair across Europe: secondary analysis of an international cohort study
Maria Picciochi, Alberto G Barranquero

TL;DR
Minimally invasive surgery for hernia repair is used much more in Western Europe than in Southern Europe, showing big differences in access to advanced surgical techniques.
Contribution
The study reveals significant regional disparities in minimally invasive surgery adoption for hernia repair across Europe.
Findings
Western Europe had the highest use of minimally invasive surgery (70.6%), while Southern Europe had the lowest (15.4%).
Bilateral hernias, high-volume surgeons, and private hospitals were linked to higher use of minimally invasive surgery.
Southern Europe needs targeted efforts to improve access to advanced surgical techniques.
Abstract
Healthcare systems in Europe vary in funding, accessibility, and spending per capita, potentially influencing patient access to advanced surgical techniques. This study aimed to provide a snapshot of the utilization of minimally invasive surgery for elective inguinal hernia repair across Europe. This was a secondary analysis of an international, prospective observational study of inguinal hernia repairs conducted between 30 January and 21 May 2023. Adults undergoing elective inguinal hernia repair in Europe were included in the present analysis. The four European regions according to the United Nations geoscheme (Southern, Eastern, Northern, and Western Europe) were compared. A multilevel multivariable logistic regression model was used to explore factors associated with use of minimally invasive surgery. A total of 8355 patients from 254 hospitals across 23 European countries were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1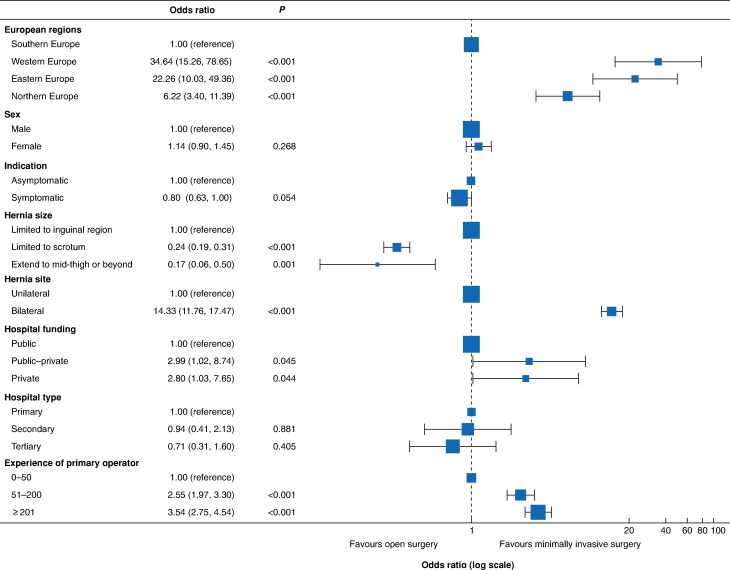 Fig. 2
Fig. 2| Southern Europe | Eastern Europe | Northern Europe | Western Europe | Total | |
|---|---|---|---|---|---|
| Age (years), mean(s.d.) | 62.4(14.1) | 58.9(15.0) | 61.3(15.9) | 60.5(15.4) | 61.8(14.6) |
|
| |||||
| Male | 5044 (90.2%) | 540 (92.2%) | 1434 (93.1%) | 585 (91.8%) | 7603 (91.0%) |
| Female | 546 (9.8%) | 46 (7.8%) | 107 (6.9%) | 52 (8.2%) | 751 (9.0%) |
|
| |||||
| I–II | 4631 (82.8%) | 486 (82.8%) | 1217 (79.0%) | 498 (78.2%) | 6832 (81.8%) |
| III–V | 930 (16.6%) | 98 (16.7%) | 304 (19.7%) | 136 (21.4%) | 1468 (17.6%) |
| Not recorded | 29 (0.5%) | 3 (0.5%) | 20 (1.3%) | 3 (0.5%) | 55 (0.7%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| 0 | 4146 (74.2%) | 441 (75.3%) | 1114 (72.3%) | 477 (74.9%) | 6178 (74.0%) |
| 1 | 1079 (19.3%) | 105 (17.9%) | 311 (20.2%) | 113 (17.7%) | 1608 (19.2%) |
| 2 | 285 (5.1%) | 27 (4.6%) | 89 (5.8%) | 32 (5.0%) | 433 (5.2%) |
| ≥ 3 | 78 (1.4%) | 13 (2.2%) | 26 (1.7%) | 15 (2.4%) | 132 (1.6%) |
| Missing | 2 (0.0%) | 0 (0%) | 1 (0.1%) | 0 (0%) | 3 (0.0%) |
|
| |||||
| Limited to inguinal region | 4706 (84.2%) | 505 (86.0%) | 1297 (84.2%) | 581 (91.2%) | 7089 (84.8%) |
| Limited to scrotum | 821 (14.7%) | 76 (12.9%) | 238 (15.4%) | 54 (8.5%) | 1189 (14.2%) |
| Extend to mid-thigh or beyond | 63 (1.1%) | 6 (1.0%) | 6 (0.4%) | 2 (0.3%) | 77 (0.9%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| Asymptomatic | 804 (14.4%) | 71 (12.1%) | 131 (8.5%) | 71 (11.1%) | 1077 (12.9%) |
| Symptomatic | 4786 (85.6%) | 516 (87.9%) | 1410 (91.5%) | 566 (88.9%) | 7278 (87.1%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| Unilateral | 4814 (86.1%) | 526 (89.6%) | 1366 (88.6%) | 472 (74.1%) | 7178 (85.9%) |
| Bilateral | 776 (13.9%) | 61 (10.4%) | 175 (11.4%) | 165 (25.9%) | 1177 (14.1%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Southern Europe | Eastern Europe | Northern Europe | Western Europe | Total | |
|---|---|---|---|---|---|
|
| |||||
| Public | 5075 (90.8%) | 333 (56.7%) | 1519 (98.6%) | 496 (77.9%) | 7423 (88.8%) |
| Public–private | 377 (6.7%) | 0 (0%) | 0 (0%) | 92 (14.4%) | 469 (5.6%) |
| Private | 115 (2.1%) | 254 (43.3%) | 0 (0%) | 49 (7.7%) | 418 (5.0%) |
| Missing | 23 (0.4%) | 0 (0%) | 22 (1.4%) | 0 (0%) | 45 (0.5%) |
|
| |||||
| Primary | 592 (10.6%) | 61 (10.4%) | 164 (10.6%) | 111 (17.4%) | 928 (11.1%) |
| Secondary | 2282 (40.8%) | 274 (46.7%) | 537 (34.8%) | 117 (18.4%) | 3210 (38.4%) |
| Tertiary | 2693 (48.2%) | 252 (42.9%) | 818 (53.1%) | 409 (64.2%) | 4172 (49.9%) |
| Missing | 23 (0.4%) | 0 (0%) | 22 (1.4%) | 0 (0%) | 45 (0.5%) |
|
| |||||
| No | 38 (0.7%) | 45 (7.7%) | 31 (2.0%) | 0 (0%) | 114 (1.4%) |
| Yes—assessment only and transfer for surgery | 179 (3.2%) | 0 (0%) | 0 (0%) | 0 (0%) | 179 (2.2%) |
| Yes—assessment and emergency surgery during daytime | 163 (2.9%) | 49 (8.3%) | 133 (8.8%) | 19 (3.0%) | 364 (4.4%) |
| Yes—assessment and emergency surgery available 24 h | 5187 (93.2%) | 493 (84.0%) | 1355 (89.2%) | 618 (97.0%) | 7653 (92.1%) |
|
| |||||
| Yes | 5195 (93.3%) | 347 (59.1%) | 1519 (100%) | 630 (98.9%) | 7691 (92.6%) |
| No | 372 (6.7%) | 240 (40.9%) | 0 (0%) | 7 (1.1%) | 619 (7.4%) |
| Southern Europe | Eastern Europe | Northern Europe | Western Europe | Total | |
|---|---|---|---|---|---|
|
| |||||
| MIS/MIS converted | 862 (15.4%) | 273 (46.5%) | 584 (37.9%) | 450 (70.6%) | 2169 (26.0%) |
| Open | 4728 (84.6%) | 314 (53.5%) | 957 (62.1%) | 187 (29.4%) | 6186 (74.0%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| Laparoendoscopic | 813 (14.5%) | 265 (45.1%) | 553 (35.9%) | 374 (58.7%) | 2005 (24.0%) |
| Laparoendoscopic converted to open | 23 (0.4%) | 8 (1.4%) | 17 (1.1%) | 6 (0.9%) | 54 (0.6%) |
| Robotic | 26 (0.5%) | 0 (0%) | 14 (0.9%) | 70 (11.0%) | 110 (1.3%) |
| Open | 4728 (84.6%) | 314 (53.5%) | 957 (62.1%) | 187 (29.4%) | 6186 (74.0%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| Yes | 5533 (99.0%) | 576 (98.1%) | 1527 (99.1%) | 636 (99.8%) | 8272 (99.0%) |
| No | 57 (1.0%) | 11 (1.9%) | 14 (0.9%) | 1 (0.2%) | 83 (1.0%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| Transabdominal preperitoneal repair | 566 (10.2%) | 237 (41.1%) | 404 (26.5%) | 263 (41.4%) | 1470 (17.8%) |
| Totally extraperitoneal repair | 260 (4.7%) | 23 (4.0%) | 137 (9.0%) | 180 (28.3%) | 600 (7.3%) |
| Lichtenstein | 3752 (67.8%) | 309 (53.6%) | 886 (58.0%) | 177 (27.8%) | 5124 (61.9%) |
| Plug and patch | 796 (14.4%) | 2 (0.3%) | 30 (2.0%) | 5 (0.8%) | 833 (10.1%) |
| PHS™ † (bilayer) | 17 (0.3%) | 1 (0.2%) | 5 (0.3%) | 9 (1.4%) | 32 (0.4%) |
| Transrectal preperitoneal | 13 (0.2%) | 0 (0%) | 2 (0.1%) | 1 (0.2%) | 16 (0.2%) |
| Transinguinal preperitoneal | 7 (0.1%) | 0 (0%) | 36 (2.4%) | 1 (0.2%) | 44 (0.5%) |
| Other | 122 (2.2%) | 4 (0.7%) | 27 (1.8%) | 0 (0%%) | 153 (1.8%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| Permanent synthetic | 5105 (92.3%) | 497 (86.3%) | 1323 (86.6%) | 556 (87.4%) | 7481 (90.4%) |
| Absorbable synthetic | 328 (5.9%) | 75 (13.0%) | 120 (7.9%) | 48 (7.5%) | 571 (6.9%) |
| Biological | 1 (0.0%) | 3 (0.5%) | 5 (0.3%) | 0 (0%) | 9 (0.1%) |
| Composite | 98 (1.8%) | 1 (0.2%) | 79 (5.2%) | 31 (4.9%) | 209 (2.5%) |
| Missing | 1 (0.0%) | 0 (0%) | 0 (0%) | 1 (0.2%) | 0 (0%) |
|
| |||||
| Not fixed | 726 (13.1%) | 168 (29.2%) | 216 (14.1%) | 160 (25.2%) | 1270 (15.4%) |
| Absorbable suture | 1785 (32.3%) | 85 (14.8%) | 163 (10.7%) | 40 (6.3%) | 2073 (25.1%) |
| Non-absorbable suture | 2524 (45.6%) | 135 (23.4%) | 850 (55.7%) | 220 (34.6%) | 3729 (45.1%) |
| Glue (fibrin/histoacryl) | 219 (4.0%) | 133 (23.1%) | 65 (4.3%) | 182 (28.6%) | 599 (7.2%) |
| Tackers | 278 (5.0%) | 54 (9.4%) | 233 (15.3%) | 34 (5.3%) | 599 (7.2%) |
| Missing | 1 (0.0%) | 1 (0.2%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| Clean | 5572 (99.7%) | 569 (96.9%) | 1531 (99.4%) | 635 (99.7%) | 8307 (99.4%) |
| Clean-contaminated | 14 (0.3%) | 18 (3.1%) | 9 (0.6%) | 2 (0.3%) | 43 (0.5%) |
| Contaminated | 3 (0.1%) | 0 (0%) | 1 (0.1%) | 0 (0%) | 4 (0.0%) |
| Dirty | 1 (0.0%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (0.0%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| No | 5566 (99.6%) | 583 (99.3%) | 1535 (99.6%) | 634 (99.5%) | 8318 (99.6%) |
| Yes | 24 (0.4%) | 4 (0.7%) | 6 (0.4%) | 3 (0.5%) | 37 (0.4%) |
|
| |||||
| General | 2471 (44.2%) | 367 (62.5%) | 1292 (83.8%) | 602 (94.5%) | 4732 (56.6%) |
| Local | 871 (15.6%) | 23 (3.9%) | 135 (8.8%) | 20 (3.1%) | 1049 (12.6%) |
| Regional block | 92 (1.6%) | 0 (0%) | 17 (1.1%) | 3 (0.5%) | 112 (1.3%) |
| Spinal | 2156 (38.6%) | 197 (33.6%) | 97 (6.3%) | 12 (1.9%) | 2462 (29.5%) |
|
| |||||
| Senior surgeon (consultant or attending) | 4082 (73.0%) | 399 (68.0%) | 1209 (78.5%) | 509 (79.9%) | 6199 (74.2%) |
| Trainee surgeon | 1499 (26.8%) | 188 (32.0%) | 329 (21.3%) | 128 (20.1%) | 2144 (25.7%) |
| Non-surgeon, medical practitioners | 9 (0.2%) | 0 (0%) | 3 (0.2%) | 0 (0%) | 12 (0.1%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
|
| |||||
| 0–50 | 990 (17.7%) | 86 (14.7%) | 188 (12.2%) | 90 (14.1%) | 1354 (16.2%) |
| 51–200 | 1475 (26.4%) | 176 (30.0%) | 429 (27.8%) | 186 (29.2%) | 2266 (27.1%) |
| ≥ 201 | 3125 (55.9%) | 325 (55.4%) | 918 (59.6%) | 360 (56.5%) | 4728 (56.6%) |
| Missing | 0 (0%) | 0 (0%) | 6 (0.4%) | 1 (0.2%) | 7 (0.1%) |
| Southern Europe | Eastern Europe | Northern Europe | Western Europe | Total | |
|---|---|---|---|---|---|
|
| |||||
| No | 2413 (43.2%) | 406 (69.2%) | 311 (20.2%) | 359 (56.4%) | 3489 (41.8%) |
| Yes | 3160 (56.5%) | 181 (30.8%) | 1229 (79.8%) | 277 (43.5%) | 4847 (58.0%) |
| Missing | 17 (0.3%) | 0 (0%) | 1 (0.1%) | 1 (0.2%) | 19 (0.2%) |
|
| |||||
| 0 (no complications) | 4903 (87.7%) | 485 (82.6%) | 1425 (92.5%) | 561 (88.1%) | 7374 (88.3%) |
| I–II | 641 (11.5%) | 94 (16.0%) | 101 (6.6%) | 62 (9.7%) | 898 (10.7%) |
| III–V | 33 (0.6%) | 8 (1.4%) | 14 (0.9%) | 13 (2.0%) | 68 (0.8%) |
| Missing | 13 (0.2%) | 0 (0%) | 1 (0.1%) | 1 (0.2%) | 15 (0.2%) |
|
| |||||
| No | 5437 (97.5%) | 566 (96.4%) | 1520 (98.7%) | 627 (98.6%) | 8150 (97.7%) |
| Yes | 140 (2.5%) | 21 (3.6%) | 20 (1.3%) | 9 (1.4%) | 190 (2.3%) |
|
| |||||
| No | 5560 (99.7%) | 585 (99.7%) | 1528 (99.2%) | 629 (98.9%) | 8302 (99.5%) |
| Yes | 17 (0.3%) | 2 (0.3%) | 12 (0.8%) | 7 (1.1%) | 38 (0.5%) |
- —(NIHR) Global Health Research Unit
- —Portuguese Hernia and Abdominal Wall Society
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHernia repair and management · Aortic aneurysm repair treatments · Appendicitis Diagnosis and Management
Introduction
The rising global burden of hernia-related health challenges, combined with advancements in minimally invasive surgical techniques, underscores the need for a comprehensive understanding of access disparities, environmental impacts, and procedural variability across regions. Addressing these issues, the HIPPO (Hernias, Pathway, and Planetary Outcomes for Inguinal Hernia Surgery) study^1^, launched in early 2023, was a global, prospective cohort study involving 18 058 patients from 640 centres across 83 countries, making it one of the largest studies of its kind. Its findings aim to shape policy recommendations, improve surgical training, and promote sustainable operating practices worldwide, representing a crucial step toward equitable and environmentally conscious surgical care that aligns with the diverse needs and capacities of healthcare systems^1,2^.
The results of the HIPPO study have demonstrated that elective inguinal hernia repair is essential for avoiding emergency operations, which are associated with higher rates of bowel resection^1^. Additionally, low- and middle-income countries reported lower rates of mesh repair^3^, a technique currently recommended to reduce the risk of recurrence^4,5^. Furthermore, these countries exhibited lower rates of minimally invasive inguinal hernia operations, emphasizing the need to expand access to these technologies^3^. Current guidelines^5^ recommend a laparoendoscopic technique because of its association with lower postoperative pain and a reduced incidence of chronic pain in patients of both sexes with primary unilateral inguinal hernia, provided that a surgeon with specific expertise and sufficient local/national resources is available. Laparoendoscopic repair is also suggested for bilateral hernia, for active young patients, and for those with high preoperative pain levels^4^.
This secondary analysis within the HIPPO study, focused on Europe, not only provides a snapshot of the current state of hernia surgery but also offers critical insights for developing strategies to promote equitable, high-quality surgical care across the continent. Europe's healthcare systems exhibit remarkable diversity, shaped by varying levels of public funding, accessibility, and health spending per capita^6^. Northern European countries benefit from robust healthcare policies that prioritize widespread access to care and advanced techniques. In contrast, Eastern European countries report lower health expenditures per capita, reflecting limited public funding and greater reliance on out-of-pocket payments^6^. Using inguinal hernia as a tracer condition for access to high-quality surgery^1^, significant variability in laparoscopic hernia surgery rates is evident across Europe, ranging from 4.6% in Italy during the years 2015–2020^7^ to 60.8% in Denmark during 2011–2020^8^. However, most studies have focused on long timeframes or single countries.
The primary aim of this study was to evaluate the rates of minimally invasive elective inguinal hernia surgery across the European regions as defined by the United Nations geoscheme: Southern, Eastern, Northern, and Western Europe^9^. A secondary aim was to identify the factors influencing its use across these regions, examine the adoption of day-case surgery, and evaluate postoperative complications.
Methods
This was a subanalysis of the HIPPO study, an international prospective, cohort study that included patients undergoing primary inguinal hernia repair. The study protocol is publicly available, was registered in ClinicalTrials.gov (NCT05748886) and has been reported fully^1^. The HIPPO study comprised a global analysis of inguinal hernia treatment pathways, encompassing both elective and emergency procedures, as well as paediatric and adult primary repairs, aimed at evaluating reliance on emergency systems, the use of mesh-based repair, and access to minimally invasive surgery (MIS) across countries with varying income levels^1,3^. Any hospital performing inguinal hernia repair was eligible to take part. Data were collected prospectively between 30 January and 21 May 2023, from all consecutive patients undergoing inguinal hernia repair. This analysis is reported in line with STROBE guidelines^10^.
Study population and setting
This analysis included adults, aged ≥ 16 years, undergoing elective primary inguinal hernia repair in hospitals in Europe. Recurrent inguinal hernias, operations through midline incisions, patients in whom no hernia was identified during surgery, and patients for whom the inguinal hernia repair was not the primary procedure were excluded. Patients were compared across the four European regions as defined by the United Nations geoscheme: Southern, Northern, Eastern, and Western Europe^9^.
Data collection
Data were collected prospectively using a standardized protocol and recorded securely on the REDCap platform hosted at the University of Birmingham. Variables captured included patient demographics (age, sex, co-morbidities, American Society of Anesthesiologists (ASA) fitness grade), hernia characteristics, and procedural details such as surgical approach (open, laparoscopic, or robotic), and type of anaesthesia. Postoperative complications were evaluated at 30 days and categorized using the Clavien–Dindo classification system^11^. Each participating centre contributed data with completeness of at least 95%.
Ethics and governance
Ethical approvals for the study were obtained from each participating centre according to local and national regulations. No changes to standard clinical care were implemented during the study; therefore, the study was registered as clinical audit or service evaluation in some centres where this was allowed (for example UK).
Outcomes
The primary outcome of this analysis was use of MIS, defined as laparoscopic or robotic procedures, and included converted operations. Secondary outcomes included 30-day postoperative complications, graded according to the Clavien–Dindo classification^11^, surgical site infection (SSI), using the Centers for Disease Control definition^12^, and adoption of day-case surgery.
Statistical analysis
Descriptive statistics were used to summarize baseline characteristics, with continuous variables reported as mean(standard deviation, s.d.), and categorical variables as frequencies and percentages. Differences between regions were tested using χ^2^ tests for categorical variables and Student's t test for continuous variables.
A multivariable multilevel logistic regression model was conducted to evaluate the influence of European regions on MIS use, adjusting for other factors that were preplanned based on previous literature^3^, and included: hospital funding, hospital type, patient sex, patient's indication for surgery, hernia size, and hernia site. To account for clustering effects, the hospital was included as a random effect in the model. The other outcomes are described as frequency and proportions.
To explore variation in complications across different regions, a multilevel logistic regression model was used. This model included hospitals as a random effect, variables previously shown to be associated with 30-day postoperative complications^1^, and other clinically plausible factors such as surgical experience and hospital funding.
All statistical analyses were undertaken using R statistical software version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two-tailed, with statistical significance set at P < 0.050.
Results
The original HIPPO study collected data from 18 058 patients across 640 hospitals in 83 countries. In this subanalysis, 8355 patients underwent elective inguinal hernia repair in 254 hospitals from 23 European countries. The majority of patients were from Southern Europe (5590 patients), followed by Northern Europe (1541 patients), Western Europe (637 patients), and Eastern Europe (587 patients). Participant countries from different regions are displayed in Fig. 1. The distribution of participating hospitals and enrolled patients by country and European region is shown in Table S1.
European regions based on the United Nations geoschemeCountries participating in the study are highlighted in colour.
Baseline characteristics
Baseline characteristics are summarized in Table 1. Overall, the mean(s.d.) age of the included patients was 61.8(14.6) years. Men constituted the vast majority across all European regions, representing 91.0% of the total sample (7603 patients). The prevalence of significant co-morbidities (grade ASA III–IV) showed minor regional differences, with slightly higher rates in Western Europe (136 of 637, 21.4%) and Eastern Europe (304 of 1541, 19.7%).
Most patients (7278 of 8355, 87.1%) were symptomatic at diagnosis, with 91.5% of patients from Northern Europe (1410 of 1541) reporting symptoms. Asymptomatic patients were more common in Southern Europe (804 of 5590, 14.4%). Unilateral inguinal hernias were the most common presentation across all regions, accounting for 85.9% of patients (7178 of 8355), whereas bilateral hernias represented 14.1% (1177 of 8355). Patients from Western Europe had the highest prevalence of bilateral hernias (165 of 637, 25.9%).
Hospital characteristics
Hospital characteristics are outlined in Table 2. Hospitals participating in the study varied substantially in type and infrastructure, and funding varied significantly across regions. Public hospitals comprised the majority, particularly in Northern Europe (1519 of 1541, 98.6%). On the contrary, private hospitals were most prevalent in Eastern Europe (254 of 587, 43.3%), indicating greater integration of private sector funding in healthcare delivery. Mixed-funding models were observed primarily in Western Europe (14.4%).
The availability of day-case surgery units varied significantly across regions. Northern and Western Europe had the highest rates of treatment in these facilities, at 100% (all 1519 patients) and 98.9% (630 of 637), respectively. In contrast, only 59.1% of patients in Eastern Europe (347 of 587) had access to day-case surgery facilities.
Primary outcomes
- shows a summary of surgical outcomes. The overall rate of MIS in elective inguinal hernia surgery was 26% (2169 of 8355). The highest rates were observed in Western Europe (450 of 637, 70.6%), followed by Eastern Europe (273 of 587, 46.5%) and Northern Europe (584 of 1541, 37.9%). The rate of MIS in Southern Europe was limited to 15.4% (862 of 5590). Robotic surgery was performed in 11% of patients in Western Europe (70 of 637), compared with a lower rate of 0.9% (14 of 1541) in Northern Europe and 0.5% (26 of 5590) in Southern Europe. None of the patients from Eastern Europe underwent robotic inguinal hernia surgery in this study.
The use of MIS by specific patient characteristics is summarized in Table S2. Among women, the rate ranged from 17.0% (93 of 546) in Southern Europe to 80.8% (42 of 52) in Western Europe. For bilateral hernias, similar rates were observed across regions, with rates always above 50%.
The most common MIS procedure performed was transabdominal preperitoneal (TAPP) repair (overall 1470 of 8355, 17.8%) whereas the most common open procedure was the Lichtenstein technique (overall 5124 of 8355, 61.9%). Only 37 patients (0.4%) underwent bowel resection at the time of surgery; the rate also varied across regions.
Overall, 6199 of 8355 interventions (74.2%) were undertaken by senior surgeons. The proportion of operations performed by trainee surgeons in Eastern Europe (188 of 587, 32%) was higher than the overall rate of 25.7% (2144 of 8355).
European regions were associated with the use of MIS, and this variation was observed in the multivariable logistic regression model (Fig. 2). Patients who had surgery in Northern, Eastern, and Western Europe all had a greater likelihood of undergoing MIS. Having surgery in a private hospital (odds ratio (OR) 2.80, 95% confidence interval (c.i.) 1.03 to 7.65) or carried out by surgeons with experience of ≥ 201 procedures (OR 3.54, 2.75 to 4.54), or having bilateral hernias (OR 14.33, 11.76 to 17.47) were also associated with higher rates of MIS. Patients with hernias extending to the scrotum and beyond had a lower likelihood of undergoing MIS.
Multivariable regression model of risk factors for minimally invasive inguinal hernia repairOdds ratios are shown with 95% confidence intervals. The dashed line indicates an odds ratio value of 1.00.
Secondary outcomes
Secondary outcomes are summarized in Table 4. Elective inguinal hernia repair was performed as a day-case procedure in 58% of the sample evaluated (4847 of 8355), with higher rates in Northern Europe (1229 of 1541, 79.8%) and lower rates in Eastern Europe (181 of 587, 30.8%).
The overall complication rate was 11.6% (966 of 8355), and interventions in Eastern Europe showed a higher rate of complications (102 of 587, 17.4%). A similar increase was observed in the proportion of grade I–II complications, according to the Clavien–Dindo classification (16% (94 of 587) versus 10.7% (898 of 8355)), and in the SSI rates (3.6% (21 of 587) versus 2.3% (190 of 8355)).
Nevertheless, the multivariable regression model of risk factors for postoperative complications (Table S3) showed that complication risk was not associated with European region, hospital funding, or experience level of the primary operator. Instead, higher risk was linked to an ASA grade of III–V (OR 1.40, 95% c.i. 1.17 to 1.67; P < 0.001), procedures classified as clean-contaminated, contaminated, or dirty (OR 2.87, 1.30 to 6.35; P = 0.009), and the need for bowel resection (OR 2.38, 1.00 to 5.63; P = 0.049). In contrast, day-case surgery was associated with a reduced risk of 30-day postoperative complications (OR 0.38, 0.32 to 0.46; P < 0.001).
Discussion
The findings of this study support the initial hypothesis that the rate of elective MIS for inguinal hernia repair varies across Europe. This unplanned subgroup analysis of the original global HIPPO study^1^ provides valuable insights into current trends in inguinal hernia repair across Europe. Accurate, up-to-date data on the precise rates of MIS in inguinal hernia repair can be challenging to obtain, with true rates available only from some registry-based studies, although these were often historical and may not truly reflect current practice. In contrast, the present study provides a timely, high-quality snapshot of inguinal hernia repair practices across Europe between 30 January and 21 May 2023.
A significant strength of this study lies in its well conducted reanalysis of pre-existing HIPPO data. These were high-quality data collected using established research methodology that has been demonstrated to be reliable and robust. The analysis plan, although not completed a priori, was established before completion of the statistical testing. The HIPPO data were purely observational and, although they were collected at a local level, the impact of potential observer bias was deemed to be low.
One major limitation of the study is the variation in patient representation from different countries and healthcare settings across the different European regions, which may have influenced the final MIS rates. In the Northern Europe group, the absence of participating centres from Denmark, Norway, and Finland may have led to an underestimation of the use of MIS for inguinal hernia repair. The published literature demonstrates a high rate of use of MIS in these countries, with 60.8% of inguinal hernia repairs in Denmark during 2011–2020 being performed using the TAPP technique^8^. Sweden, the only Nordic country represented in the present study, reported that, in 2021, laparoscopic techniques for inguinal hernia repair were used in approximately 40% of men and up to 80% of women^13^. The Northern Europe group analysed here consisted predominantly of patients from the UK. This limits the ability to compare the present results with previously published literature, as most of the available data are outdated. For example, a previous study^14^ reported a 23.2% MIS rate in England during 2011–2017, which may not reflect current trends.
The data from Eastern Europe may have been disproportionately affected by the high proportion of patients treated in privately funded hospitals (43.3% versus 5.0% overall). Nationwide analysis from Romania^15^ showed that MIS repair was performed in 12.6% of patients in the public system between 2019 and 2021, compared with 50.6% of those in the private system. This is consistent with data reported elsewhere in the literature, showing increased odds of MIS for inguinal hernia repair in private hospitals^3,16,17^.
Having addressed the limitations of the study, it is relevant to highlight that the present results demonstrate a higher rate of MIS in Western Europe (70.6%) than documented previously. Previous studies reported a MIS rate of 56.5% in France during 2015–2021^18^, and 58.6% for unilateral inguinal hernia in the Herniamed Registry (Germany, Austria, and Switzerland) during 2010–2020^19^.
In contrast, the Southern Europe group had lower rates of MIS for inguinal hernia repair (15.4%). This group had a large representation from Italy and Spain, where laparoscopic inguinal hernia repair accounted for only 4.5% of procedures in Italy (2015–2020)^7^ and 5.7% in Spain (2016–2018)^16^. Data from other countries in this region are scarce, but multicentre data identified a MIS rate of 36.4% in the Republic of Northern Macedonia^20^ and 10.3% in Slovenia^21^. This region includes Southeastern European countries, which have fewer economic resources than other high-income European nations^22^, leading to limited access to MIS equipment and issues with mesh availability. Therefore, despite the variation in patient numbers, the present findings are likely to reflect an accurate rate of MIS for inguinal hernia repair in this region.
There has been a steady shift over time from open hernia repair to MIS techniques^7,13,15^. The use of MIS is supported by the latest clinical guidelines, with Europena Hernia Society guidelines recommending laparoscopic techniques for the primary repair of unilateral inguinal hernias^5^, although the decision between totally extraperitoneal repair or TAPP repair should be based on the surgeon's skills, education, and experience^4^. However, these guidelines state that specific patient and hernia characteristics still warrant use of Lichtenstein or open preperitoneal mesh techniques^5^. Patients with multiple co-morbidities or recurrent hernias^23^ or inguinoscrotal hernias^24^ are more likely to undergo open hernia repair. The limited adoption of MIS may reflect surgeon preference^16^ despite adequate surgical expertise, insufficient training among those with limited procedural experience, and concerns about direct costs.
Inguinal hernia guidelines also emphasize the importance of local resources when considering a minimally invasive repair^5^. In Eastern Europe, access to advanced surgical techniques and medical devices for inguinal hernia repair likely depends on out-of-pocket patient payments in the private sector^6^. In some Southern European countries, where public health expenditure is relatively limited compared with that in the rest of the European Union^6^, policymakers often prioritize a higher volume of procedures at a lower direct cost^16^. Greater emphasis on early recovery and improved quality of life could help justify increased resource allocation for advanced technologies in inguinal hernia repair.
The evaluation of 30-day postoperative complications indicates that elective inguinal hernia surgery in Europe is associated with a low risk of severe morbidity, with no significant differences observed across European regions. The risk factors for postoperative complications identified in this study closely align with those known to predict mortality following urgent inguinal hernia surgery^25^. In this context, with the exception of selected high-risk patients, day-case surgery should be more common than reflected in the present data. Although the proportion of patients undergoing outpatient procedures has increased over time^26^, some healthcare systems still rely heavily on inpatient care^6^, and day-case surgery units remain underdeveloped, particularly in Eastern Europe. Besides, the differences in hospital stay between open and minimally invasive inguinal hernia repair are less pronounced than in other surgical fields, such as colonic surgery^27^ or cholecystectomies^28^, where laparoscopy has long been the standard. Expanding the use of day-case surgery could help reduce healthcare costs while maintaining high-quality outcomes^29^, potentially offsetting the increased expenses associated with minimally invasive techniques^30^.
This study also highlighted areas that warrant further observation. Notably, the rate of use of the plug-and-patch technique in Southern Europe was relatively high, accounting for 14.4% of all repairs in the region (796 of 5590), despite recommendations against it owing to the excessive use of foreign material and the associated risk of plug erosion^4^. Additionally, 12.9% of all repairs in the study (1077 of 8355) were performed on asymptomatic hernias. Surgical intervention in such instances should be carefully discussed with the patient, as watchful waiting for asymptomatic inguinal hernias can be suggested in men^4,5^. Further research is needed in this area to prevent unnecessary operations that may strain healthcare systems^31^.
The increasing rates of MIS for inguinal hernia repair and recent clinical guidelines make it imperative that thorough consideration is given to surgical education, and enhancing the experience of residents and fellows in minimally invasive procedures. A minimum of 60 procedures during surgical residency is considered necessary to safely perform open anterior mesh repair for groin hernia without supervision^32^. Limited training opportunities in MIS repair are often a limiting factor, despite the requirement for graduating residents to be competent in performing these techniques^33^. The disparity between different European regions has been recognized by some surgical societies, leading to the creation of the Forward Program of the European Association of Endoscopic Surgeons, which aims to support the technologically less advanced Southeastern Europe by providing education in MIS surgery for young surgeons^34^.
In this setting, robot-assisted surgery may offer a shorter learning curve for inguinal hernia repair with more active participation than laparoscopic procedures^35^, while also providing an opportunity to convert open operations into minimally invasive procedures, potentially benefitting patient outcomes^36^. The rate of robot-assisted procedures remains low in Europe, reaching only 11% in Western Europe and less than 1% in other regions in the present study. Despite its benefits, the higher cost of robot-assisted surgery compared with laparoscopic techniques (€2612 versus €1963)^37^, along with longer operating times^38^, may limit its accessibility in certain healthcare systems^39^, potentially creating new inequities between European regions.
Significant disparities in MIS adoption for elective inguinal hernia repair exist across Europe. Targeted initiatives should especially prioritize Southern Europe to ensure more equitable access to advanced surgical techniques and ensure that practices align with the latest European clinical guidelines.
Supplementary Material
zraf122_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NIHR Global Health Research Unit on Global Surgery . Access to and quality of elective care: a prospective cohort study using hernia surgery as a tracer condition in 83 countries. Lancet Glob Health 2024;12:e 1094–e 110338797188 10.1016/S 2214-109X(24)00142-6 · doi ↗ · pubmed ↗
- 2Picciochi M, East B, Eseenam Agbeko A. Developing impact from the HIPPO study: surgery and health systems research. Impact Surg 2024;1:88–89
- 3National Institute for Health and Care Research (NIHR) Global Health Research Unit on Global Surgery . Global access to technologies to support safe and effective inguinal hernia surgery: prospective, international cohort study. Br J Surg 2024;111:znae 16438985889 10.1093/bjs/znae 164PMC 11235323 · doi ↗ · pubmed ↗
- 4The Hernia Surge Group . International guidelines for groin hernia management. Hernia 2018;22:1–16510.1007/s 10029-017-1668-x PMC 580958229330835 · doi ↗ · pubmed ↗
- 5Stabilini C, Van Veenendaal N, Aasvang E, Agresta F, Aufenacker T, Berrevoet F et al Update of the international Hernia Surge guidelines for groin hernia management. BJS Open 2023;7:zrad 08037862616 10.1093/bjsopen/zrad 080PMC 10588975 · doi ↗ · pubmed ↗
- 6OECD/European Observatory on Health Systems and Policies . State of Health in the EU. https://health.ec.europa.eu/state-health-eu_en (accessed 6 January 2025)
- 7Ortenzi M, Botteri E, Balla A, Podda M, Montori G, Sartori A. Nationwide analysis of open groin hernia repairs in Italy from 2015 to 2020. Hernia 2023;27:1429–143737847334 10.1007/s 10029-023-02902-z PMC 10700422 · doi ↗ · pubmed ↗
- 8Christophersen C, Baker JJ, Fonnes S, Andresen K, Rosenberg J. Lower reoperation rates after open and laparoscopic groin hernia repair when performed by high-volume surgeons: a nationwide register-based study. Hernia 2021;25:1189–119733835325 10.1007/s 10029-021-02400-0 · doi ↗ · pubmed ↗