A scoping review of measurement tools and a content validity evaluation of the University of Jyvaskyla Active Aging Scale (UJACAS)
Rosa Napoletano, Antonella Lopez, Sergio Traficante, Elisabetta Ricciardi, Luigi Tinella, Alessandro Oronzo Caffò, Andrea Bosco, Giuseppina Spano

TL;DR
This paper reviews tools for measuring active aging and evaluates the University of Jyvaskyla Active Aging Scale as a comprehensive option.
Contribution
The paper provides a scoping review and content validity evaluation of the UJACAS questionnaire for active aging.
Findings
25 questionnaires were identified, but they varied in the aspects of active aging they measured.
UJACAS was found to be the most comprehensive and well-translated questionnaire for evaluating active aging.
Heterogeneity in terminology across questionnaires highlights the need for clearer definitions in active aging assessment.
Abstract
The concept of active aging (AA) was defined as the process of optimizing opportunity for health, security, and social participation for older people. While several questionnaires were developed to measure AA, there is no universal consensus on how to measure it, underlining a lack of clarity about what aspects to consider in the evaluation. To contribute to fill this gap, the aims of these two studies were to provide a guide for aging care professionals to choose the most appropriate questionnaire(s) based on a scoping review of the specialist literature and on a content analysis of the questionnaire, that is, the University of Jyvaskyla Active Aging Scale (UJACAS). Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines were used. We found 25 records introducing questionnaires. The content validity evaluation of the most…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
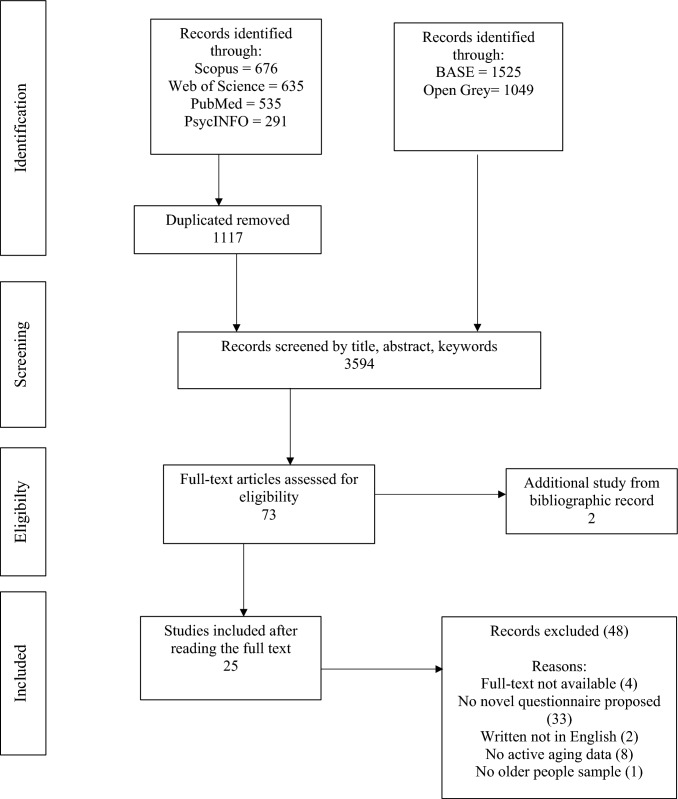 Figure 1
Figure 1- —A.Mi.C.A. Assistenza olistica Intelligente per l’aCtive Ageing in ecosistemi indoor e outdoor” (T1-MZ-09), Traiettoria 1 – Azione 1.1 del Piano operativo salute:“Active & Healthy Ageing - Tecnologie p
- —Testing the efficacy of remote, sustainable empowerment protocols in promoting psycho-physical well-being in the life-span” (Prot. 202284WCP9), PRIN: Progetti Di Ricerca Di Rilevante Interesse Naziona
- —Università degli Studi del Molise
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAging and Gerontology Research · Geriatric Care and Nursing Homes · Frailty in Older Adults
Introduction
Conceptualization of active aging
The phenomenon of population aging is globally significant, with several factors contributing to this trend (e.g., longer life expectancy and greater quality of health care) (Kim et al. 2023). Consequently, as cohorts live longer and have fewer children, these factors have caused changes in the age structures of the population (United Nations 2020). According to the United Nations (2020), older persons are generally defined as such in relation to their chronological age, i.e., from 60 or 65 years of age onwards. Given this demographic shift, ensuring the well-being and autonomy of older individuals has become an important challenge in modern society, given the complexities associated with age-related health issues—cardiovascular, neurodegenerative, musculoskeletal and neuropsychiatric disorders (Li et al. 2021; Sathyanarayana Rao and Shaji 2007). For this reason, the need to preserve health, vitality and independence of older people currently represents a challenge of paramount importance (Storeng et al. 2018). Following this view, the perspective on aging has changed significantly in the gerontological literature. There was a shift away from a pathological perspective of later life to a positive perspective considering later life as a period of success and productivity (Johnson and Mutchler 2014). As a reflection of this positive perspective of aging, the concept of active aging (AA) was defined by World Health Organization (WHO 2002) as “the process of optimizing opportunities for health, participation and security in order to enhance quality of life as people age” (WHO 2002, p.12). Additionally, AA is a goal of health, and social policies aimed to improve three pillars: security, health and participation (WHO 2002). At practical level, AA is influenced by: (a) economic determinants (income capacity, income social protection, autonomy in managing finances, work activity); (b) availability of health and social services (access to healthcare services, to formal caregivers, support to informal caregivers); (c) behavioral determinants (tobacco and alcohol use, regular physical activity, nutritional habits, dental health, pharmacy); (d) social determinants (social support, protection from violence and abuse, literacy and learning); (e) physical environment (environmental characteristics, safe housing, public transport availability, falls, access to clean air and water, safe food); (f) personal determinants (e.g., cognitive functioning, mental health) (WHO 2002). Moreover, International Longevity Centre (2015) expanded the model adding a fourth pillar: lifelong learning. Recently, Hijas-Gómez et al. (2020) conducted a study with the aim of operationalizing the AA framework taking each pillar as an individual construct and using principal component analysis. According to the authors, each pillar is composed as follows:
- Health: psychological health, sleep health, physical health.
- Participation: social activities, social support and leisure perception, physical activity.
- Security: institutional support, leisure grants, housing issues.
- Lifelong learning: level of education and attendance at training activities.
It remains that a fundamental step for professionals involved in promoting aging care is to be able to use streamlined and effective measures to evaluate the quality of AA in older people.
Evaluation of active aging
Evaluation of active aging (AA) is an important issue for policymakers as well as for professionals of care to promote evidence-based interventions improving older peoples’ quality of life (Han et al. 2023). At international level, the first quantitative measure of AA was the Active Aging Index (AAI) developed by Zaidi et al. (2013). AAI was calculated in 28 European Union (EU) countries, and it is composed by 22 indicators based on four domains: employment; participation in society; independent/healthy and secure living; capacity and enabling environment for active aging (i.e., remaining and healthy life expectancy, educational attainment). According to the authors, AAI is useful to develop policies and programs to deal challenges related to aging and it can distinguish multidimensional characteristics of AA. Considering this international perspective, index and sub-indices provide comparable data within EU countries related to untapped potential and various aspects of AA (i.e., social participation, independence, etc.). Calculation of AAI requires access to international surveys and databases. At individual level, AA could be measured through multiple self-report measures (for a review: Han et al. 2023). The assessment at individual level is also useful to analyze subjective well-being, perceived health, individual income and environmental resources (Barslund et al. 2017). Although international and individual level measurements of AA were distinguished, there is no universal consensus on how to measure it due to the presence of a wide range of models and indicators (Paul et al. 2012; Hijas-Gómez et al. 2020). A recent review conducted by Han et al. (2023) aimed to identify the most recommendable measurement tools of AA for use in clinical and research contexts. This was based on an assessment of the psychometric properties of the tools in question, as well as a quality assessment of studies using the Consensus-based standards for the selection of health measurement instruments (COSMIN) risk of bias methodology (Han et al. 2023; COSMIN 2022). Additionally, a scoping review was conducted by Xiao et al. (2024) with the aim to identify available tools for the evaluation of AA in older individuals and their defining characteristics (e.g., year, Country, theoretical framework, number of items, dimensions, sample size, reliability, validity and study level, i.e., individual or macro level) with a particular focus on the applications of these in China.
However, although it is known the presence of a wide range of models and indicators (Paul et al. 2012; Hijas-Gómez et al. 2020), this issue remains poorly investigated. Based on this evidence, it is reasonable to assume that the construction of measurement instruments may often reflect the heterogeneity in AA theories and indicators. As a result, the process of selection of an appropriate questionnaire based on the interest of the researcher and the assessment process itself could be longstanding. Additionally, a choice of questionnaire not in line with the research objectives could lead to an unfocused assessment process with the potential risk of burdening respondents, a major problem when respondents are older people (Rolstad et al. 2011). Indeed, older people reported lower rates of participation/less reliable responses in surveys than younger people due to physical (e.g., sensory disabilities), mental (e.g., cognitive functioning), and motivational (Motel-Klingebiel et al. 2014; Wagner et al. 2018) limitations.
The presence of several models and indicators of AA and the lack of a universal consensus on how to measure this construct could lead to confusion in choosing the most appropriate questionnaire for the assessment process. For this reason, identifying available questionnaires for the assessment of AA could be useful to help aging care professionals in selecting effective, fast and appropriate questionnaire based on the specific aspects of interest. Indeed, the selection of an appropriate questionnaire is crucial to lighten the assessment process and minimizing the burden on respondents by limiting the number of questionnaires they are required to complete, especially when respondents are older people (Rolstad et al. 2011). Additionally, the presence of different models/indicators and different questionnaires highlights the need to analyze in detail each instrument and the specific aspects of the construct investigated by each subscale and item of each instrument.
Research design and purpose/aims
Bearing these issues in mind, our research is focused on the analysis of content areas such as the physical, social, economic, cognitive, psychological/emotional, ecological, and cultural ones and other characteristics such as aims of the questionnaire, available translation for a specific cultural context. Identifying these specific aspects for each questionnaire could be useful to get a comprehensive overview of the different indicators and aspects employed to assess the intended construct. At practical level, it could be useful in clinical and research contexts to help tool users during the choice and assessment processes.
The present research, developed in two studies, had the following specific aims:
- To conduct a scoping review on available questionnaires for evaluation of AA and to analyze their contents (Study I). A scoping review is useful to identify potential size of available evidence and knowledge gaps, also involving ongoing research (Grant and Booth 2009; Mak and Thomas 2022). In particular, the Study I is focused on reporting the following information regarding each questionnaire: (a) content areas investigated and their adaptation to the AA determinants (WHO 2002; International Longevity Centre 2015), that is, physical, social, economic, cognitive, psychological/emotional, ecological and cultural areas and the related items/indicators, (b) main aims of the studies introducing the questionnaire and, (c) available validation information in any possible language and cultural context.
- Based on results obtained from Study I, Study II performed a detailed content validity evaluation of a specific AA questionnaire deemed most complete based on number of covered areas (Almanasreh et al., 2019), number of available validation information and translations into different languages.
Study I—Scoping review on measurement tools for the assessment of active aging
The aim of Study I was to conduct a scoping review to identify available questionnaires for evaluation of AA and to analyze respective assessed aspects.
Methods
Eligibility criteria This scoping review was conducted in according to The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR; Tricco et al. 2018). PRISMA-ScR enables methodological quality to the study providing a checklist and flow chart to describe steps of source selection (Tricco et al. 2018).
The inclusion criteria were the following: (a) documents written in English, (b) articles published in journals and (c) gray literature. Gray literature also refers to studies that do not report significant findings and therefore are often not published in scientific journals (Paez 2017). For these reasons, gray literature is an important resource for literature reviews because it may reduce publication bias, and it may a more complete framework of evidence (Paez 2017; Haddaway and Bayliss 2015). Since the construct of AA was coined in 2002 (WHO 2002), (d) documents written from 2002 to 2025 were selected. We included (e) studies that presented a questionnaire for measuring AA for the first time. Additionally, (f) studies with adaptations and/or validations of the questionnaires in other languages were also specified. Exclusion criteria: secondary studies and documents not written in English were excluded.
Search session The search session was conducted on September 3rd, 2025. Scopus, Web of Sciences (WoS), PsycINFO, and PubMed databases were used to select eligible studies. Scopus and WoS include multidisciplinary coverage (Archambault et al. 2009). PsycINFO covers behavioral science and mental health areas, while PubMed collects documents of biomedicine and health literature (Goossen 2020). Since databases such as Scopus and WoS contain more articles published in journals (Mongeon and Paul-Hus 2016), Bielefeld Academic Search Engine (BASE) and OpenGrey databases were used for the search of gray literature. The search strategy was defined using the following query based on title, abstract and keywords of papers: “active aging” OR “active ageing” AND “measur*” OR “measurement tool*” OR “scale” OR “test*” OR “questionnaire*”. Queries modified and adapted for each database are presented in Supplementary materials (Supplementary Tables S1, S2). Other studies were found by the inspection of the reference lists of the selected papers.
Data extraction and article selection From the selected records, duplicates were removed. Selected documents were screened for eligibility in two specific steps. In the first step, documents were assessed by title, abstract, and keywords to verify that they met the inclusion and exclusion criteria, i.e., proposal of a new questionnaire for active aging evaluation/validation of an existing questionnaire in another language. In the second step, full texts were analyzed for a further check following the aforementioned inclusion and exclusion criteria. For each included document, the following information was extracted: year, Country and language, sample age, study design (e.g., cross-sectional or longitudinal), investigated content areas, and aim of the questionnaire. The process of article selection was conducted by two independent raters (RN and GS). Additionally, a third independent rater (AL) was involved to solve disagreements, and the final decision was based on consensus among the three reviewers. A total of 25 documents were included in the final sample. In Fig. 1, the process for the inclusion of studies in accordance with the eligibility criteria is shown.Fig. 1. Flowchart of source selection
Results
Summary of findings
Table 1 shows information of each included study, i.e., year of publication, Country, sample, and study design. Among them, 21 studies proposed a new questionnaire, and the remaining four were translation and adaptation studies. Table 2 shows main characteristics of each included questionnaire. Table 1. Main characteristics of included studiesQuestionnaire/YearCountrySample ageStudy designActive Aging Awareness Questionnaire (AAAQ)Ahmad Bahuri et al. (2021)MalaysiaThree different samples, mean age (49.40; 49.90; 50.19)LongitudinalActive Aging Well-Being Index (AA-WB)Fritzell et al. (2021)Sweden > 60 yearsData from national surveysSelf-Aging Index (SAI)Gonçalves et al. (2017)Portugal ≥ 55 yearsData from a national survey (Study of the Aging Profiles of the Portuguese Population, EPEPP)and a cross-national panel dataset (Survey of Health, Aging and Retirement in Europe, SHARE)AAI—BangladeshHaque and Afrin (2022)Bangladesh ≥ 60 yearsCross-sectionalActive Aging Scale for Thai Adults (AAS—Thai)Thanakwang et al. (2014)Thailand ≥ 60 yearsLongitudinalVietnamese Active Aging Index (VAAI)Pham et al. (2020)Vietnam ≥ 55 yearsLongitudinalMarsillas et al. (2017)Spain ≥ 60 yearsCross-sectionalOliveira and Tavares (2020)Brazil ≥ 60 yearsCross-sectionalPaúl et al. (2012)Portugal ≥ 55 yearsData from national surveysMorales Ortiz and Fernandez (2020)Spain ≥ 48 yearsCross-sectionalda Silva Sousa and De Azevedo Barros (2020)Brazil ≥ 60 yearsCross-sectionalTaiwan Active Aging Index (TAAI)Hsu et al. (2019)Taiwan ≥ 55 yearsCross-sectionalYilmaz et al. (2023)Turkey > 60 yearsCross-sectionalSelf-Active Aging Index (S-AAI) Keeratisiroj et al. (2023)Thailand ≥ 60 yearsData from national surveysPunyakaew et al. (2023)Thailand ≥ 60 yearsLongitudinalIndividual Active Aging Index for European Countries(AAI- EU)Barslund et al. (2017)13 European Countries ≥ 55 yearsData from a cross-national panel dataset (Survey of Health, Aging and Retirement in Europe, SHARE)The University of Jyvaskyla Active Aging Scale (UJACAS)Rantanen et al. (2019)Finland ≥ 60 yearsLongitudinalBuys and Miller (2012)Australia ≥ 50 yearsCross-sectionalActive Community Asiamah et al. (2020)Ghana ≥ 60 yearsCross-sectionalHaque et al. (2016)Thailand ≥ 60 yearsData from national surveysActive Aging Scale—Urdu language (AAS-Pak)Bibi et al. (2023)Pakistan ≥ 60 yearsLongitudinalUniversity of Jyvaskyla Active Aging Scale (UJACAS)—Sweden languageNordeström et al. (2024)Sweden ≥ 55 yearsLongitudinalUniversity of Jyvaskyla Active Aging Scale (UJACAS) –Turkey languageErbil and Hazer (2019)Turkey ≥ 60 yearsLongitudinalUniversity of Jyvaskyla Active Aging Scale (UJACAS)–German languageHinrichs et al. (2024)Switzerland ≥ 65 yearsLongitudinalMarsillas et al. (2025)Spain ≥ 60 yearsCross-sectionalTable 2Main characteristics of included questionnairesQuestionnaireOriginal languageTerm referring to the assessed aspects of AACovered content areas and related itemsAimOther validationPhysicalPsychologicalEconomicSocialCognitiveCulturalEcologicalActive Aging Awareness Questionnaire (AAAQ)Ahmad Bahuri et al. (2021)Malay/––––1, 3:Awareness of specific elements of AA:4: free from chronic disease6: free from disabilities7: regular exercise9: healthy food10: no alcoholic beverages11: good oral health12: healthy minds14: not feeling lonely16: participation in voluntary activities17: participation in social activities20: hobbies21: learning new things22: good amount of saving for retirement23: own house––Monitoringawareness regarding AA in middle-aged people/Active Aging Well-Being Index (AA-WB)Fritzell et al. (2021)SwedishDomains2.2: Physical activities 3.1: Mobility3.2: able to perform ADL 3.4: Self-rated health3.5: Life-expectancy at 75. 4.1:Access to health care4.2:Access to dental care3.3: Mental health1.1: Cash-margin1.2: No financial difficulties1.3: Not at risk-of-poverty2.1: Cultural and leisure activities5.1: Cohabiting5.2: Family contacts5.3: Social contacts6.1: Care for older people6.2: Political participation6.3: Activity in organization6.5: Reading newspapers2.1:Cultural and leisure activities-Comparing levels of AA to detect inequalities and changes over the time in oldest old/Self-Aging Index (SAI) Gonçalves et al. (2017)PortugueseDomainsComplaints about health statusBMIWaist measureFalls (number, moment, cause, sequelae)Mobility (indoor, outdoor, climbing stairs)ADL e IADLExercise (walk and sport)SmokingComplaints about emotional statusFeeling of dismay/hopelessness Lack of interestFeelingnervousness/anxiousnessSleep problemsLack of energyActual jobSocial networkMarital statusHousehold sizeTime alone in 24 h periodConfiding with someoneSpatial and time awarenessGardening and****Housekeeping–Gardening and****HousekeepingProviding a self-assessment of AA status for older people/Active Aging Index (AAI)—BangladeshHaque and Afrin (2022)EnglishDimensions111–114: Sleep quality, walk, diet201: Self-related health status203: Disability204: Treatment of disease204(1): Regular medications204(2–3): Local accessibility to health care205: ADL206: IADL207: Alcohol drinking, smoking302: Help in activities120: Satisfaction with life202: Self-related mental health304: Satisfaction with family services407: Fear to be alone in house110: Family income115–116: Access to ICT119: Elderly friendly house401: Income402: Monthly income403: Source of income405: Home ownership406: Elderly friendly housing environment103: Marital status104: Head of household302: Help in activities303: Engagement in social activities105: Education115–116: Access to ICT118: Decision making501–514: Perception about AA117:Watching TV,listening to radio,reading newspaper117:**Watching TV,Listening to radio,reading newspaper–Monitoring QoL in older people/Active Aging Scale for Thai Adults (AAS—Thai) Thanakwang et al. (2014)ThaiFactors1: Being self-reliant5: Healthy lifestyle3: Spiritual wisdom4: Financial security2:Engagement with society7:Strengthening family ties to ensurecare6: Engagement in active learning6:Engagement in active learning–Assessmentof AA levelsBibi et al., (2023)—Language: UrduVietnamese Active Aging Index (VAAI) Pham et al. 2020VietnameseDomains–WELL-BEING wb1: Happy or good moodwb2: Peaceful and relaxedwb3: Full of energywb4: Feeling fresh and restedwb5: Daily life filled with things that interest meBASIC NEEDS:mdprv3: Buy meat frequently mdprv2: Unexpected expense mdprv1:Utility billINTERMNEEDSmdprv4: Traveling ortourismmdprv5: TVmdprv6: FridgeHIGH NEEDS:mdprv8: Washing machine mdprv7: Air conditionermdprv9: MotorbikeVOLUNTARY ACTIVITIES vol1: Community and society services,vol2: Cultural, educational, sport, occupational organizations, vol3: Charity activities,vol4: Human rights, environment–vol2: Cultural, educational, sport, occupational organizations,–Measuring and tracking AA levels/Marsillas et al. (2017)SpanishDimensionsPHY1: walk/ridePHY2: sport/exerciseOH1: median symptoms (two weeks)OH2: chronic diseasesSH1: performance ADLSH3: self-perceived healthF2: ADL/IADL (Mahoney and Barthel 1965; Lawton and Brody 1969)**Art1: singing and playing instrumentsArt2: craftingProd2: cookingOH3: psychological distress (three months)SL1: doing desirable thingsSL2: happiness to count on othersSL3: feeling of energy last weekSL4: feeling of confidence about future last weekG1: stimulation in anything last weekG2: satisfaction for achievement anything last weekEmo1: having fun last weekEmo2: feeling of happiness last weekEmo3: feeling of euphoria last weekSWL1: satisfaction related to ideal of lifeSWL2: conditions of lifeSWL3: satisfaction with lifeSWL4: obtaining important thingsSWL5: no changes in lifeEC3: expression of feelingsAC3: being positive and learning from difficult situationsAC4: taking difficult situations with humorSol1: spending time to be alone****Sol2: hobbiesE1: paid work (last week)ICT1: using phoneICT2: using computerICT3: using internetSol2: hobbiesOut1: going theaterOut2: travelingRecr1: watching TVSP1: care children/grandchildrenSP2: care older people/disableSP3: unpaid voluntary activities (12 months)SP4: political activities (12 months)SA1: play cards with others (six months)SA2: visit others (six months)SA3: religious activity (six months)Soc1: meeting friendsSoc2: receiving visitsSoc3: counting on othersSoc4: talking with someoneSoc5: going out with peopleEC1: obtaining affect from othersEC2: obtaining help from othersOut3: being member of associationEC3: expression of feelingsSoc6: receiving helpSoc7: receiving love and affectSoc8: receiving love from familyOut1: going theaterLL1: going to lectures in the last six monthsLL2: going to seminaries, courses****LL3: reading books and newspapersSH2: memory and attention affectionCog1: MEC-30 Lobo et al. (1999)AC1: changing situationsAC2: solving problemsAC3: being positive and learning from difficult situationsArt1: singing and playing instrumentsArt2: craftingICT1: using phoneICT2: using computerICT3: using internet****Prod2: cookingRecr2: SudokuSol1: spending time to be aloneOut1: going theaterLL1: going to lectures in the last six monthsLL2: going to seminaries, coursesLL3: reading books and newspapers****Sol2: hobbiesProd1: gardeningEvaluation of different elements of AA at the individual level/Oliveira and Tavares (2020)Portuguese DeterminantsFunctioning of hearing, vision, taste, smell, touchMorbiditiesPhysical activityPhysical security and protectionChanges in health statusCurrent health statusSleep qualityAlcohol useSmokingVaccination statusFamily history of CNCDsAccess to health careLink with health servicesPreventive examinationsRoutine check-upPhysical environment (means of transport, home security)ResilienceDepression/emotionalPhysical environment (feeling safe)Monthly incomeEconomic conditionMoney to meet basic needsPhysical environment (means of transport, home security)Environment in the homeRetirements/PensionPaid workSocial networkSocial supportPersonal relationshipCommunity activitiesOut-of-school activitiesCognitive ability (MMSE, Bertolucci et al.1994)–Physical environment (climate, pollution)Assessment of AA determinants/Paúl et al. (2012)PortugueseDeterminantsPerforming ADL e IADLPulmonary function Strength Subjective healthIllnessSubjective physical activityVisionAuditionSmokingSleep problemsPsychological distress HappinessPersonality Optimism LonelinessLife satisfactionSleep problemsQuality of lifeIncomeSocial networkCognitive functioning (MMSE, Bertolucci et al. 1994)––Assessment of AA determinants/Morales Ortiz and Fernandez (2020)Spanish**/CraftingSpending time in hobbiesAutonomous management of finance Using computerSpending time in hobbiesGoing to theater, watching filmGoing out with friendsTaking part to discussionsTrying to learn new things Using computer Writing letters Listening to music Going to theater, watching film Crafting Taking classesSpending time in hobbiesGoing to theater, watching film****Taking classes–Assessment of cognitively stimulating activities/da Silva Sousa and De Azevedo Barros (2020) Portuguese/Physical activity during leisureWorshipPaid workTravelingUse of internetVoluntary work/associationSociocultural activitiesVisitsPersonal contactsAccess to regular and other coursesUse of internetSociocultural activitiesAccess to regular and other courses**–Assessment of engagement in activities/Taiwan Active Aging Index (TAAI)Hsu et al. (2019)ChineseDomains3.1: Physical activity3.2: Access to health and dental care3.3: Independent living3.7:Physical safety from violence3.9: Physical function independence3.12: Primary prevention care utilization3.13:Physical safety from injuries4.1–2:Life expectancy**4.7:Transportation accessibility4.8: Transportation convenience4.9: Barrier-free space3.11: No depressive symptoms4.3: Mental well-being1:Employment3.4:Relative median income3.5: No poverty risk3.6:No sever material deprivation3.14: Owning assets4.4:Use of ICT4.7:Transportation accessibility4.8:Transportation convenience4.9: Barrier-free space2.1: Voluntary activities2.2: Care children/grandchildren2.3: Care disabled families2.4: Political participation2.5:Other social group participation4.5: Social contact4.10: Social integration and social respect3.3: Independent living3.8: Lifelong learning3.10: No severe cognitive impairment4.4:Use of ICT3.8:Lifelong learning4.9:barrier-free space**Monitoring AA and defining AA policies/Yilmaz et al. (2023)TurkishDimensionsTaking long walks **Participating in sports activitiesGoing to concert/watching film/playing instrumentsRepairing tools–TravelingGoing to concert/watching film/playing instrumentsRepairing toolsTalking to friend/relativeson the phoneMeeting with friends/relativesVolunteering activitiesGoing to restaurants/cafes, etc.Participating to religious activities Participating in sports activitiesParticipating in hobby groupsGoing to concert/watching film/playing instrumentsRepairing toolsGoing to concert/watching film/playing instrumentsGardeningAssessment social participation in older people which living in urban and rural areas/Self-Active Aging Index (S-AAI) Keeratisiroj et al. (2023)ThaiFactorsHealth1: Physical healthHealth 2: VisualHealth3: HearingHealth 4: Barthel ADL (1965)Health 5: functional abilityHealth 6: Chronic diseasesHealth 9: sleep problemsHealth 11–12: oral careHealth 13: BMIHealth 14: physical activityHealth 15: smokingHealth 16: alcoholHealth17: Annual check-upHealth 7: Psychological distressHealth 8: No happinessHealth 9: Sleep problemsPar1: WorkingPar3: Financial support to familiesSec1: House ownershipSec2: Head of householdSec3: Residential safetySec5: Income levelSec6: Source of incomeSec7: Sufficiency of incomeSec8: Saving bathSec9: Debt bathPar2: Marital statusPar4: Member of groupPar5: Participationin activitiesPar6: Meeting neighborsHealth 10: Forgetfulness problem––Assessment AA in older people which leaving in rural areas/Punyakaew et al. (2023)ThaiComponentsH1: Chronic conditionH2: Pain and discomfortH3: Physical abilityH5: Physical health conditionS2: Live conditions and SecurityH4: Mental healthS1: Financial stabilityS2: Live conditions and SecurityE1: Use of ICTSP1: ReligionSP2: CommunitySP3: Family and friendsE1: Use of ICTE2: LiteracyE2: Literacy**–Assessment of AA levels/Individual Active Aging Index for European Countries(AAI- EU) Barslund et al. (2017)EnglishDomains3.1:Physical exercise3.2:Access to health and dental care3.3: Independent living arrangements3.7: Physical safety from crime4.1.-2:Remaining life expectancy4.3: Mental wellbeing1:Employment3.4:Relative median income3.5: No poverty risk for older person3.6: No severe material deprivation2.1: Voluntary activities2.2: Care children/grandchildren2.3:Care to older adults2.4: Political participation4.5: Social connectedness4.4: Use of ICT4.6: Educational attainment3.8: Lifelong learning****3.8: Lifelong learning–Comparing levels of AA to detect inequalities/The University of Jyvaskyla Active Aging Scale (UJACAS) Rantanen et al. (2019)FinnishSides1: crafting2: singing, playing instrument, drawing4: going out to nature5: physical exercise8:help and support people****14: improving coziness at home13: making days more interesting14: improving coziness at home15: taking care of appearance17: spirituality7: use of computer or iPad16. ensuring financial affairs1: crafting****3: events (study and club/association)****8: help and support people9:maintain social relationships10: meet new people12:taking responsibility to promote social and public questions****3: events (study and club/association)****2: singing, playing instrument, drawing6:exercise mind and memory7: use of computer or iPad11: taking responsibility to furthering life-related issues12:Taking responsibility to promote social and public questions****3: events (study and club/association)12:taking responsibility to promote social and public questions4: going out to natureAssessment of AA at individual levelErbil and Hazer, (2019),Language: TurkishNordeström et al. (2024),Language: Swedish Hinrichs et al. (2024),Language:GermanBuys and Miller (2012)EnglishDomainsF:Physical functioning, role limitations, bodily pain, general health, vitalityG: VisionH: Home and environment:****access, visibility, safety, usability, maintenance, comfortE: Emotional well-being,Emotional and mental healthD:Spiritual believesA: Paid and voluntary workH: Home and environment:****access, visibility, safety, usability, maintenance, comfortC:Social: subjective support and social interactionsB:Learning new things––Measuring the three pillars of AA: health, security, participation/Active Community Asiamah et al. (2020)EnglishFactorsHPS: health and paramedical servicesSas: sanitation and aesthetics****SDCI: safety and disability friendliness of commercial infrastructure–SDCI: safety and disability friendliness of commercial infrastructureSCOs: social centers and organizationsPRSN: public services and road network****SDCI: safety and disability friendliness of commercial infrastructure–SCOs: social centers and organizationsSas: sanitation and aestheticsPRSN: public services and road networkMonitoring the maturity of the built environment for social and physical activities/Haque et al. (2016)ThaiDeterminantsExerciseOral healthMedicationADLSubjective healthIllnessVisibilityHearingFallsSmokingAlcohol drinkingHealth promotion and disease prevention, Curative health services, Continuous care,Mental health careAnnual health check-upLocation of bed****Location of toiletHappiness levelPsychological distress statusWorkIncomeSufficiency of incomeSavingsLocation of bed****Location of toiletSocial support qualityMarital statusCommunity participationParticipate in elderly group–––Assessment of AA determinants and AA levels in older people/Marsillas et al. (2025)SpanishDimensionsIndependence in Basic Life Activities (ADL; Mahoney and Barthel 1965)Independence in Instrumental Life Activities (IADL; Lawton and Brody 1969)Presence of symptoms in the past two weeksAbsence/presence of chronic diseaseAbsence/presence of non-chronic disease or psychologicalstress in the past 3 monthsPerceived limitations in daily activitiesPerception of daily activity limited by cognitive stateSatisfaction with healthPerceived on health compared to peersSinging/playing instruments Drawing or craftsWalkingSports, exercise, or dancingGardeningCookingSatisfaction with relationship with neighborsSatisfaction with relationship with friendsSatisfaction with help from familySatisfaction with time spent with familyFeeling loved by familyFeeling things are going wellFeeling glad for having people to count onFeeling full of energyFeeling confident about the futureJoyCheer or happinessEuphoricInterest AchievementPaid workUse of mobile phoneUse of computerUse of the Internet****Cinema/Theater TravelingFrequency of contact with friends and familyVisitsHaving people who care about oneselfPossibility to talk to someone about problems Receiving invitations to entertain or going out Receiving help when being illReceiving love and affectionFeeling loved by familyCaring for children and grandchildren Political participationVolunteeringPlaying cards/other games with peopleVisiting friends/relatives/neighborsMini-examen cognoscitivo Lobo et al. (1999)Interest AchievementCaring for children and grandchildrenPolitical participation****VolunteeringUse of mobile phoneUse of computer. Use of the InternetReadingUse of mobile phone Use of computerUse of the Internet****Games: Crosswords, Sudoku, etcAttendance to lectures. Attendance to courses within/outside theregular education systemSinging/playing instruments Drawing or crafts****Cinema/Theater Traveling. Associations or clubsTV watchingCollect thingsGardeningEvaluation of AA at individual level/Note: - = content area not considered; / = validation studies not found; terms referring to assessed aspect of AA not specified; Items/indicators covering multiple areas are shown in boldAbbreviation: AA = Active Aging; ADL = Activities of Daily Living; IADL: Instrumental Activities of Daily Living; QoL = Quality of Life; ICT = Information and Communication Technology; CNCDs = Chronic Non-Communicable Disease(s)
The following important features are reported for each questionnaire:
- terms used to refer to the assessed aspects of AA (e.g., “determinants,” “components,” etc.);
- content areas (e.g., physical, psychological, social, etc.) covered by items and number of items of the questionnaire, if specified;
- asserted aims underlying the development of the questionnaire;
- available translation / validation in other languages.
The first finding regarded different referring to the assessed aspects. Particularly, six studies used the term “domains” (i.e., Buys and Miller 2012; Gonçalves et al. 2017; Barslund et al. 2017; Hsu et al. 2019; Pham et al. 2020; Fritzell et al. 2021); three studies used “determinants” (Haque et al. 2016; Paúl et al. 2012; Oliveira and Tavares 2020); three studies used “factors” (Thanakwang et al. 2014; Keeratisiroj et al. 2023; Asiamah et al. 2020); four studies used “dimensions” (Marsillas et al. 2017; Haque and Afrin 2022; Yilmaz et al. 2023; Marsillas et al. 2025), one study used “components” (Punyakaew et al. 2023), and one study used “sides” (Rantanen et al. 2019).
Furthermore, often the generic term “health” or “personal factors” encompasses physical and mental health (e.g., Fritzell et al. 2021; Oliveira and Tavares 2020; Paúl et al. 2012; Hsu et al. 2019; Keeratisiroj et al. 2023; Punyakaew et al. 2023; Barslund et al. 2017). Most of questionnaires contained 4 or more subscales, except for the Active Aging Awareness Questionnaire (AAAQ; Ahmad Bahuri et al. 2021), Active Community, and two questionnaires developed by da Silva Sousa and de Azevedo Barros (2020) and Morales Ortiz and Fernandez (2020) which were not divided in subscales. Given this heterogeneity, it was chosen to group aspects using the term “content areas” to clarify specific investigated aspects:
- Physical area includes activities promoting mobility and physical efficiency, physical exercise, autonomy in performing activities of daily living;
- Cognitive area includes activities promoting perception, attention, learning, memory, thinking, decision-making, problem solving and language;
- Psychological/emotional area includes activities that promote psychological well-being (e.g., prevention of depression, anxiety, lack of energy, feelings of loneliness);
- Ecological area includes activities promoting the enjoyment of natural environments;
- Cultural area regards the participation in cultural activities;
- Economic area includes activities promoting financial autonomy, financial security, (light) work activity;
- Social area regards the participation in community activities, received/provided social support, preservation of social relationships (family and friends).
Analyzing the content areas covered by items, the questionnaires by Marsillas et al. (2017, 2025), the University of Jyvaskyla Active Aging Scale (UJACAS; Rantanen et al. 2019) and the Taiwan Active Aging Index (TAAI; Hsu et al. 2019) included items measuring all areas. On the other side AAAQ (Ahmad Bahuri et al. 2021) focused only on cognitive area. Generally, physical, psychological, social, cognitive, and economic areas were included in almost all the questionnaires while ecological and cultural aspects were less frequently considered. Moreover, 12 studies specified number of items. The two shortest questionnaires were composed by 11 items (da Silva Sousa and de Azevedo Barros 2020; Morales Ortiz and Fernandez 2020). On the contrary, one questionnaire had 177 items (Buys and Miller 2012) and the questionnaire UJACAS had 17 items for 4 subscales (that is, the same 17 content areas evaluated on four different aspects).
Regarding the aims of included studies, most of questionnaires aimed to assess levels of AA and the respective determinants. Particularly, three studies (Paúl et al. 2012; Oliveira and Tavares 2020; Haque et al., 2016) developed a new protocol for evaluation of AA determinants adapted from by other scales. Three questionnaires aimed to evaluate AA at individual level (Rantanen et al., 2019; Marsillas et al., 2017, 2025). On the other hand, AAAQ (Ahmad Bahuri et al. 2021) aimed to monitor awareness about AA, Activity Community (Asiamah et al. 2020) was developed to measure effective community characteristics to ensure social participation. The AAI for European Countries and AA-WB aimed to analyze inequalities of AA in older people (Barslund et al. 2017; Fritzell et al. 2021). The questionnaire of Morales Ortiz and Fernandez (2020) focused specifically on evaluation of cognitively stimulating activities and Self-Active Aging Index (S-AAI; Keeratisiroj et al. 2023) focused on older people living in rural areas.
In conclusion, only the Active Aging scale for Thai Adults (AAS-Thai; Thanakwang et al. 2014) and UJACAS (Rantanen et al. 2019) were validated and translated in other languages. Specifically, Bibi et al. (2023) validated the AAS-Thai in Urdu language and UJACAS were validated in Sweden, Turkish and German (Nordeström et al. 2024; Erbil and Hazer 2019; Hinrichs et al. 2024).
Study II—Content validity evaluation of the University of Jyvaskyla Active Aging Scale (UJACAS)
The aim of Study II was to conduct a content validity evaluation of a chosen questionnaire for evaluation of AA. This could be useful to obtain a complete framework of evaluated aspects by a specific questionnaire and to ensure a greater dissemination for exhaustive evaluation of the construct.
Based on results by Study I, the UJACAS scale (Rantanen et al. 2019) was chosen for content validity evaluation in according to the following reasons:
- The scale covered all content areas. Consequently, this scale could detect the different aspects related to AA construct.
- Since this scale has a vast but not disproportionate number of items, it is reasonable to assume that UJACAS has the potential to assess appropriately aspects related to AA without increasing too much the burden on respondents. Additionally, it is possible to administer the scale as a questionnaire or an interview, this dual option allows the scale to be tailored to the needs of the respondent and/or the aim of the evaluator.
- To our knowledge, this scale was validated and translated in another three languages other than Finnish, of the Western European area i.e., Swedish, Turkish and German (Nordeström et al. 2024; Erbil and Hazer 2019; Hinrichs et al., 2024). Only another scale AAS—Thai (Thanakwang et al. 2014) was translated into another language (i.e., Urdu), and no other validation studies were found for the remaining questionnaires. A greater number of translations of an instrument could ensure cross-cultural comparisons (Bujang et al. 2022).
The UJACAS questionnaire is composed by 17 items corresponding to activities still carried out, usually, at a later age (e.g., social, physical, leisure, and cultural activities; management of finances and daily affairs; use of technological devices). Each item is developed into 4 subscales corresponding to the following questions:
- Goal: “During the previous four weeks, I have wanted to…”. This subscale refers to how strong was the desire to carry out activity.
- Ability: “During the previous four weeks, I have or would have been able to…”. This subscale refers to refers to how well the respondent was able to perform activity, based on health status and functional abilities (i.e., physical and mental abilities).
- Autonomy: “During the previous four weeks, my opportunity to…”. This subscale refers to the opportunity to carry out activity, considering matters related to life and environment.
- Activity: “During the previous four weeks, I did…”. Activity refers to the frequency of performing.
According to the authors, the four subscales reflect four central sides of AA, and each activity is assessed for the four sides. It was demonstrated that the questionnaire was able to assess a unidimensional latent construct of AA (Rantanen et al. 2019).
The total score ranges from 0 to 272 with higher scores indicating higher levels of AA.
Response scale selected is a 5 point Likert-like scale from 0 to 4. Response options range:
- from “not at all” to “very strongly” for the subscale Goal;
- from “not even with help” to “without any difficulties” for the subscale Ability;
- from “It has not been possible” to “very good” for the subscale Autonomy;
- from “not at all” to “daily or almost daily” for the subscale Activity.
According to the authors, the scale has good validity, reliability, and a test–retest reliability.
Methods
Eight experts were identified among academics and scientists with expertise in the assessment of healthy and pathological aging. Literature suggested to use from five to ten raters to decrease probability of casual agreement (Almanasreh et al. 2019). In more detail, the experts were external to the research group and were selected according to two criteria: they were either PhD candidates or had a PhD in Psychometrics. All the experts gave their consent before proceeding. For each rater, an information kit and a response form (with items set at random) will be presented.
For each item, the asked question was “to which content areas do the activity listed in the item refer?”. Options were:
- 0 if the item does not refer to content area,
- 1 if the item does refer to content area.
It was also clarified that more than one content area can be indicated if the item was considered to cover more than one. The sums of the scores provided by the evaluators for each item and content area were calculated. To verify whether the items encompassed and assessed one or more content areas, the content areas that reported the first and second highest scores were identified. Subsequently, the ratio of the first and second highest scores was calculated. The term “content validity evaluation” was chosen to differ from the content validity analysis (e.g., Lawshe, 1975). Content validity analysis provides evidence that the components of an assessment are both relevant to and representative of the construct they are designed to measure (Almanasreh et al., 2019). In this case, we wanted to analyze how much each item on the UJACAS scale could cover one or more specific content areas identified for Study I.
Results
Table 3 shows the sum scores for all eight raters. Specifically, each row corresponds to the sum scores for each item, while each column refers to the sum scores for each content area. The last column of the table shows the calculated ratio between the first and second highest scores related to content areas. The ratio scores allow us to analyze the extent to which each item covers one or more content areas. A ratio score of 2 or greater suggests that the item primarily addresses a single content area, corresponding to the content area that received the highest score. Conversely, a ratio score below 2 indicates that the item may encompass multiple content areas, corresponding to the content area that reported the first and the second highest scores. Table 3. Sum scores of items and content areas of University of Jyvaskyla Active Aging Scale (UJACAS) based on eight ratersContent areasitem abbreviationphysicaleconomicsocialpsychological/emotionalcognitiveecologicalculturalratio1_crafting71025011.42_artistic pursuit32046031.53_events217321714_nature60142801.35_exercise801211046_cognitive training0000800/7_technology211160238_help others61862001.39_maintain relationships10851101.610_meet new people00852001.611_promote own matters52075001.412_societal activity00742151.413_make days interesting02073032.314_make home cozy01272103.515_appearance33251011.716_economic balance0800400217_spirituality11642351.2Note: the items abbreviations referred to the University of Jyvaskyla Active Aging Scale. The content areas were physical, economic, social, psychological/emotional, cognitive, ecological, and cultural. The numerical values represent the total number of raters who assigned a particular item to a specific content area. For example, if five raters considered item 1 “crafting” pertained to the cognitive area, the score in that cell corresponds to 5. The last column reported the ratio between the highest and second-highest scores for each item. For example, the ratio for item 1 was 1.4 (corresponding to 7 divided by 5). In this case, the ratio was below 2, indicating that item 1 may encompass multiple content areas (i.e., physical and cognitive areas)
Overall, only item 6 (“cognitive training”) did not report ratio value because covered the cognitive area.
Ten items reported a ratio value less than 2. This indicates that the items could exhaustively cover more than one content area.
In particular, the cognitive area was covered by item 1 (“crafting”), item 2 (“artistic pursuit”), item 11 (“promote own matters”). The physical area was covered by item 1, item 4 (“nature”), item 8 (“help others"), item 11, and item 15 (“appearance”). The social area was covered by item 3 (“events), item 8, item 9 (“maintain relationships”), item 10 (“meet new people”), item 12 (“societal activity”) and item 17 (“spirituality”). Items 3, 12 and 17 covered also the cultural area. The psychological/emotional was covered by items 2, 8, 9, 10, 11, and 15. The economic area was covered by item 15 while the ecological area was covered only by item 4.
In conclusion, the remaining items reported a ratio greater than 2. This indicates that these items covered mainly one content area.
Item 7 (“technology”) and item 14 (“make home cozy”) covered the cognitive area while item 5 (“exercise”) covered the physical area. Item 16 (“economic balance”) covered the economic area and item 13 (“make days interesting”) covered the psychological/emotional area.
General discussion
The general aim of the present studies was to identify existing questionnaires for the evaluation of AA to help health experts to choose faster the suitable questionnaire related to aim and to the aspects to be assessed. To realize this, a scoping review was conducted to identify existing questionnaires for the evaluation of active aging (AA) and to describe the characteristics related to assessed aspects, main aim and validations in other languages (Study I). Based on results obtained by Study I, a deepened content validity evaluation of the University of Jyvaskyla Active Aging Scale (UJACAS) was conducted to have a comprehensive framework of investigated aspects (Study II).
Study I
In the present scoping review, 25 studies published between 2002 and 2025 were included. Main findings highlighted that the questionnaires are quite different in terms of covered areas by items and terms used to describe investigated aspects. Furthermore, it is worth mentioning that few studies presented validation in other languages of existing questionnaires.
At first, although most of the questionnaires were developed after 2015, only one study considered all four pillars of AA—security, participation, health, and lifelong learning—(da Silva Sousa and de Azevedo Barros 2020). Probably, authors referred to the AA model of the WHO (WHO 2002), rather than the expanded model that added lifelong learning as the fourth pillar (International Longevity Centre 2015). The addition of lifelong learning supports the other three pillars and underlines that learning plays an important role in improving well-being and quality of life in older people (Findsen and Formosa 2016). Future studies should refer to the updated model, considering all four pillars for validating new questionnaires.
Furthermore, while social, physical, psychological, cognitive and economic aspects were often considered in the AA evaluation process, ecological and cultural aspects were often overlooked. This could cause a loss of important information, since ecological and cultural aspects can significantly affect a successful and active aging. In the previous studies, it was demonstrated that green space accessibility predicted well-being and promoted physical and outdoor activities, social relationships, and participation in community (Lak et al. 2021; Zeng and Yang 2019; Sánchez-González and Egea-Jiménez 2021; Ricciardi et al. 2023; Spano et al. 2023). In this sense, green space accessibility becomes a resource to strengthen the four pillars of active aging.
Regarding cultural aspects, performing cultural activities (e.g., study groups) was related to a higher quality of life and satisfaction with health in older people (Koponen et al. 2023). Furthermore, the accessibility of cultural environments (e.g., exhibitions and museums) provides older individuals with the opportunity to engage in lifelong learning, which is the fourth pillar of AA. For these reasons, supporting cultural activities is important to support active aging policies (Hernández Lara and Toney 2021). Based on this evidence, the development of new questionnaires should insert items or indicators related to ecological aspects to analyze their influence on physical activities, social participation and perceived well-being.
Another important aspect concerns different terms used to present content areas. The terms “components”, “determinants”, “dimensions”, and “domains” are often used interchangeably.
The term “domains” often suggests broad, primary categories that encompass various aspects of a complex concept. In the context of AA, “domains” may refer to major areas of life (e.g., physical health, social engagement, psychological well-being) that collectively contribute to an individual's experience of aging. The use of “domains” implies a structured framework where each domain represents a distinct, yet interconnected, aspect of active aging. It reflects a comprehensive approach, treating each domain as integral to the whole. The use of “determinants” suggests a focus on the underlying factors or variables that influence AA outcomes. These are likely seen as causal agents or key drivers that shape how individuals age actively. Studies using “determinants” may emphasize the cause-effect relationships, such as socioeconomic factors, health behaviors, or environmental conditions that impact active aging. This term implies a more analytical or explanatory approach, concentrating on identifying and addressing root causes. “Components” implies a more modular or building-block approach, where different parts contribute to the whole. In AA, “components” might be specific elements (e.g., mobility, social participation, cognitive function) that together form the complete construct of active aging. The use of this term suggests that these elements can be individually analyzed or modified without necessarily altering the overall structure of active aging. It conveys a view of AA as an assembly of smaller, interdependent parts. The term “dimensions,” the most general one, suggests a multi-faceted, often qualitative view of AA, where different perspectives or axes of experience are considered. In the context of AA, “dimensions” might refer to different angles from which the aging process is examined, such as the subjective (e.g., self-perceived health), objective (e.g., functional abilities), or relational (e.g., social interactions) aspects. The use of “dimensions” indicates a flexible, layered understanding of AA, where each dimension adds depth and complexity to the overall concept.
These terms reflect differing theoretical perspectives and emphases—ranging from holistic and causal approaches to modular and multi-dimensional views of active aging.
This heterogeneity in used terms can reflect a lack of clarity in the AA theory. The model developed by WHO (2002) did not specify the difference between determinants and components of AA. Particularly, determinants such as financial security/economic factors and health were often defined as components, causing lack of clarity (Boudiny 2013). According to Boudiny (2013), the term “component” should be used to refer to an essential part of AA. On the other hand, health and financial security should be considered as instrumental resources to perform certain activities, rather than AA itself (e.g., economic finances and physical abilities might help to perform certain activities such as leisure or physical activities). Therefore, these aspects should be considered as determinants that can promote or hinder AA and not as components of AA (Boudiny 2013). However, there is still uncertainty about what the components of AA are and how to evaluate the construct (Belanger et al. 2017). Given this conceptual heterogeneity, highlighting the meanings of the different terms is important. On a practical level, clarifying these definitions can also provide benefits for professionals in clinical settings. Recognizing the specific function of each term could help professionals in selecting assessment tools with greater precision. For example, professionals might choose to evaluate a specific component (e.g., social participation) using a specific questionnaire, while evaluating a determinant (e.g., economic resources) with a different questionnaire, while recognizing heterogeneity and different meanings of the terms. This selective and tailored approach allows a personalized and refined assessment of the AA construct.
Five studies proposed new questionnaires for evaluation of AA adapted by other scales (Marsillas et al. 2017, 2025; Paúl et al. 2012; Buys and Miller 2012; Oliveira and Tavares 2020). Since the development of a new questionnaire requires rigorous steps, adapting instruments is a common process (Sousa et al. 2017). Given the multiplicity of questionnaires available, adapting existing questionnaires preserving their conceptual equivalence could be useful to reduce time and cost demanding actions (Hall et al. 2018; Sousa et al. 2017).
On the same line, we acknowledge that only two questionnaires (The University of Jyvaskyla Active Aging Scale, UJACAS; Rantanen et al. 2019; The Active Aging Scale for Thai Adults, AAS-Thai; Thanakwang et al. (2014) had validations in multiple languages. This represents a limitation in terms of study replication, comparative studies, and dissemination of the questionnaires. Adaptation and translation of questionnaires is an essential process to use them in new cultural and linguistic contexts (Gjersing et al. 2010). Moreover, cross-cultural adaptation of questionnaires is an important process to reduce risk of bias (Herdman et al. 1998) and allows a fair comparison between cultures of the same indicators (Bujang et al. 2022). For these reasons, future validations in other languages could be useful to ensure greater applicability of questionnaires. However, since most of the questionnaires were developed in 2020, it is reasonable to assume that the development of questionnaires and their respective validation studies in other languages is still at an early stage.
Study II
Content validity evaluation was conducted identifying eight academics and scientists with expertise in the assessment of healthy and pathological aging. Particularly, it was calculated a ratio value to detect the coverage of content areas by each item.
At first, social relations and participation (i.e., items 3, 8, 9, 10) could encompass different factors in line with the literature. Previous evidence reported that enacted social support and participation in activities with formal support predicted life satisfaction and positive affect (Siedlecki et al. 2014; Blace 2012). Also, participation in activities with social support (e.g., assistance activities, carrying out errands for others) requires physical abilities (Blace 2012). Participation in cultural and social activities (e.g., taking part in art classes, going to theater), social support networks, and social integration, are associated with greater life satisfaction, positive affect, and affective balance (Reyes-Martínez et al. 2021). Cultural activities in older people are important to reduce stress and anxiety and to improve self-esteem (Murtin and Zanobetti 2024).
Regarding physical activity (i.e., item 5), psychological and emotional aspects are not dominant factors. This was explained in previous studies. Exercise has been shown in the literature to lead to improved well-being and life satisfaction, and physical activity could be considered a protective factor against depression (Ryu and Heo 2017; Kadariya et al. 2019). However, considering the intensity level of physical activity, a previous study showed that light physical activity (bowling, archery, electric trolley golf, fishing) was associated with life satisfaction and physical health, while moderate physical activity (e.g., light tennis, slow or light swimming, low-impact aerobics) was associated with physical health but not life satisfaction (Bae et al. 2017). For these reasons, although exercise may be associated with psychological well-being, this relationship is not always shown and may depend on the intensity of the exercise.
Moreover, leisure activities such as crafting and artistic pursuit (i.e., items 1, 2) could include the different aspects such as cognitive functioning and perceived well-being. In this regard, it was demonstrated that leisure activities predicted higher cognitive functioning and that cognitive functioning in turn predicted participation in leisure activities (Lifshitz-Vahav et al. 2017). Particularly, musical activity (e.g., dancing, playing instruments, and singing) is an important resource to promote well-being and cognitive health in older people (Dingle et al. 2021) and crafting activity , frequently performed in the elderly, enhances physical and mental health (Chacur et al. 2022).
Going outside and enjoying nature (i.e., item 4) could include aspects related to physical abilities and ecological characteristics in line with previous studies. Physical performance is an essential prerequisite to perform outdoor activities (Portegijs et al. 2014). On the other hand, it was shown that ecological characteristics (e.g., quality of air and near green space) could encourage older people to perform activities in natural environments (Yu et al. 2021).
Furthermore, using technology (i.e., item 7) comprises mainly cognitive aspects. In this regard, previous studies reported that problem solving ability, episodic memory and executive functioning were associated with technology devices (e.g., phone, computer, Internet) (Charness and Boot 2009; Choi et al. 2021). Other predictors were cultural knowledge and education. However, changes related to age in visual acuity (e.g., susceptibility to lightness) and in motor efficiency (e.g., arthritis) could hinder technology use. Considering this, although the utilization of technology is predominantly reliant on cognitive abilities, physical limitations may potentially obstruct the utilization.
In conclusion, the two items referred to activities to be performed independently (i.e., items 11, 16), include coherent aspects in according to the literature. Promoting own matters requires self-management abilities (e.g., positive affect, self-efficacy, taking initiative, investing in resources to obtain long-term benefits) which mediate the relationship between cognitive, physical functioning and well-being (Steverink et al. 2005; Cramm et al. 2013). Moreover, adequate cognitive and physical functioning ensure the maintenance of self-management abilities to preserve well-being (Cramm et al. 2013). Regarding financial balance, it was demonstrated that cognitive functioning and financial literacy may influence financial behaviors in older people (Kim et al. 2018). Particularly, worse cognitive abilities are associated with reduced self-efficacy which, in turn, decrease financial management ability (Tang 2021). Therefore, cognitive ability could be an important aspect of economic balance.
Limitations
This work has limitations. The cross-sectional design adopted for many studies does not allow analysis of the test–retest reliability of the questionnaires. Another potential limitation may arise from the fact that only studies that had proposed the questionnaire considering a sample of older people were included. For this reason, some studies proposing a questionnaire for evaluation of AA may have been excluded.
On the other side, we believe that the greatest advantage of this work is represented by the practical potential for users of the questionnaires, both in clinical and research contexts.
Very frequently, the presence of different questionnaires for AA assessment and heterogeneous indicators could lead to confusion about the most appropriate questionnaire to use. Our work provides a valuable perspective for making informed and personalized choices when selecting a questionnaire. By identifying the areas each questionnaire covers and their respective validations in other languages, we offer a useful resource for evaluators, helping to streamline both the selection and evaluation process. Additionally, a targeted selection of questionnaires tailored to the evaluators' objectives would help reduce the burden on respondents.
Conclusion
This work offers potentially valuable insights into the existing questionnaires for measuring AA, providing a practical resource for health experts. By identifying the specific content areas covered by each questionnaire and their validation status in different languages, this work aids in the informed selection of questionnaires, potentially reducing the time and burden associated with the evaluation process. Selected questionnaires are different in investigated aspects and each study uses different terms to describe these aspects: domains might be seen as broad, predefined categories for organizing knowledge about AA, determinants focus on causality, with an emphasis on factors that shape the process of active aging, components refer to individual elements that together constitute AA, suggesting a modular structure, dimensions represent various perspectives or axes of AA, offering a multi-faceted view of the concept. This suggests a potential confusion between what fundamentally constitutes AA and what factors influence it, likely stemming from a lack of conceptual clarity. Finally, this research could help aging care professionals toward a focused and informed selection of questionnaires according to their evaluation needs. Moreover, given that UJACAS scale covers the largest number of aspects related to active aging and is the most widely translated questionnaire in other languages, future validation studies could ensure greater diffusion of this questionnaire for an exhaustive assessment of active aging.
Future efforts should focus on enhancing the clarity of AA models, integrating ecological factors, and expanding the validation of questionnaires across various languages and cultures.
Conflict of interests
The authors declare no competing interests.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 22 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bertolucci PH, Brucki SM, Campacci SR, Juliano Y (1994) O Mini-Exame do Estado Mental em uma população geral. Impacto da escolaridade [The Mini-Mental State Examination in a general population: impact of educational status]. Arquivos de neuro-psiquiatria, 52(1): 1–78002795 · pubmed ↗