Allergic Contact Dermatitis to 1.6‐Hexanediol Diacrylate in Ski Boots
Nadia Raison‐Peyron, Alison Poncy, Jakob Dahlin, Cecilia Svedman

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
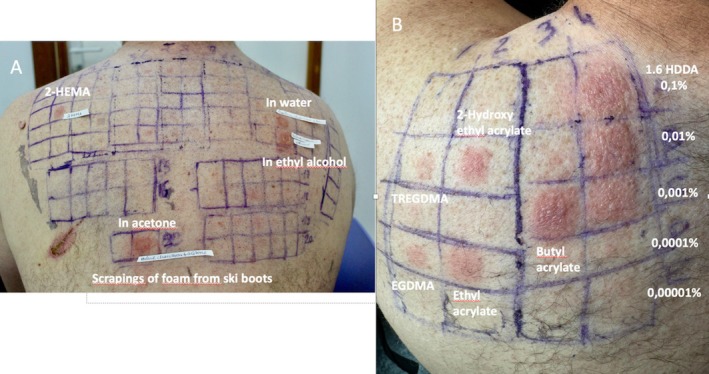 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsContact Dermatitis and Allergies · Surgical Sutures and Adhesives · Occupational exposure and asthma
We report the case of a 48‐year‐old male patient, a cutler by profession, referred for recurrent eczema on his lower limbs sparing the feet. His medical history included allergic rhinoconjunctivitis to grass, multiple sclerosis, sleep apnoea, and a previous but unspecified skin reaction to adhesive dressings.
On three separate occasions during downhill ski training, the patient developed a similar clinical presentation of erythematous, vesicular, pruritic lesions on his lower legs while wearing a new pair of thermoformed ski boots whose interior part was composed of foam covered with black fabric in contact with legs but not feet (Figure 1A–C). Prior to the episodes with eczema, the patient had worn the boots twice with no reaction.
Patch testing was carried out on the patient's back using IQ Ultra Chambers (Chemotechnique Diagnostics, Vellinge, Sweden), occluded for 2 days with Opertape (Iberhospitex, Innovative Health Technologies, Barcelona, Spain), and reading was performed on Day (D)2, D3, and D7 according to ESCD guidelines [1].
The baseline European series (Chemotechnique Diagnostics, Vellinge, Sweden) showed a single positive reaction to 2‐hydroxyethyl methacrylate (2‐HEMA) 2% in petrolatum (pet), ++ on D2 and D3. Ski boot foam scrapings (extracted using water, ethyl alcohol, and acetone) were also all strongly positive (+++) on D2 and D3 (Figure 2A). Conversely, the rubber and plastics/glues series, including acetophenone azine 1% pet, were all negative. Late readings on D7 revealed no further positive results.
A chemical analysis of the foam sample via gas chromatography–mass spectrometry performed in Sweden revealed a significant quantity of 1,6‐hexanediol diacrylate (1,6 HDDA). The concentration of 1,6‐HDDA in the ski‐boot foam scraping was about 350 ppm (0.035%). Subsequently, we therefore performed additional patch testing with an acrylates series and 1,6 HDDA 0.1% pet, using serial dilutions. 1,6 HDDA showed a strong positive reaction at the three highest concentrations (0.1%, 0.01%, and 0.001%). Other substances tested also elicited positive reactions, including triethylene glycol dimethacrylate (TREGMA) 2% pet, ethylene glycol dimethacrylate 2% pet (EGDMA), 2‐hydroxyethyl acrylate 0.1% pet, ethyl acrylate 0.1% pet, and butyl acrylate 0.1% pet (Figure 2B).
One year later, the patient skied again with the same ski boot shells, but with a different brand of new booties (still thermoformed). The dermatitis quickly relapsed on his lower legs. Then, he continued to ski, wrapping his lower legs in cellophane under socks, without any reaction.
Discussion
1
Rubber, biocides, dyes, acetophenone azine, and formaldehyde resins are commonly implicated in allergic contact dermatitis elicited by individual sports equipment [2, 3], while the main sources of acrylate exposure are typically found in nail care (e.g., artificial nails and semi‐permanent varnishes), dentistry (e.g., composite resins), adhesive dressings, glues, and printing inks [4, 5, 6].
2‐HEMA is usually considered a marker for allergy to methacrylates, with a high incidence of cross‐reactions to other methacrylates, which is the reason why it was included in the baseline European series in 2019 [6, 7]. 1,6 HDDA (CAS no. 13048‐33‐4) is a multifunctional acrylate and a potent sensitiser. Several cases of allergic contact dermatitis to 1,6 HDDA have already been reported in the literature, including one related to the coating of a glucose sensor transmitter, another involving medical devices used by patients with ostomy, and the last one linked to a hospital wristband [8, 9, 10]. A case of toxic epidermal necrolysis–like contact dermatitis caused by ultraviolet‐cured inks containing 1,6 HDDA has also been described [11].
The patient had worn the ski boots twice before the dermatitis occurred without any reaction, and when patch tested, was highly positive also at extremely low concentrations of 1,6 HDDA (0.001%) indicating that the sensitisation occurred through the boots. The sensitisation as such is surprising; the possibility of a manufacturing defect of the first ski boots, with excessive quantities of 1,6 HDDA in the glue used to bond the black fabric to the foam, or in the materials themselves that make up the liner might be considered.
The recurrence of the dermatitis with a new pair of boot liners from a different brand suggests the presence of (meth)acrylates, although not identified.
Efforts have been made to investigate how commonly reactions like these are, but we couldn't obtain any information from the ski boot manufacturer or the manufacturer of the foam inside the boot liners.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. D. Johansen , K. Aalto‐Korte , T. Agner , et al., “European Society of Contact Dermatitis Guideline for Diagnostic Patch Testing ‐ Recommendations on Best Practice,” Contact Dermatitis 73 (2015): 195–221.26179009 10.1111/cod.12432 · doi ↗ · pubmed ↗
- 2B. Marzario , D. Burrows , and S. Skotnicki , “Contact Dermatitis to Personal Sporting Equipment in Youth,” Journal of Cutaneous Medicine and Surgery 20, no. 4 (2016): 323–326.26471743 10.1177/1203475415611377 · doi ↗ · pubmed ↗
- 3N. Raison‐Peyron and D. Sasseville , “Acetophenone Azine,” Dermatitis 32, no. 1 (2021): 5–9.33273242 10.1097/DER.0000000000000697 · doi ↗ · pubmed ↗
- 4R. Montgomery , S. J. Stocks , and S. M. Wilkinson , “Contact Allergy Resulting From the Use of Acrylate Nails Is Increasing in Both Users and Those Who Are Occupationally Exposed,” Contact Dermatitis 74, no. 2 (2016): 120–122.26763991 10.1111/cod.12497 · doi ↗ · pubmed ↗
- 5A. Herman , L. de Montjoye , I. Tromme , A. Goossens , and M. Baeck , “Allergic Contact Dermatitis Caused by Medical Devices for Diabetes Patients: A Review,” Contact Dermatitis 79, no. 6 (2018): 331–335.30264920 10.1111/cod.13120 · doi ↗ · pubmed ↗
- 6A. C. de Groot and T. Rustemeyer , “2‐Hydroxyethyl Methacrylate (HEMA): A Clinical Review of Contact Allergy and Allergic Contact Dermatitis. Part 2. Cross‐ and Co‐Sensitization, Other Skin Reactions to HEMA, Position of HEMA Among (Meth)acrylates, Sensitivity as Screening Agent, Presence of HEMA in Commercial Products and Practical Information on Patch Test Procedures,” Contact Dermatitis 90, no. 1 (2024): 1–16.37778325 10.1111/cod.14430 · doi ↗ · pubmed ↗
- 7M. Wilkinson , M. Gonçalo , O. Aerts , et al., “The European Baseline Series and Recommended Additions: 2019,” Contact Dermatitis 80 (2019): 1–4.30421432 10.1111/cod.13155 · doi ↗ · pubmed ↗
- 8I. Siemund , J. Dahlin , M. Mowitz , N. Hamnerius , and C. Svedman , “Allergic Contact Dermatitis due to 1,6‐Hexanediol Diacrylate in Ostomy Patients,” Contact Dermatitis 90, no. 5 (2024): 501–506.38332444 10.1111/cod.14516 · doi ↗ · pubmed ↗