Allergic Contact Dermatitis to Colophonium in a ‘Carnival Mask’
Gabriela Blanchard, Olivier Sorg, Pierre Piletta‐Zanin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
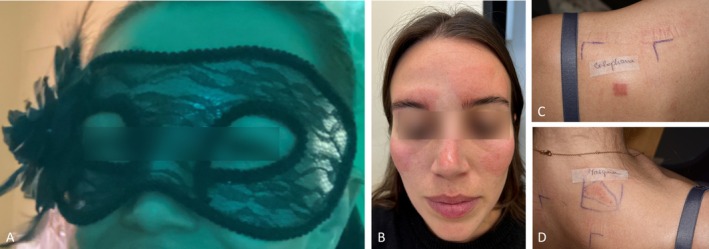 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsContact Dermatitis and Allergies · Immunotoxicology and immune responses · Pesticide Exposure and Toxicity
Colophonium is a frequent cause of allergic contact dermatitis (ACD) with an estimated prevalence of 3.1% among patch‐tested patients in Europe [1]. Abietic acid isomers are the main components of colophonium, and their oxidation products are thought to be the primary allergens in colophonium [2].
Case Report
1
A 30‐year‐old Caucasian female developed a well‐demarcated, itchy facial erythema within 24 h of wearing a Halloween mask (Figure 1A,B), consistent with ACD. She was treated with topical corticosteroids followed by topical pimecrolimus, until reaching complete remission. Patch tests were performed using the European baseline, preservative and emulsifier series (supplied by Chemotechnique Diagnostics, Vellinge, Sweden) using IQ Ultra chambers (Chemotechnique Diagnostics) and the patient's own products, including a piece of the mask used (‘as is’). Allergens were applied for 48 h. Readings on day (D) 2 and D4 showed +++ positive reactions for colophonium (20% Pet) (Figure 1C), as well as the patient's mask (Figure 1D). This led us to hypothesise that the mask likely contained colophonium. As the individual mask ingredients were not available, we proceeded with a high‐performance liquid chromatography analysis to confirm this hypothesis. Abietic acid was found at a concentration of 2.65 ± 0.02 mg/g in both the frontal and temporal zones of the mask (see Supporting Information S1 and S2).
(A) The colophanium‐containing face mask worn by the patient. (B) Well‐demarcated facial erythema consistent with allergic contact dermatitis. (C) Strong positive patch test reaction to colophonium on day 4 (+++). (D) Strong positive patch test reaction to the patient's mask on day 4 (+++).
Discussion
2
The detection of abietic acid in both the frontal and temporal zones of the patient's mask confirms the diagnosis of ACD caused by colophonium derivatives. Colophonium is a naturally occurring resin found in the sap of coniferous trees. It is commonly used as a component of adhesives, such as tapes and glues [3], as well as in cosmetics, paper products and footwear [4]. It is interesting to note that the interior part of the mask (in contact with the patient's skin) was smooth without any adhesivity. According to Regulation No. 1272/2008 of the European Parliament and Council, the manufacturers and importers of colophony‐containing products should label them ‘Contains colophony. May produce an allergic reaction’ if the colophony content exceeds 0.1% [5]. Nevertheless, due to the lack of standardised quantification methods, even in the absence of such labelling, clinicians should maintain a high degree of suspicion for sensitization to abietic acid or colophonium in cases of ACD, including those involving non‐adhesive products.
Consent
The authors obtained written consent from the patient for their photographs and medical information to be published in print and online and with the understanding that this information may be publicly available. Patient consent forms were not provided to the journal but are retained by the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1: Supporting Information.
Figure S1: Chromatogram for abietic acid.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1W. Uter , A. Bauer , A. Belloni Fortina , et al., “Patch Test Results With the European Baseline Series and Additions Thereof in the ESSCA Network, 2015–2018,” Contact Dermatitis 84, no. 2 (2021): 109–120.32945543 10.1111/cod.13704 · doi ↗ · pubmed ↗
- 2M. Pesonen , K. Suuronen , S. Suomela , and K. Aalto‐Korte , “Occupational Allergic Contact Dermatitis Caused by Colophonium,” Contact Dermatitis 80, no. 1 (2019): 9–17.30229960 10.1111/cod.13114 · doi ↗ · pubmed ↗
- 3A. M. Downs and J. E. Sansom , “Colophony Allergy: A Review,” Contact Dermatitis 41, no. 6 (1999): 305–310.10617209 10.1111/j.1600-0536.1999.tb 06178.x · doi ↗ · pubmed ↗
- 4L. D. Bugnet , S. Sanchez‐Politta , O. Sorg , and P. Piletta , “Allergic Contact Dermatitis to Colophonium‐Contaminated Socks,” Contact Dermatitis 59, no. 2 (2008): 127–128.18759888 10.1111/j.1600-0536.2008.01341.x · doi ↗ · pubmed ↗
- 5A. T. Karlberg , M. H. Albadr , and U. Nilsson , “Tracing Colophonium in Consumer Products,” Contact Dermatitis 85, no. 6 (2021): 671–678.34291483 10.1111/cod.13944 · doi ↗ · pubmed ↗