Temporal Predictions from Anhedonia To Anxiety in Adolescents with Major Depressive Disorder
Yannie D. Lee, Kenneth Towbin, Daniel S. Pine, Argyris Stringaris, Katharina Kircanski

TL;DR
This study shows that anhedonia, a key symptom of depression, is linked to social anxiety in adolescents with major depressive disorder.
Contribution
The study reveals that anhedonia predicts future social anxiety but not generalized anxiety in adolescents with MDD.
Findings
Anhedonia is concurrently associated with both social and generalized anxiety symptoms.
Anhedonia predicts future social anxiety symptoms but not generalized anxiety.
Neither social nor generalized anxiety predicts anhedonia over time.
Abstract
Anhedonia is a hallmark symptom of major depressive disorder (MDD) characterized by diminished ability to experience pleasure, motivation, or interest in usual activities. Anhedonia also is recognized as a transdiagnostic symptom dimension, but its links to other symptom dimensions are not fully elucidated. Given the high rates of depression and anxiety comorbidity in adolescence, we assessed concurrent and longitudinal associations between anhedonia and anxiety symptoms in adolescents diagnosed with MDD. The sample consisted of 157 adolescents with MDD (Mage = 15.54, 71.34% female) who were followed for several years in a research context involving longitudinal observation and, for a portion of the sample, treatment. Participants regularly completed self-report measures of anhedonia and anxiety symptoms across time. Data were analyzed using multilevel modeling to examine within-person…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
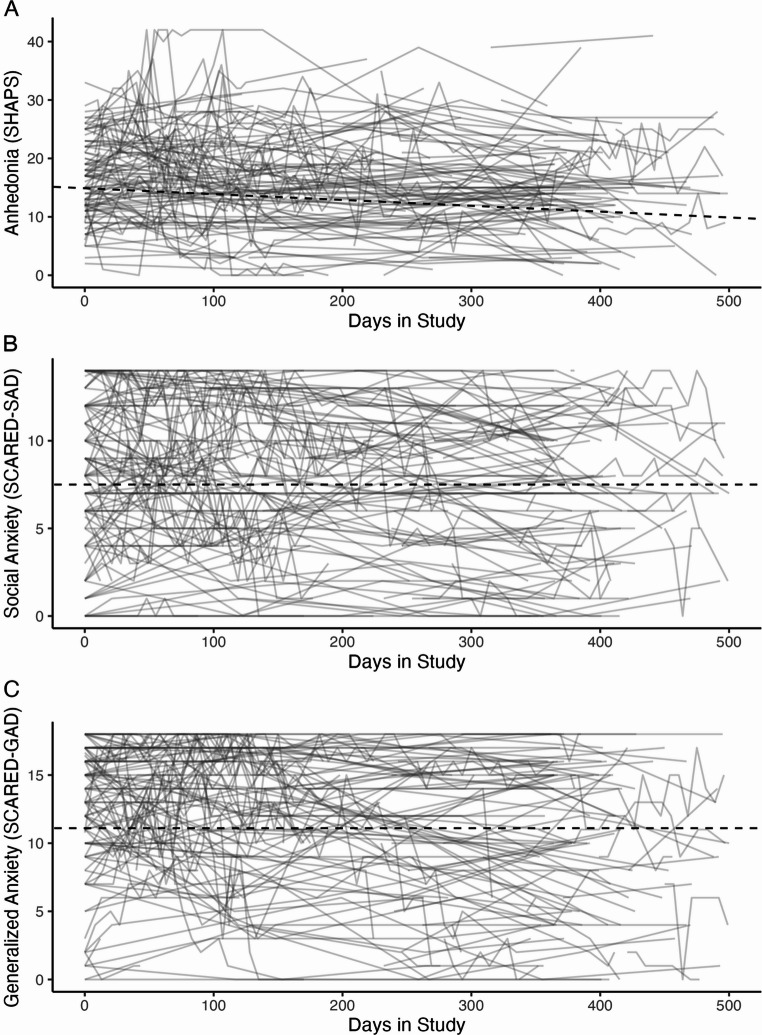 Figure 1
Figure 1- —National Institute of Mental Health (NIMH)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild and Adolescent Psychosocial and Emotional Development · Mental Health Research Topics · Anxiety, Depression, Psychometrics, Treatment, Cognitive Processes
Introduction
Anhedonia is a core symptom of major depressive disorder (MDD) that manifests as a pervasive reduction in the ability to derive pleasure, motivation, or interest from usual activities (American Psychiatric Association [APA], 2022). In adult samples, anhedonia has emerged as a transdiagnostic symptom dimension, implicated across a wide range of psychopathology, such as attention-deficit hyperactivity disorder, autism spectrum disorder, schizophrenia, and substance use disorders (Guineau et al., 2023); Liang et al., 2022). However, its role in MDD is particularly pronounced, as anhedonia is a predictor of poor psychosocial outcomes (Wong et al., 2024), psychological and pharmacological treatment response (McMakin et al., 2012); Spijker et al., 2001); Treadway & Zald, 2011); Vrieze et al., 2013), and heightened risk for suicide-related outcomes (Auerbach et al., 2022); Nock & Kazdin, 2002); Winer et al., 2014). Despite its clinical significance, anhedonia remains largely unaddressed by existing cognitive and behavioral therapies (Cuijpers et al., 2014); Pizzagalli, 2022); Sandman & Craske, (Sandman and Craske 2022), which primarily target reductions in negative affect rather than enhancements in positive affect or hedonic capacity. While anhedonia has been extensively studied in adults, far less is known about its role in youth, particularly in relation to anxiety and depression comorbidity. This gap is especially relevant for adolescents with MDD, a population in which anhedonia may play a central role in the etiology and maintenance of depression, and may also contribute to the frequent comorbidity between depression and anxiety (Gupta et al.,(Gupta et al. 2024a). Given anhedonia’s potential role in exacerbating both depression and anxiety, the current study examined its relationship with anxiety in adolescents with MDD, conceptualizing it as a key mechanism underlying their comorbidity.
Depression and anxiety are highly comorbid in youth (Kalin, 2021); Melton et al., 2016). Studies indicate that approximately 25–50% of youth with depression also meet criteria for an anxiety disorder (Garber & Weersing,(Garber and Weersing 2010), while about 10–15% of those with an anxiety disorder experience comorbid depression (Cummings et al., 2014), underscoring the frequent co-occurrence and clinical significance of these conditions in early development (Long et al., 2018).
Despite the high prevalence and clinical impact of depression-anxiety comorbidity in youth, research has largely overlooked the mechanistic role of anhedonia in this relationship. Studies have established that comorbid anxiety amplifies the severity and chronicity of depression (Aderka et al., 2012); Franco et al., 2007); Koyuncu et al., 2019); O’Neil et al., 2010), and risk for various adverse outcomes such as suicidality (Nock et al., 2010), yet few have examined how anhedonia contributes to this exacerbation in adolescent populations. Given anhedonia’s association with poor treatment response (McMakin et al.,(McMakin et al. 2012) and heightened clinical severity in MDD (Gabbay et al., 2015), it is plausible that it also plays a central role in sustaining or worsening comorbid anxiety, further complicating clinical outcomes. These effects may be particularly pronounced during adolescence, a developmental stage marked by heightened vulnerability to mood and anxiety disorders.
Adolescence is a period of heightened vulnerability to anxiety and depression (Garber & Weersing, 2010); Johnson et al., 2018); McLaughlin & King, 2015). This coincides with enhanced plasticity in reward-responsive brain areas (Foulkes & Blakemore, 2016); Galván, 2010, 2013); Walker et al., 2017), which may increase sensitivity to disruptions in hedonic processes. Given the interplay between neurodevelopment and psychopathology, adolescence may be a particularly sensitive period for the emergence and trait stabilization of anhedonia, influencing both depression and anxiety trajectories. For example, one study found that adolescent anhedonia was uniquely associated with more severe clinical outcomes, including greater overall illness severity, higher suicidality scores, longer episode duration, and a greater number of depressive episodes (Gabbay et al., 2015). A clinical trial examining treatment-resistant adolescents revealed that anhedonia uniquely predicted a longer time to remission and fewer depression-free days during second-step treatment with selective serotonin reuptake inhibitors (SSRIs) and cognitive-behavioral therapy (McMakin et al., 2012). Furthermore, preliminary findings suggest that anhedonia may follow distinct developmental trajectories across adolescence, with some adolescents experiencing stable or decreasing symptoms while others exhibit persistence or worsening over time (Gupta et al., 2024b). Among at-risk adolescents, lower depression severity emerged as a potential protective factor, buffering against the persistence or exacerbation of anhedonia as they transitioned into adulthood. These variations in anhedonia trajectories suggest that some adolescents may be more resilient to its long-term effects, while others remain vulnerable to worsening symptoms that contribute to later psychopathology. Altogether, these findings underscore the clinical significance of anhedonia in adolescent MDD and impact on illness severity, clinical trajectories, and treatment outcomes.
Historically, theoretical models of anxiety and depression have characterized anhedonia as a facet of low positive affect, a trait unique to depression (e.g., Clark & Watson, 1991). However, reconsidering anhedonia within a transdiagnostic framework may provide new insights into the mechanisms underlying co-occurring depression-anxiety in adolescence. For instance, Winer and colleagues (2017) conducted three studies examining the interplay among anhedonia, anxiety, and depressive symptoms in a non-clinical sample of adults. They found that anxiety-driven avoidance moderated the relationship between anxiety and depression, particularly among individuals who avoided highly enjoyable activities, ultimately leading to increased depressive symptoms. Furthermore, they demonstrated that anxiety mediated both cross-sectional and longitudinal associations between anhedonia and depression, with this mediation emerging consistently across multiple timepoints. Notably, anxiety symptoms emerged as a key mediator linking recent increases in anhedonia to later depressive symptoms. This highlights the central role of anxiety in the pathway from reward dysfunction to depression and suggests it may be a mechanism through which changes in hedonic capacity shape depressive symptom trajectories.
In a complementary vein, recent work has identified how anhedonia may also impede recovery from anxiety by disrupting reward-related processes essential to therapeutic success. Specifically, anhedonia has been proposed as a barrier to recovery in anxiety due to its influence on reward valuation, responsiveness, and learning. For example, diminished reward valuation may lead individuals to perceive potential rewards as less attainable or worthwhile, tipping the balance in favor of avoidance over approach behaviors (Pittig et al., 2021). Moreover, reduced responsiveness to rewards—either anticipated or experienced—may interfere therapeutic exposures to threat-relevant contexts, limiting opportunities for positive reinforcement and new learning (Rosenberg & Horowitz et al., 2024). As such, altered reward processing may represent a key mechanism through which anhedonia perpetuates both anxiety and depression, underscoring the need for further research into how specific anxiety symptoms are associated with hedonic deficits during critical periods of development.
Mixed findings link anhedonia to generalized anxiety disorder (GAD; Brown et al., 1998); Prenoveau et al., 2010), whereas stronger evidence supports its association with social anxiety disorder (SAD). SAD shares substantial clinical overlap with depressive symptomatology—including sadness, loneliness, poor self-esteem, and low positive affect—and is highly prevalent among youth with comorbid MDD (Adams et al., 2016; Danneel et al., 2019; Stein et al. 2005). Adults with severe social anxiety symptoms exhibit blunted reward responsiveness similar to that seen in depression (Kashdan, 2004, 2007) and report lower levels of both state and trait positive affect (Kashdan & Steger, 2006). Emerging evidence indicates that these associations are also present in adolescents (Bakker et al., 2017); Forbes & Dahl, 2012); Leventhal et al., 2017), suggesting that hedonic deficits may be rooted early on in development. Luckhardt and colleagues (Luckhardt et al. 2023) found that adolescents with comorbid MDD and SAD exhibited blunted reward anticipation and processing on a gambling task, mirroring patterns seen in adults with depression (Luking et al., 2016). Similarly, reward-related deficits in both social and non-social contexts have been linked to treatment response in youth with anxiety and depression, suggesting that altered reward processing may contribute to the persistence of anxiety symptoms over time (Schwartz et al., 2019). Despite these findings, research on anhedonia in adolescents with co-occurring MDD and anxiety remains scarce. Most existing studies have focused on adult, non-clinical samples and cross-sectional designs, limiting insight into how anhedonia relates to social and generalized anxiety over the course of development.
The present study aims to bridge this gap by examining the longitudinal relationships between anhedonia, social anxiety, and generalized anxiety in adolescents diagnosed with MDD. Specifically, we assess both concurrent and longitudinal relationships between anhedonia and anxiety symptoms. Anhedonia may maintain and exacerbate generalized anxiety by diminishing reward valuation and responsiveness, reinforcing avoidance behaviors, and perpetuating a maladaptive feedback loop (Taylor et al., 2022). As reward motivation diminishes, individuals may increasingly turn to avoidance as a coping mechanism. Although this may offer short-term relief, it can exacerbate anxiety and reduce engagement with potentially rewarding experiences over time (Rosenberg & Horowitz et al., 2024). Consequently, this pattern may hinder exposure to corrective experiences and perpetuate motivational and hedonic deficits. Social anxiety, a well-established risk factor for depression (Adams et al., 2016); Dalrymple & Zimmerman, 2007); Griffith et al., 2020); Kalin et al., 2021; Koyuncu et al., 2019); Ohayon & Schatzberg, 2010); Long et al., 2018); Rapee et al., 2019), may also arise from depression-related interpersonal challenges, such as peer rejection, social withdrawal, and impaired social skills (Cummings et al., 2014); Danneel et al., 2019); Hamilton et al., 2016); Jacobson & Newman, 2017). Consistent with cumulative interpersonal risk models of social anxiety and depression (Epkins & Heckler, 2011), repeated negative social experiences—such as low peer acceptance, social exclusion, or difficulty forming or maintaining relationships—may reinforce avoidance behaviors and further entrench comorbid symptoms over time. These dynamics are particularly salient in the context of adolescence, a critical period when peer relationships significantly shape psychosocial well-being and identity (Corsano et al., 2006); Lamblin et al., 2017); Oberle et al., 2010); Roach, 2018). First, we hypothesized that anhedonia would be positively associated with social and generalized anxiety symptoms concurrently. Second, we hypothesized that anhedonia would share a positive, reciprocal relationship with both social and generalized anxiety over time.
Methods
Participants
Data for the present study was collected as part of the Characterization and Treatment of Depression (CAT-D) study at the National Institute of Mental Health (NIMH), a longitudinal cohort study focused on the characterization and treatment of depression in adolescents (Sadeghi et al., 2022; CAT-D data openly available at https://github.com/transatlantic-comppsych/CATD-study). The cohort encompassed both adolescents with depression and nonpatient controls, monitoring their development and progress over the span of several years. Recruitment began in December of 2018. Participants were recruited primarily from the Washington metropolitan region, identified through locally distributed postcards aimed at identifying adolescents exhibiting symptoms of MDD. Community practitioner referrals were also utilized for recruitment. All participants were assessed by trained clinicians who utilized the Kiddie Schedule for Affective Disorders and Schizophrenia - Present and Lifetime Version (KSADS-PL; Kaufman et al., 1997), a semi-structured diagnostic interview. Out of 170 adolescents with MDD initially enrolled in the cohort, 157 completed the required assessments for inclusion and provided permission for data sharing in this analysis. Of these 157 adolescents, 122 completed the KSADS in-person, while 35 completed the face-to-face clinical KSADS interview using telehealth platforms due to COVID-19-related restrictions. Inclusion criteria consisted of individuals between the ages of 11 and 17 at the time of enrollment and who had met criteria for a previous or ongoing diagnosis of MDD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; APA,2013). Exclusion criteria included: a diagnosis of schizophrenia, schizophreniform disorder, schizoaffective illness, bipolar disorder, severe autism spectrum disorder, anorexia nervosa, or other severe eating disorders; an intelligence quotient (IQ) of < 70 on the Wechsler Abbreviated Scale of Intelligence - Second Edition (WASI II; Wechsler, (Wechsler 2011); depressive symptoms due to effects of drugs of abuse or a neurological condition; a diagnosis of alcohol or other substance use disorders; current active suicidal ideation; repeated self-harm in the context of interpersonal conflict; and serious medical conditions such as epilepsy or heart disease. All participants provided written consent as part of standard enrollment procedure and received monetary compensation for research task and questionnaire completion. As part of the study, adolescents with current diagnosis of MDD were also offered treatment in the form of evidence-based cognitive behavioral therapy (CBT), primarily consisting of behavioral activation (BA).
Procedures
The study comprised two primary parts: (1) Characterization and (2) Treatment. In the Characterization portion, all participants engaged in various behavioral tasks and underwent neuroimaging scans (i.e., magnetic resonance imaging and magnetoencephalography), and completed structured follow-up assessments at approximately 6-, 12-, 18-, and 24-months post-enrollment. Individuals with ongoing major depression expressing interest treatment were given evidence-based CBT sessions on a weekly basis, for a maximum of 13 weeks. The intervention was based on incorporating BA with components of MATCH-ADTC (Chorpita & Weisz, 2009) and was designed as a 13–14 session protocol with each session lasting approximately 1.5–2 h. Given this variability in engagement and the fact that most participants did not complete a full treatment dose (M = 7.11), we did not separate participants into distinct treatment and non-treatment groups in our analyses. At each visit, participants were asked to complete several self-report measures including measures of anhedonia and anxiety symptoms (details below). All research procedures were approved by the Institutional Review Board (IRB). Due to the COVID-19 pandemic, a substantial portion of the data were collected during a period that only allowed for virtual visits. Additionally, the number of total visits for each participant varied (range = 1–25, M = 8.22, SD = 5.44), and days between visits were not standardized (range = 6-1758, M = 465.24, SD = 399.75). Test-retest reliability and internal consistency were calculated using all available timepoints, regardless of the number of visits per participant or the time between them. We computed single-measure two-way random-effects ICCs [ICC(2,1)] with 95% confidence intervals to evaluate absolute agreement across all available timepoints (Koo & Li, 2016). Internal consistency was assessed using Cronbach’s alpha (α) and McDonald’s omega (ω).
Measures
Anhedonia
The Snaith-Hamilton Pleasure Scale (SHAPS; Snaith et al., (Snaith et al. 1995) is a 14-item self-report measure of anticipated hedonic response, or lack thereof, to typically pleasurable experiences. These experiences span sensory, social, and intrapersonal domains (e.g., “I would be able to enjoy my favorite meal”, “I would enjoy being with my family or close friends”, “I would find pleasure in my hobbies and pastimes”). The SHAPS has demonstrated robust internal consistency in clinical samples (α = 0.82-0.91; Franken et al., 2007); Langvik & Austad, 2019; Nakonezny et al., 2015) and adequate reliability in adolescent populations (α = 0.87; Leventhal et al., 2015).
Items are rated on a 4-point Likert-type scale (0 = strongly agree; 3 = strongly disagree) and yield a severity score ranging from 0 to 42, with higher scores indicating greater levels of anhedonia. The present study utilized total scores (internal consistency in present sample: α = 0.93, ω = 0.94). Test-retest analyses demonstrated moderate reliability across time (ICC = 0.61).
Social and Generalized Anxiety
The self-report version of the Screen for Child Anxiety Related Disorders (SCARED; Birmaher et al., 1997) was used to assess social and generalized anxiety. The SCARED consists of 41 items that screen for the presence of five anxiety disorders over the past three months: generalized anxiety disorder, separation anxiety disorder, panic disorder, social anxiety disorder, and school avoidance. Participants responded to a series of statements indicating the degree to which the statements described them (e.g., “I am nervous”, “People tell me that I worry too much”, “It is hard for me to talk with people I don’t know well”) on a 3-point Likert scale (0 =not true or hardly ever true; 1 = somewhat true or sometimes true; 2 = very true or very often true). The measure yields a total score as well as five subscale scores. The total SCARED has demonstrated excellent internal consistency (α = 0.91), while the social and generalized anxiety subscales have shown good reliability, with α = 0.78 and α = 0.81, respectively (Runyon et al., 2018). Subscale scores were used in all analyses, demonstrating strong internal consistency in the present sample (social anxiety: α = 0.91, ω = 0.93; generalized anxiety: α = 0.92, ω = 0.94). Test-retest analyses demonstrated good reliability across both subscales (social anxiety: ICC = 0.73; generalized anxiety: ICC = 0.76).
Statistical Analyses
Data were analyzed using R (version 4.4.2; RStudio Team, 2024) and HLM 8.0 (Raudenbush & Congdon, 2021). Internal consistency and reliability analyses, including baseline Pearson correlations, Cronbach’s alpha, McDonald’s omega, and intraclass correlation coefficients (ICCs) were calculated using the psych package (version 2.4.12; Revelle, 2024). Statistical assumptions were tested using the dplyr package (version 1.1.4; Wickham et al., 2023). Power analyses were conducted using the pwr package (version 1.3-0; Champely, 2020). Data visualization was modeled using the ggplot2 package (version 3.3.3; Wickham, 2016). Given the hierarchical structure of the data in which time points were nested within participants, we employed multilevel modeling (MLM). MLM enabled simultaneous estimation of within- and between-person effects, while accommodating varying time intervals between time points, and accommodating missing data through implementation of restricted maximum likelihood estimation (REML) (Snijders & Bosker, 2011). For our analyses, we combined all available time points per participant (i.e., Characterization and Treatment, when applicable). This approach maximized the number of data points, bolstering statistical power. To account for variability between time points in time-lagged MLMs, a time-point difference variable was calculated corresponding to the number of days between consecutive time points (days) in the study and included as a level-1 covariate. Random intercepts and slopes were specified in all models. Robust standard errors were used. Level-1 predictors were centered around the group (person) mean, such that coefficients represent the relation between the predictor and outcome within person. In all equations below, i denotes time points and j denotes participants. As multiple statistical models were conducted, each with multiple predictors, all results were false discovery rate (FDR)-corrected (Benjamini-Hochberg procedure) with the percentage of false positives set toq = 0.05. As such, results reported in the text and tables represent raw coefficients and standard errors from the MLMs along with FDR-corrected p values.
Assumptions of Statistical Models
Following the recommendations of Snijders and Bosker (2011), we assumed normality of level-1 residuals and level-2 random coefficients, homogeneity of variance at level-1, and a constant covariance matrix for level-2 random coefficients.
Distribution of level-1 residuals and level-2 random coefficients were assessed using Shapiro-Wilk tests. Results indicated significant deviations from normality for all models at level-1 (W range: 0.960–0.986, p <.001). For level-2 random coefficients, results were mixed. Cross sectional and longitudinal models where anhedonia predicted anxiety symptoms deviated significantly from normality (W range: 0.933–0.979, ps < 0.001) while longitudinal models where anxiety symptoms predicted anhedonia met normality assumptions (W range: 0.983–0.984, ps > 0.071. Q-Q plots suggested that residuals were normally distributed at the center but showed deviations at the tails (eFigure 1 in the Supplement).
Homogeneity of variance was assessed using Levene’s test. All models were significant (Fs = 1.30–2.71, ps < 0.05), indicating heteroscedasticity at the participant-level. To evaluate whether the assumption of a constant covariance matrix for level-2 random coefficients was met, likelihood ratio tests were conducted to compare models with random intercepts only to models with both random intercepts and slopes. For all models, the likelihood ratio tests were significant (ps < 0.001), indicating that including random slopes significantly improved model fit and that the effects of predictors varied meaningfully across participants, suggesting heterogeneity in the covariance matrix.
Concurrent Associations
We first tested for concurrent associations of anhedonia with social anxiety and generalized anxiety within persons, within time points (Fox & Weisberg 2019).
Level-1 Models (time point level; separate equations used for social anxiety and generalized anxiety):
Anhedonia_ij_ = β_0j_ + β_1j_(Social Anxiety or Generalized Anxiety) + r_ij_.
Level-2 Model (participant level):
β_0j_ = γ_00_ + u_0j_.
β_1j_ = γ_10_ + u_1j_.
Here, Anhedonia_ij_ refers to the level of anhedonia for participant j at time point i, β_1j_ refers to the association between level of social anxiety or generalized anxiety and level of anhedonia for participant j, and r_ij_ is the within-person residual variance. γ_00_ refers to the mean level of anhedonia across participants, γ_10_ refers to the mean association between level of social anxiety or generalized anxiety and anhedonia across participants, and u_0j_ and u_0j_ are the respective between-person random effects.
Temporal Associations
We next texted for time-lagged associations of anhedonia with social anxiety and generalized anxiety within persons. Sample equation:
Level-1 Models (time point level; four separate models conducted):
Anhedonia_ij(t)_ = β_0j_ + β_1j_(Social Anxiety_t−1_) + β_2j_(Anhedonia_t−1_) + β_3j_(Days Between t and t-1_t_) + r_ij_.
Level-2 Models (participant level):
β_0j_ = γ_00_ + u_0j_.
β_1j_ = γ_10_ + u_1j_.
β_2j_ = γ_20_ + u_2j_.
β_3j_ = γ_30_ + u_3j_.
Here, β_1j_ refers to the prediction of anhedonia at the current time point (t) by social anxiety at the previous time point (t-1). The analysis covaries β_2j_ as the level of anhedonia at the previous time point (t-1), such that results for β_1j_ reflect the effect of social anxiety on subsequent change in level of anhedonia. The analysis also covaries β_3j_, the number of days in between t and t-1.
Power Analyses
We estimated power for key fixed effects in cross-sectional and longitudinal designs, assuming a one-sample t-test framework adjusted for clustering. Analyses targeted 80% power at α = 0.05 to detect small (d = 0.2), medium (d = 0.5), and large (d = 0.8) effect sizes (Cohen, 1988), with an assumed average of 7 observations per participant. Results indicated that detecting a small effect (d = 0.2) required 397 total observations (57 participants), a medium effect (d = 0.5) required 67 observations (10 participants), and a large effect (d = 0.8) required 29 observations (6 participants). Our cross-sectional sample comprised 1,517 observations from 157 participants (M = 9.67 observations per participant), while the longitudinal sample included 1,047 observations from 137 participants (M = 7.65 observations per participant). These sample sizes exceeded a priori requirements, yielding > 99% power cross-sectionally and longitudinally for small effects (d = 0.2) and > 99% power for medium to large effects (d≥ 0.5), aligning with multilevel model considerations outlined by Arend and Schäfer (2019).
Results
Participant Characteristics
Baseline demographic and clinical characteristics of participants are presented in Table 1. The sample comprised 157 adolescents, with 121 participants diagnosed with ongoing MDD and 36 diagnosed with previous but not ongoing MDD at baseline (Mage = 15.54, SD = 1.63; 71.34% female; 66.88% White; 13.38% Biracial; 9.55% Black, 8.92% Asian, 0.64% declined to answer, 0.64% Pacific Islander). All participants completed a series of laboratory research visits in Characterization (N = 157, Mvisits = 8.64); some also completed weekly sessions of outpatient CBT (primarily BA) (N = 64, Msessions = 7.11). All available data were used for each analysis. The full sample (N = 157) was utilized in concurrent analyses. Baseline correlational analyses included 148 participants with complete data on all relevant measures. Longitudinal models included between 140 and 142 participants, depending on the specific variables included in each model and availability of data for each participant.
Table 1. Demographic and clinical characteristics of participantsVariableM (SD) or %; RangeAge15.54 (1.61); 11–18Sex (female)71.34Race White66.88 Biracial13.38 Black9.55 Asian8.92 Pacific Islander0.64 Declined to answer0.64Ethnicity Non-Hispanic0.90 Declined to answer0.02 Clinical Measures at BaselineSHAPS16.07 (6.92); 0–33SCARED-SAD7.88 (4.18); 0–14SCARED-GAD11.95 (4.88); 0–18SHAPS Snaith-Hamilton Pleasure Scale, SCARED-GAD Screen for Child Anxiety Related Disorders-Generalized Anxiety Subscale, SCARED-SAD Screen for Child Anxiety Related Disorders-Social Anxiety Subscale. N = 148 for baseline analyses
Baseline correlations between all measures are presented in Table 2. Additionally, Fig. 1 presents participants’ levels of anhedonia, social anxiety, and generalized anxiety across the first 500 days of the study, representing 58.80% of all data points. This timeframe was selected because participant attrition increased substantially after 500 days, resulting in fewer available data points beyond this period. Baseline means were calculated outside of the MLM model using all participants’ first available visit scores, which differ from those shown in Fig.1. It is important to note that some baseline data for questionnaires and diagnoses were missing for nine participants even though their IDs were included in the final dataset. As a result, the number of participants included in baseline analyses (N = 148) may differ slightly from the total sample size used in analyses (e.g., concurrent and longitudinal). The mean baseline SHAPS score across participants scores was 16.07; the SHAPS does not have established clinical cutoffs. An initial MLM testing SHAPS score as a function of the number of days in the study indicated that overall, the sample showed a decrease in anhedonia over time (b = − 0.003, p <.001). The mean baseline SCARED social anxiety subscale score was 7.88, with ≥ 8 being a clinically-significant threshold; the mean baseline SCARED generalized anxiety subscale score was 11.95, with ≥ 9 being a clinically significant threshold (Birmaher et al., 1997). Initial MLMs testing SCARED social anxiety and generalized anxiety scores as a function of the number of days in the study indicated that overall, the sample showed decreases in both social anxiety (b = − 0.001, p =.002) and generalized anxiety (b = − 0.002, p <.001) over time.Fig. 1. Anhedonia, social anxiety, and generalized anxiety scores across the first 500 days in study. Note. Each line represents an individual participant’s score over time, illustrating variability in trajectories. The black dashed line represents the MLM-predicted trajectory for each measure, derived from the equation using the intercept and slope for days in study
Table 2. Baseline pearson correlations for Anhedonia, Social, and generalized anxietyVariable1231. SHAPS---2. SCARED-SAD0.21*--3. SCARED-GAD0.190.54**-*p <.05. **p <.01. *** p <.001. Some baseline data were missing for nine participants, resulting in a slightly smaller sample size for these analyses (N = 148) than the full dataset (N = 157)
To explore whether baseline depression influenced associations between symptoms, we conducted exploratory Pearson correlations separately for participants with a previous (remitted) diagnosis of MDD (n = 36) and those with ongoing MDD (n = 121). Among participants with ongoing MDD, generalized and social anxiety symptoms were moderately correlated (r =.49, p <.001), but neither was significantly associated with anhedonia (SAD: r =.01, p =.92; GAD: r = −.04, p =.65). In contrast, within the previous MDD group, both generalized and social anxiety symptoms were significantly correlated with anhedonia (SAD: r =.19, p =.023; GAD: r =.21, p =.013), and GAD and SAD remained strongly related (r =.54, p <.001). A Fisher’s r-to-z comparison indicated that the association between GAD and anhedonia was significantly stronger in the previous MDD group than in the ongoing group (z = −2.12, p =.034). Differences in SAD–anhedonia correlations did not reach statistical significance (p =.13). These findings suggest potential variation in symptom relationships depending on depression status, though they were not guided by a priori hypotheses and should be interpreted with caution given the small sample size of the previous MDD group. To further contextualize these findings, we examined the baseline prevalence of anxiety disorders in the sample. Anxiety disorders were classified as either previous (lifetime) or ongoing (current). For social anxiety disorder, three participants were missing diagnostic data. Of the remaining 154 participants, 74 did not meet criteria for either previous or ongoing SAD, while 80 met criteria for previous SAD—79 of whom also met criteria for ongoing SAD. For generalized anxiety disorder (GAD), two participants were missing data. Of the remaining 155, 41 did not meet criteria for either previous or ongoing GAD, and 114 met criteria for both previous and ongoing GAD.
Concurrent Associations
Full results for all models testing concurrent associations are presented in Table 3. As hypothesized, anhedonia was significantly associated with both social anxiety (b = 0.46, p =.002) and generalized anxiety (b = 0.37, p =.002) within time points.
Temporal Associations
Full results for all models testing temporal associations are presented in Table 3. First, anhedonia, social anxiety, and generalized anxiety all showed significant auto-correlations from t-1 to t. Above and beyond these effects, as hypothesized, anhedonia at t-1 significantly predicted change in social anxiety from t-1 to t (b = 0.04, p =.008), such that within participants, higher-than-average levels of anhedonia predicted subsequent increases in social anxiety, whereas lower-than-average levels of anhedonia predicted subsequent decreases in social anxiety. However, contrary to expectations, anhedonia at t-1 did not predict change in generalized anxiety from t-1 to t (b = 0.03, p =.129). Likewise, social anxiety at t-1 did not predict change in anhedonia from t-1 to t (b = − 0.05, p =.671), and generalized anxiety at t-1 did not predict change in anhedonia from t-1 to t (b = 0.06, p =.458).
Table 3. Results of multilevel models testing Temporal associationsSocial Anxiety Predicting AnhedoniaPredictorUnstd. coeff. SE
t p valueIntercept (Anhedonia_t_) (β_0j_)14.890.6523.020.002Social Anxiety_t−1_ (β_1j_)−0.050.11−0.430.671Anhedonia_t−1_ (β_2j_)0.300.047.090.002Days Between t and t-1 (β_3j_)−0.010.00−1.120.293Generalized Anxiety Predicting AnhedoniaIntercept (Anhedonia_t_) (β_0j_)16.010.6226.010.002Generalized Anxiety_t−1_ (β_1j_)0.060.070.790.458Anhedonia_t−1_ (β_2j_)0.280.046.870.002Days Between t and t-1 (β_3j_)−0.010.00−1.150.293Anhedonia Predicting Social AnxietyIntercept (Soc. Anx.t) (β_0j_)7.500.3322.520.002Anhedonia_t−1_ (β_1j_)0.040.0142.830.008Social Anxiety_t−1_ (β_2j_)0.260.055.610.002Days Between t and t-1 (β_3j_)−0.000.00−1.490.187Anhedonia Predicting Generalized AnxietyIntercept (Gen. Anx.t) (β_0j_)11.100.4326.080.002Anhedonia_t−1_ (β_1j_)0.030.021.710.129Generalized Anxiety_t−1_ (β_2j_)0.240.055.170.002Days Between t and t-1 (β_3j_)−0.000.00−1.190.293
Discussion
The present study aimed to bridge gaps in the literature by exploring bidirectional relations between anhedonia and anxiety symptoms in adolescent MDD. We sought to comprehensively investigate both concurrent and temporal links of anhedonia with social anxiety and generalized anxiety symptoms at the within-person level. Consistent with our first hypothesis, anhedonia was positively associated with both social anxiety and generalized anxiety symptoms concurrently. Temporally, anhedonia emerged as a predictor of within-person change in social but not generalized anxiety at the subsequent time point, partially supporting our second hypothesis. That is, anhedonia was a unique temporal driver of social anxiety. This suggests that in adolescents with MDD, fluctuations in anhedonia may modulate the course of social anxiety symptoms across time, underscoring putative mechanistic links between anhedonia and social anxiety.
Notably, anhedonia predicted changes in social anxiety but not generalized anxiety. One potential explanation for this pattern is that unlike generalized anxiety, social anxiety is inherently tethered to reward-related processes. Social interactions involve reward anticipation, motivation, and learning (Kupferberg et al., 2016), making them especially relevant to anhedonia (Barkus & Badcock 2019). Adolescence is a period when peer acceptance and social belonging are critical to well-being (Marston et al., 2010); Sisk & Gee, (2022). During this time, social stressors become particularly salient, and the quality of social relationships plays a pivotal role in shaping mental health outcomes. By contrast, adolescents with diminished motivation and pleasure in response to social experiences may withdraw due to lowered expectations of enjoyment or a perceived inability to engage effectively (Watson et al., 2020). Over time, this reduced engagement may limit opportunities for positive reinforcement and social skill development, compounding both social anxiety and depression symptoms. In contrast, generalized anxiety disorder (GAD) is characterized by excessive, uncontrollable worry across multiple domains, including academic performance, health, and future uncertainty, rather than being narrowly tied to social contexts (Rowa et al., 2017). Although reward deficits might indirectly influence GAD symptoms—for instance, by dampening positive emotions (Eisner et al., 2009)—the primary characteristics of GAD may be more closely tied to broader cognitive processes than to specific reward-related dysfunction (Barkus & Badcock 2019).
Positive and negative social interactions can have profound effects on self-esteem, social competence, and overall well-being in early development. Anhedonia may reduce the drive to engage in positive social experiences (Watson et al., 2020), decreasing opportunities for connection and fostering feelings of alienation or inadequacy (Wittchen et al., 2000). Conversely, positive social relationships can serve as protective factors by promoting resilience and buffering against internalizing symptoms (Haddow et al., 2021); Kochel et al., 2017); Narr et al., (2019). Recognizing that social withdrawal and avoidance are core features of both social anxiety and depression, disruptions in interpersonal relationships during adolescence may contribute to the reciprocal associations between these conditions. Such dynamics have been explained through the lenses of Sensitivity Shift Theory (SST; Richey et al., 2019) and Reward Devaluation Theory (RDT; Winer & Salem, 2016). Sensitivity Shift Theory (SST) presents an integrated model addressing positive affect and motivational deficits in individuals with SAD. Social anhedonia refers to a trait-like disinterest in and absence of pleasure derived specifically from social interactions, and according to SST, a subset of youth who exhibit heightened sensitivity to both positive and negative social contexts may develop social anxiety through social anhedonia-driven avoidance. Reward Devaluation Theory (Winer & Salem, 2016) proposes that a subset of individuals with depression devalue and actively avoid positive or rewarding stimuli due to repeated associations with negative outcomes or potential for disappointment. In this way, positive experiences may become internally threatening, fostering avoidance of social situations that might otherwise be rewarding. Given the relatively stable nature of anhedonia throughout development (Bennik et al., 2014); Conway et al., (2017), reward-related aberrations may manifest as early risk factors that drive and maintain social anxiety symptoms through avoidance and negative reinforcement (Barkus, 2021); Taylor et al., (2022).
The unidirectional relationship from anhedonia to social anxiety raises important considerations. In adolescents with MDD, it is possible that reward dysfunction precedes and drives the emergence and maintenance of social anxiety symptoms, rather than vice versa. Notably, just over half of the current sample met criteria for both previous and ongoing SAD, suggesting chronicity for many but also variability in onset and course. During adolescence—a period in which peer rejection is acutely felt and social rewards are paramount (Somerville, (2013); (Lynn Mulvey et al. 2017)—this withdrawal may heighten fears of negative evaluation and reinforce avoidance behaviors, fueling social anxiety symptoms over time. Social anxiety involves a fundamental conflict between approach and avoidance tendencies (APA, 2013). While adolescents with social anxiety may deeply desire social connection, the fear of embarrassment and negative evaluation can create a paradox (Alden & Taylor, 2010); Caouette & Guyer, (2014). That is, they may deeply crave social acceptance yet simultaneously believe they are undeserving or incapable of achieving it. This internal conflict can lead to avoidance of social interactions despite a strong underlying desire for connection, reinforcing social anxiety and negative self-perceptions over time. Considering the heterogeneity of depression in adolescence (Chahal et al., 2020; Rice et al., 2019); (Thapar et al., 2022); Yaroslavsky et al., (Yaroslavsky et al. 2013), anhedonia may not affect all adolescents with MDD in the same way. For instance, those with comorbid SAD may experience more entrenched reward-related deficits than those without. Emerging evidence suggests that certain facets of reward-processing (i.e., sensitivity, motivation, learning; motivation; (Boyle et al., 2023) may contribute to distinct clinical presentations (Borsini et al., 2020); (Winer et al., 2019). Future work should investigate how subtypes of anhedonia (e.g., consummatory, anticipatory, learning; (Craske et al., 2016) manifest across different internalizing disorders and whether specific deficits in reward processing confer differential risk for specific forms of anxiety (i.e., social or generalized anxiety) compared to depression.
Exploratory analyses from the current study also revealed that baseline associations between anxiety and anhedonia differed based on MDD status, i.e., previous vs. ongoing. Specifically, the correlation between generalized anxiety symptoms and anhedonia was significantly stronger in adolescents with a previous (remitted) diagnosis of MDD compared to those with ongoing MDD. This finding, while post hoc and limited by a relatively small subgroup sample size, suggests that the nature of symptom relationships may shift along with depressive symptomatology. These preliminary results highlight the importance of considering diagnostic status when examining symptom dynamics and suggest that remission may alter the strength or salience of reward-related processes in relation to anxiety.
Beyond depression status, the co-occurrence of MDD and anxiety disorders at baseline in this study may have further shaped the symptom relationships observed over time. Given the high rates of comorbidity between these conditions, anxiety symptoms may contribute to persistent anhedonia, even among adolescents whose depressive symptoms have remitted. Moreover, the distinction between previous and ongoing MDD, in combination with anxiety disorder status, may shape the strength and direction of symptom interactions in ways not fully captured in this study. Although this study did not explicitly test these interactions, our findings underscore the value of a dimensional, symptom-based framework for tracking fluctuations in anhedonia and anxiety over time. Future research may benefit from simultaneously modeling changes in diagnostic status and symptom severity to better capture the dynamic nature of comorbid internalizing symptoms during adolescence.
Because our study focused on adolescents with MDD, anhedonia may have played a more central role in shaping secondary social anxiety symptoms—that is, symptoms emerging in the context of depression—whereas in primary social anxiety disorder (SAD), reward processing may remain intact but be disrupted by avoidance tendencies. This distinction may help explain why anhedonia predicted social anxiety symptoms over time, but not vice versa. Our diagnostic data revealed that most participants with SAD and GAD at baseline met criteria for both previous and ongoing diagnoses, reflecting high comorbidity and chronicity. These patterns suggest that in the context of adolescent MDD, comorbid anxiety may reflect a more severe or entrenched symptom profile, in which anhedonia exerts a stronger influence on anxiety symptom trajectories. Thus, while anhedonia may broadly contribute to internalizing symptoms, its effects on anxiety may be more domain-specific—particularly for social anxiety, given the critical role of social reward processing in maintaining fear and avoidance. Future research should investigate whether these patterns differ in adolescents with primary anxiety disorders, where SAD or GAD are the principal presenting concerns, rather than disorders co-occurring with or following depression.
Clinical Implications
In light of our findings, there is a need for integrative approaches that target anhedonia in adolescents. Recent randomized clinical trials focusing on increasing positive affect and reward sensitivity in adult populations have demonstrated promising results in reducing stress, anxiety, and depression, surpassing the efficacy of traditional cognitive-behavioral interventions that primarily target negative affect (e.g., Craske et al., 2019, 2023); (McMakin et al., 2011); Taylor et al., (2017a, 2017b, 2024). While these interventions show promise, fewer studies have systematically tested similar approaches in adolescents. Emerging research suggests that interventions emphasizing positive emotional experiences—such as gratitude-based exercises, behavioral activation, and mindfulness—may be particularly beneficial in both clinical and school-based settings (Klos et al., 2020); Tejada-Gallardo et al., (Tejada-Gallardo et al. 2020); Owens & Waters, 2020). Even so, further research is needed to determine how these approaches can be optimally adapted for and implemented in youth populations. Given the distinct developmental challenges of adolescence, interventions tailored to enhance positive affect may serve as protective factors against stress while promoting mental health and resilience (Gilbert, 2012; Kansky et al., 2016); Sewart et al., 2019). Future work should focus on modifying and implementing reward-focused interventions in adolescent populations, identifying mechanisms of change, and evaluating their efficacy in improving co-occurring anxiety and depression symptoms across settings.
Limitations
One significant limitation of this study is that data collection occurred partly during the COVID-19 pandemic. A multidimensional stressor of unprecedented scale (Gruber et al., 2021), this context likely precipitated interpersonal stress, reflecting atypical developmental trajectories and potentially confounding self-reports of anxiety and depression severity (Magson et al., 2021). Consequently, the contextual influence of the pandemic on our results may limit generalizability to otherwise typical adolescent experiences. Additionally, the reliance on self-report measures may introduce biases. Future studies may benefit from incorporating complementary levels of measurement, such as neurophysiological indices (e.g., heart rate, cortisol levels, neuroimaging) and behavioral assessments (e.g., decision-making tasks, social interaction paradigms, clinician-rated measures), as these could be more informative in identifying mechanistic links between anhedonia and social anxiety, where longitudinal associations were observed. Further, investigating anhedonic and diminished positive experiences across multiple facets of hedonic function, such as anticipatory pleasure, consummatory pleasure, and motivation for reward (Rizvi et al.,(Rizvi et al. 2015), could provide a more comprehensive understanding of its role in the development and maintenance of social anxiety and depression. While our findings are interpreted within a framework of secondary social anxiety symptoms emerging in the context of MDD, we did not have data on the temporal onset of comorbid conditions. As such, we use the term “secondary” to reflect the structure of the sample—adolescents with MDD—rather than to indicate diagnostic primacy. Future studies that systematically assess onset order could clarify how the sequencing of depression and anxiety influences symptom dynamics and developmental trajectories. Finally, while findings suggest a temporal role of anhedonia predicting social anxiety, replication in larger samples is needed to derive reliable clinical implications.
Conclusions
We utilized a longitudinal sample of adolescents with ongoing or previous MDD followed longitudinally, allowing for a comprehensive understanding of clinical outcomes during a critical developmental period. Collectively, these results suggest that anhedonia may play a significant role in concurrent social anxiety and generalized anxiety symptoms in adolescent MDD, while also uniquely predicting social anxiety across time. These findings contribute to a growing body of literature on anhedonia in adolescent depression and as a transdiagnostic mechanism across mood and anxiety disorders. Additional research is necessary to replicate and extend the findings and to further inform interventions targeting emotional disorders in adolescents.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alden, L. E., & Taylor, C. T. (2010). Interpersonal processes in social anxiety disorder. Interpersonal processes in the anxiety disorders: Implications for Understanding psychopathology and treatment (pp. 125–152). American Psychological Association. 10.1037/12084-005
- 2Champely, S. (2020). pwr: Basic functions for power analysis (Version 1.3-0) Rpackage R package Rpackage. Retrieved from https://github.com/heliosdrm/pwr
- 3Fox, J., & Weisberg, S. (2019). An R companion to applied regression (3rd ed.). Sage. https://www.john-fox.ca/Companion/
- 4Haddow, S., Taylor, E. P., & Schwannauer, M. (2021). Positive peer relationships, coping and resilience in young people in alternative care: A systematic review. Children and Youth Services Review,122,. 10.1016/j.childyouth.2020.105861
- 5Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., Williamson, D., & Ryan, N. (1997). Initial reliability and validity data. Journal of the American Academy of Child and Adolescent Psychiatry, 36(7), 980–988. 10.1097/00004583-199707000-00021. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL).10.1097/00004583-199707000-000219204677 · doi ↗ · pubmed ↗
- 6Raudenbush, S. W., & Congdon, R. T. (2021). HLM 8: Hierarchical linear and nonlinear modeling. Scientific Software International, Inc.
- 7Revelle, W. (2024). psych: Procedures for psychological, psychometric, and personality research (Version 2.4.12) [R package]. Northwestern University. Retrieved from https://CRAN.R-project.org/package=psych
- 8R Studio Team (2024). R Studio: Integrated development environment for R [Computer software]. PBC. http://www.rstudio.com/