Association between serum phosphate levels and 28-day mortality in patients with sepsis-associated liver injury: a cohort study
Ting Ao, Yingxiu Huang, Peng Zhen, Ming Hu

TL;DR
Higher phosphate levels in blood at ICU admission are linked to higher 28-day death rates in patients with sepsis-related liver injury.
Contribution
Identifies serum phosphate as a novel independent predictor of mortality in sepsis-associated liver injury patients.
Findings
Higher phosphate levels at admission were significantly linked to increased 28-day mortality.
The association remained significant after adjusting for age, sex, comorbidities, and illness severity.
Subgroup analyses confirmed the consistent relationship between phosphate levels and mortality.
Abstract
Sepsis-associated liver injury (SALI) has a high mortality rate, but there is no established prognostic criterion for its outcomes. Although serum phosphate levels have been associated with mortality in several critical illnesses, research on their relationship with SALI is limited. This research aimed to explore the association between serum phosphate levels and 28-day mortality in SALI patients. We enrolled patients with SALI from the Medical Information Mart for Intensive Care-IV database. Serum phosphate levels were recorded within the initial 24 h of Intensive Care Unit admission. The primary outcome of interest was 28-day mortality. Multivariable Cox regression was applied to examine the association between serum phosphate and mortality. Additional subgroup analyses were carried out to ensure these findings. We analyzed data from 538 SALI patients, with a mean age of 69 years,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
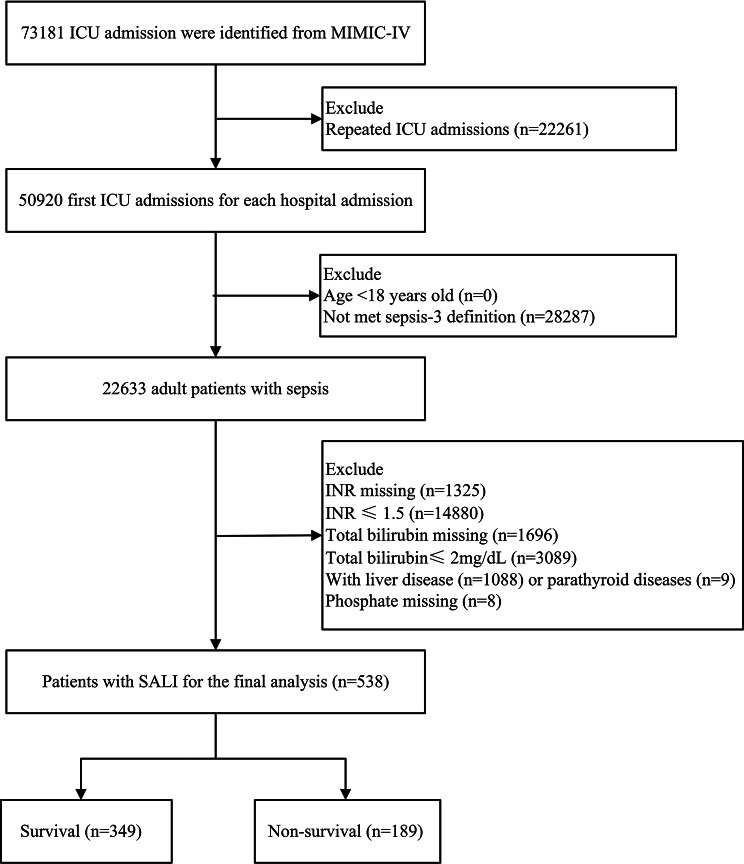 Figure 1
Figure 1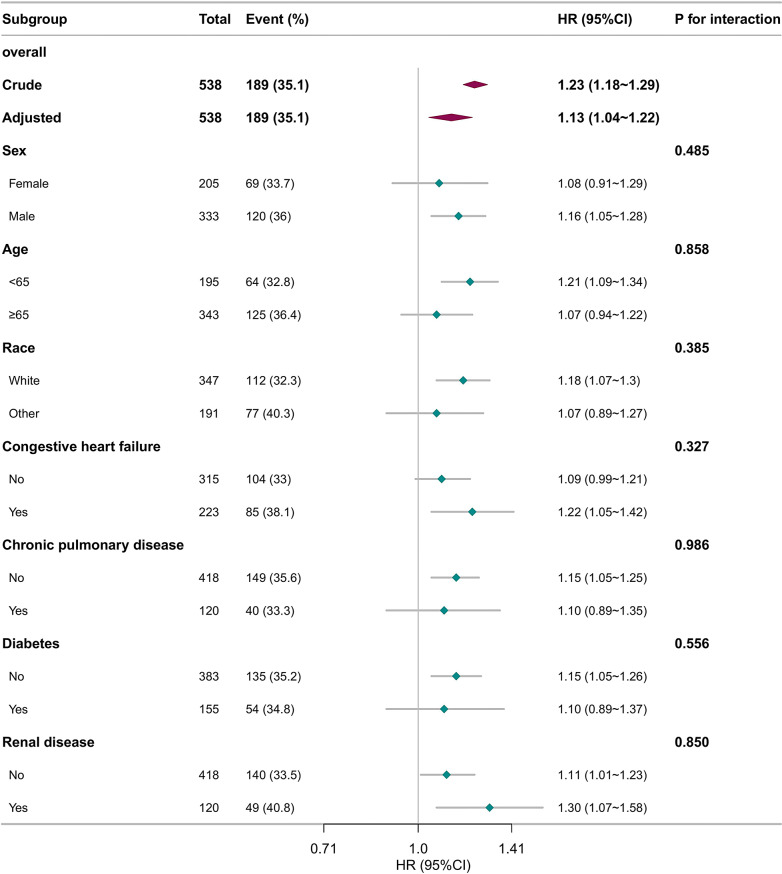 Figure 2
Figure 2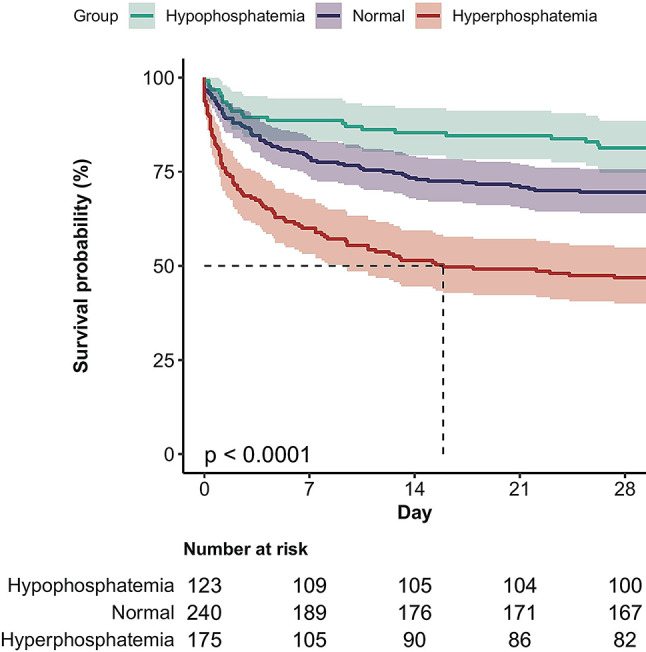 Figure 3
Figure 3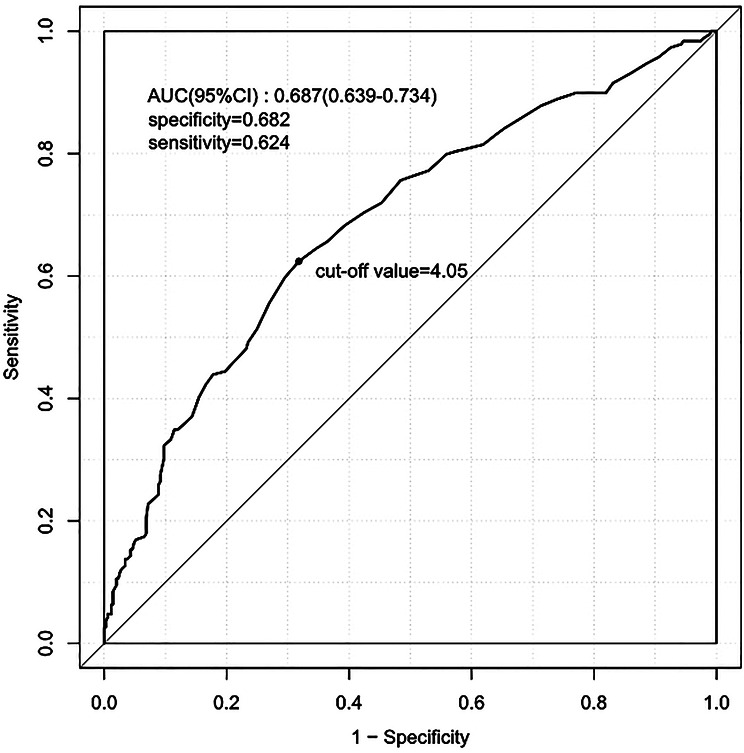 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Clinical Nutrition and Gastroenterology · Abdominal Surgery and Complications
Introduction
Sepsis is a critical state marked by organ impairment due to an inappropriate host response to infection [1]. Rudd et al. [2] reported that sepsis-related mortality is approximately 22.5%, contributing to 19.7% of global deaths. This high mortality rate imposes a significant economic burden. The liver, a central organ involved in detoxification, metabolism, and immune functions, is particularly susceptible to sepsis [3]. The development of sepsis-associated liver injury (SALI) involves a complex array of factors, including inflammatory responses, bacterial translocation, and oxidative stress [4, 5]. SALI is a crucial component of sepsis-induced multiple organ failure and is often linked with a poor prognosis [6]. Identifying effective prognostic markers is vital for the timely management of SALI.
Comprising about 1% of total body weight, phosphate ranks as the second most prevalent mineral in humans [7]. It is essential for various biological processes, including energy production, pH regulation in the blood, enzyme activation, and the function of organs such as the kidneys and immune system [8].
Several studies have demonstrated that abnormal serum phosphate levels are associated with adverse outcomes in critical illness. Hyperphosphatemia was an independent predictor of death in sepsis [9, 10]. Similar associations have been observed in patients with acute pancreatitis [11], severe burns [12], and COVID-19 [13], indicating that elevated phosphate is a consistent risk factor across diverse populations. The role of hypophosphatemia, however, remains controversial. Some studies suggested that it may serve as a marker of disease severity and is associated with an increased risk of mortality in critically ill patients [14]. Conversely, other reports described hypophosphatemia as protective, showing reduced mortality in septic patients [9, 15].
Importantly, previous studies have focused on general sepsis or critically ill populations, with no investigation specifically targeting patients with SALI, a subgroup characterized by distinct pathophysiological features and high mortality. Whether phosphate abnormalities are associated with mortality in SALI remains uncertain. To address this gap, we analyzed data from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database to examine the association between serum phosphate levels and 28-day mortality of SALI patients. Our findings provide novel insights into the prognostic significance of serum phosphate in this vulnerable group.
Materials and methods
Data sources and setting
Data for this investigation was sourced from the MIMIC-IV database, which provides comprehensive, de-identified electronic health records for Intensive Care Unit (ICU) admissions at Beth Israel Deaconess Medical Center (BIDMC) in Boston, MA, USA, spanning 2008–2019. Access was approved under certification number 58,844,105(First author: Ting Ao). Ethical approval was provided by the BIDMC Institutional Review Board, which waived the requirement for informed consent. The present cohort study adhered to the guidelines set forth by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [16].
Study population
The cohort included all ICU admissions in the MIMIC-IV database who were deemed eligible. We specifically focused on adult patients meeting the Sepsis-3 definition, defined as a Sequential Organ Failure Assessment (SOFA) score increase of at least 2 points attributable to infection-induced dysregulated host response. In accordance with the Surviving Sepsis Campaign guidelines, SALI was defined as total bilirubin level greater than 2 mg/dL and an International Normalized Ratio (INR) exceeding 1.5 in sepsis patients. These criteria are broadly accepted in published studies [17–20]. The analysis was restricted to patients who had serum phosphate levels recorded during the initial 24 h following ICU admission. Patients were excluded based on the criteria listed below: (1) patients aged less than 18 years; (2) repeated hospitalizations, excluding their first ICU admission; (3) missing phosphate data; (4) pre-existing parathyroid or liver diseases prior to sepsis onset.
Exposure
Serum phosphate levels measured within 24 h of ICU admission were used as the exposure factor. Individuals were divided into subgroups according to standard reference ranges for serum phosphate. According to the MIMIC-IV database, the reference range for normal serum phosphate levels was defined as 2.7 mg/dL to 4.5 mg/dL.
Covariates
Using Structured Query Language (SQL), patient data from the MIMIC-IV database were extracted and systematically recorded in PostgreSQL. At the onset of sepsis, we systematically gathered initial records, which included a wide array of physiological parameters: heart rate, mean blood pressure (MBP), respiratory rate, white blood cell count (WBC), platelet count, hemoglobin, glucose, potassium, sodium, blood urea nitrogen (BUN), creatinine, bicarbonate, total calcium, phosphate, and alanine aminotransferase (ALT). Additionally, we collected patient characteristics such as age, sex, race, SOFA score, and Charlson Comorbidity Index. Information on comorbidities, including renal disease, diabetes, chronic pulmonary disease, and congestive heart failure, was ascertained via International Classification of Diseases (ICD) code.
Outcome
The primary outcome was 28-day mortality. Secondary endpoints included in-hospital mortality, in ICU mortality, 90-day and 365-day mortality, and the number of ventilator-free, vasopressor-free, and ICU-free days during the initial 28-day period.
Statistical analysis
As this study is retrospective, the sample size was established according to the data accessible in the database. To handle missing data, we applied nearest neighbors’ imputation. Data are expressed as frequencies (percentages) for categorical variables and as means ± SD or medians (IQR) for continuous variables. Comparisons of continuous variables were performed using either Student’s t-test or the Wilcoxon rank-sum test according to distribution, and categorical variables were analyzed using Pearson’s chi-squared.
Variables included in the analysis were chosen based on clinical relevance and established findings in the literature [15, 21]. The impact of serum phosphate levels on 28-day mortality was assessed using multivariable Cox regression models, which yielded hazard ratios (HR) and 95% confidence intervals (CI) after adjusting for key covariates. Subgroup analyses were performed to explore potential interactions with relevant covariates and to address bias, including factors such as age, sex, race, and comorbidities. Kaplan–Meier survival curves were used to evaluate 28-day mortality across different phosphate level strata, with statistical significance determined by the log-rank test. Additionally, receiver operating characteristic (ROC) curves were generated, and the area under the curve (AUC) was calculated to evaluate the predictive performance of serum phosphate levels for 28-day mortality. Finally, sensitivity analyses were conducted: (a) excluding patients with renal diseases; (b) The Modification of Diet in Renal Disease (MDRD) study equation, which incorporates age, sex, race, and serum creatinine, was used to estimate glomerular filtration rate(eGFR) [22]. Then eGFR as a continuous covariate was included in the multivariable Cox regression models.
Analyses were performed using R Statistical Software (Version 4.2.2, http://www.R-project.org, The R Foundation) and Free Statistics software (Version 2.0, Beijing FreeClinical Medical Technology CO., Ltd, Beijing, China). A p-value of less than 0.05 in a two-sided test was regarded as statistically significant.
Results
Study cohort and patients’ characteristics
Following stringent screening based on predetermined inclusion and exclusion criteria, a total of 538 patients were deemed eligible for inclusion in the study (Fig. 1). Among these individuals, 349 were classified as survivors (survival group) and 189 as non-survivors (non-survival group). The mean age of the study population was 69 ± 16.7 years, with males comprising 333 (61.9%) of the total cohort. In the entire cohort, those in the non-survival group had higher SOFA score and charlson comorbidity index, and more likely to have greater serum phosphate level (Table 1).
Fig. 1. Flow chart of patient selection. Note: ICU, Intensive Care Unit; MIMIC-IV, Medical Information Mart in Intensive Care-IV; SALI, Sepsis-Associated Liver Injury; INR, International Normalized Ratio
Table 1. Baseline characteristics of participantsPatient characteristicTotal (n = 538)Survival (n = 349)Non-survival (n = 189) p Sex, n (%)0.575 Female205 (38.1)136 (39)69 (36.5) Male333 (61.9)213 (61)120 (63.5)Age(years), Mean ± SD69.0 ± 16.767.9 ± 17.570.9 ± 14.80.050Race, n (%)0.062 White347 (64.5)235 (67.3)112 (59.3) Other191 (35.5)114 (32.7)77 (40.7)Vital signs Heart rate (bpm), Mean ± SD93.9 ± 18.091.5 ± 16.898.3 ± 19.3< 0.001 MBP (mmHg), Mean ± SD74.6 ± 9.275.8 ± 8.772.6 ± 9.8< 0.001 Respiratory rate (bpm), Mean ± SD21.5 ± 4.420.9 ± 4.122.4 ± 4.7< 0.001Comorbidity disease, n (%) Congestive heart failure223 (41.4)138 (39.5)85 (45)0.222 Chronic pulmonary disease120 (22.3)80 (22.9)40 (21.2)0.640 Diabetes155 (28.8)101 (28.9)54 (28.6)0.928 Renal disease120 (22.3)71 (20.3)49 (25.9)0.138Score system Charlson comorbidity index, Median (IQR)6.0 (4.0, 8.0)6.0 (4.0, 7.0)7.0 (5.0, 9.0)< 0.001 SOFA score, Median (IQR)4.0 (3.0, 6.0)4.0 (3.0, 6.0)5.0 (4.0, 7.0)0.004Laboratory parameters Potassium (mmol/L), Mean ± SD4.2 ± 0.94.1 ± 0.84.5 ± 1.0< 0.001 Sodium (mmol/L), Mean ± SD137.8 ± 5.7137.9 ± 5.0137.6 ± 6.80.527 Bicarbonate (mmol/L), Mean ± SD19.9 ± 5.120.6 ± 4.918.5 ± 5.3< 0.001 Hemoglobin (g/dL), Mean ± SD10.6 ± 2.510.7 ± 2.510.2 ± 2.70.027 Total calcium (mg/dL), Mean ± SD7.9 ± 1.08.0 ± 1.07.9 ± 1.10.270 Creatinine (mg/dL), Median (IQR)1.4 (0.9, 2.1)1.2 (0.9, 1.7)1.8 (1.2, 2.7)< 0.001 BUN (mg/dL), Median (IQR)27.0 (17.0, 46.0)23.0 (15.0, 35.0)41.0 (23.0, 61.0)< 0.001 Glucose (mg/dL), Median (IQR)128.0 (101.0, 162.0)126.0 (102.0, 157.0)131.0 (98.0, 174.0)0.408 Platelets (K/uL), Median (IQR)146.0 (91.2, 205.8)146.0 (100.0, 204.0)145.0 (73.0, 209.0)0.331 WBC(K/uL), Median (IQR)13.5 (7.7, 20.0)13.5 (8.5, 20.0)13.7 (7.2, 19.9)0.328 Phosphate (mg/dL), Median (IQR)3.7 (2.7, 5.0)3.4 (2.5, 4.3)4.4 (3.5, 6.2)< 0.001 ALT (IU/L), Median (IQR)99.5 (34.2, 253.1)110.0 (35.0, 232.0)88.0 (31.0, 337.0)0.716Note: bpm, beats per minute; MBP, mean blood pressure; SD, standard deviation; IQR, interquartile range; SOFA, Sequential Organ Failure Assessment; BUN, blood urea nitrogen; WBC, white blood cell; ALT, alanine aminotransferase
Association between phosphate and 28-day mortality
The overall prevalence of 28-day mortality was determined to be 35.1%. The unadjusted multivariable Cox regression analysis indicated that elevated phosphate levels upon admission were significantly linked to higher 28-day mortality. (HR, 1.23; 95% CI, 1.18 to 1.29; p < 0.001; Table 2). After adjusting for age, sex, race, MBP, heart rate, respiratory rate, potassium, sodium, creatinine, BUN, bicarbonate, glucose, platelets, WBC, hemoglobin, total calcium, ALT, charlson comorbidity index, SOFA, renal disease, diabetes, chronic pulmonary disease, and congestive heart failure, the association between serum phosphate and 28-day mortality remained significant. Specifically, each 1 mg/dL increment in phosphate was associated with a 13% increase in 28-day mortality risk (HR, 1.13; 95% CI, 1.04 to 1.22; p = 0.006).
Table 2. Relationship between phosphate and 28-day morality in different modelsn. totaln. event(%)Model 1Model 2Model 3Model 4Model 5HR (95%CI)p valueHR (95%CI)p valueHR (95%CI)p valueHR (95%CI)p valueHR (95%CI)p valuePhosphate538189 (35.1)1.23 (1.18 ~ 1.29)< 0.0011.24 (1.19 ~ 1.31)< 0.0011.19 (1.13 ~ 1.26)< 0.0011.12(1.03 ~ 1.21)0.0071.13 (1.04 ~ 1.22)0.006Note: HR, hazard ratio; CI, confidence intervalModel 1: unadjustedModel 2: adjusted for sex, age, raceModel 3: adjusted for model 2 + heart rate, mean blood pressure, respiratory rateModel 4: adjusted for model 3 + potassium, sodium, creatinine, blood urea nitrogen, bicarbonate, glucose, platelets, white blood cell count, hemoglobin, total calcium, alanine aminotransferaseModel 5: adjusted for model 4 + charlson comorbidity index, Sequential Organ Failure Assessment, congestive heart failure, chronic pulmonary disease, diabetes, renal disease
Subgroup analyses
To explore potential effect modification, subgroup analyses were undertaken based on age, sex, race, and key comorbidities, including congestive heart failure, diabetes, chronic pulmonary disease, and renal disease, examining their influence on the association between serum phosphate and 28-day mortality. Subgroup analyses revealed no statistically significant interactions (p > 0.05, Fig. 2), suggesting a uniform effect of serum phosphate on 28-day mortality across different groups.
Fig. 2. Subgroup analyses for the association of serum phosphate with 28-day mortality in SALI patients. Note: Multivariate Cox proportional hazards models were adjusted for heart rate, mean blood pressure, respiratory rate, potassium, sodium, creatinine, blood urea nitrogen, bicarbonate, glucose, platelets, white blood cell count, hemoglobin, total calcium, alanine aminotransferase, charlson comorbidity index, Sequential Organ Failure Assessment score. SALI, Sepsis-Associated Liver Injury; HR, hazard ratio; CI, confidence interval
Kaplan-Meier survival curve analysis
According to the normal reference ranges, we categorized phosphate into three groups, hyperphosphatemia (phosphate > 4.5 mg/dl), normal (2.7 mg/dL-4.5 mg/dL) and hypophosphatemia (phosphate ≤ 2.7 mg/dl), and performed survival curve analysis. The 28-day cumulative survival rates were found to be lower in the hyperphosphatemia group than in the other groups, as shown by the Kaplan-Meier curve (log-rank test, p < 0.0001) (Fig. 3).
Fig. 3. Kaplan-Meier curve for 28-day mortality according to serum phosphate
ROC curve analysis
ROC analysis indicated that serum phosphate levels have a moderate clinical predictive value for 28-day mortality in SALI patients, with AUC of 0.687(95% CI: 0.639–0.734) (Fig. 4).
Fig. 4ROC curves of serum phosphate. Note: ROC, Receiver operating characteristic; AUC, Area under the curve
Secondary outcomes
Higher phosphate levels were also associated with increased in-hospital mortality (HR, 1.13; 95% CI, 1.03 to 1.22; p = 0.006), in-ICU mortality (HR, 1.12; 95% CI, 1.03 to 1.22; p = 0.009), 90-day mortality (HR 1.11; 95% CI, 1.02 to 1.20; p = 0.017), and 365-day mortality (HR 1.11; 95% CI, 1.02 to 1.20; p = 0.010). For every 1 mg/dL increment in phosphate level, ICU-free days decreased by 0.95 (95% CI, -1.53 to -0.38), ventilator-free days by 1.08 (95% CI, -1.70 to -0.45), and vasopressor-free days by 1.05 (95% CI, -1.68 to -0.41) over a 28-day period (Table 3).
Table 3. Secondary outcome analysisSecondary outcomesn. totaln. event (%)Crude modelAdjusted modelHR/β(95%CI)p-valueHR/β(95%CI)p-value90-day mortality^a^538226 (42.0)1.23 (1.17–1.28)< 0.0011.11 (1.02 ~ 1.20)0.017365-day mortality^a^538273 (50.7)1.22 (1.17–1.27)< 0.0011.11 (1.02 ~ 1.20)0.010In-hospital mortality^a^538169 (31.4)1.25 (1.20 ~ 1.31)< 0.0011.13 (1.03 ~ 1.22)0.006In-ICU mortality^a^538143 (26.6)1.26 (1.20 ~ 1.32)< 0.0011.12 (1.03 ~ 1.22)0.009ICU-free days until 28 days^b^538NA-1.87 (-2.30~-1.45)< 0.001-0.95 (-1.53~-0.38)0.001Vasopressor-free days until 28 days^b^538NA-2.02 (-2.48~-1.55)< 0.001-1.08 (-1.70~-0.45)0.001Ventilator-free days until 28 days^b^538NA-2.01 (-2.47~-1.54)< 0.001-1.05 (-1.68~-0.41)0.001^a^: Mortality outcomes are expressed as hazard ratios (HRs) with 95% confidence intervals (CI) derived from Cox regression models^b^: Ventilator-free days, vasopressor-free days, and ICU-free days until 28 days were presented as β coefficients (95% CI) from linear regression modelsCrude model was unadjustedAdjusted model was adjusted for sex, age, race, heart rate, mean blood pressure, respiratory rate, potassium, sodium, creatinine, blood urea nitrogen, bicarbonate, glucose, platelets, white blood cell count, hemoglobin, total calcium, alanine aminotransferase, charlson comorbidity index, Sequential Organ Failure Assessment, congestive heart failure, chronic pulmonary disease, diabetes, renal disease
Sensitivity analyses
After excluding patients with renal disease, the association between serum phosphate and 28-day mortality in SALI remained consistent. Following adjustment for potential confounders (excluding renal disease), a 1 mg/dL rise in phosphate was linked to a 12% increase in 28-day mortality risk (95% CI, 1.01–1.23; P = 0.025; Supplementary Table 1). In addition, MDRD study equation was used to calculate eGFR). Then eGFR was adjusted in the fully adjusted model. The results remained robust(HR 1.11; 95% CI, 1.02–1.21; P = 0.012; Supplementary Table 1).
Discussion
Elevated serum phosphate levels were significantly associated with a greater risk of 28-day mortality in SALI patients, according to the study results. This relationship was consistently observed across various subgroup analyses. Additionally, hyperphosphatemia was associated to a heightened risk of both in-ICU and hospital mortality.
Phosphate is essential for various physiological functions, including oxygen transport, homeostasis, and cellular metabolism [10, 23]. Imbalances in serum phosphate levels, including hypophosphatemia and hyperphosphatemia, can adversely affect health and are associated with poor outcomes. Research has increasingly focused on the clinical relevance of serum phosphate. Guo et al. [10] demonstrated that every 1 mg/dL rise in serum phosphate was linked to a 19% increase in 30-day mortality risk of sepsis (95%CI,1.13 to 1.26). Elevated phosphate levels have also been linked to higher risks of hospital and ICU mortality, while hypophosphatemia was found to be protective [21]. Consistent with prior research, our study demonstrated a significant positive association between serum phosphate and 28-day mortality in patients with SALI.
However, the association between abnormal phosphate levels and outcomes in critical ill patients remains contentious. A retrospective cohort analysis found a U-shaped relationship between serum phosphate and long-term primary cardiac disease risk, with hypophosphatemia potentially increasing the risk [24]. Another research suggested hypophosphatemia was an independent risk factor for 28-day ICU mortality (adjusted odd ratio, 1.5; 95% CI, 1.1 to 2.1; P = 0.01) [14]. Conversely, a systematic review and meta-analysis found no significant association between pre-intervention hypophosphatemia and increased mortality risk (relative risk,0.97; 95% CI, 0.86–1.09; P = 0.588) [25]. Our study found that hypophosphatemia was associated with lower 28-day mortality in patients with SALI. Variations in patient cohorts, the timing of measurements, and the thresholds used to define abnormal phosphate levels could account for these differences.
The detailed mechanism through which phosphate impacts the prognosis of SALI continues to be uncertain. Excessive phosphate levels can lead to toxic effects that contribute to damage in various organs, including the liver. Phosphate has been connected to both inflammatory reactions and oxidative stress, as well as cytotoxic effects [26]. Elevated phosphate levels have been identified as an independent risk factor for inflammatory conditions and are positively associated with traditional inflammatory markers, including C-reactive protein and interleukin-6 [27]. Furthermore, oxidative stress, driven by phosphate, plays a critical role in organ injury [28, 29]. The interplay of excessive oxidative stress and inflammatory responses, combined with endothelial and epithelial damage from infection, can lead to sepsis-associated organ dysfunction [30]. The liver is particularly susceptible to this combined damage from sepsis and phosphate toxicity. Due to the retrospective nature of this observational study, the causal mechanisms underlying the observed associations cannot be determined. Additional studies are needed to explore these mechanisms and to better understand the contribution of phosphate to hepatic injury in sepsis.
Our investigation exhibits several notable advantages. Firstly, it represents one of the first systematic investigations into the link between serum phosphate levels and mortality in patients with SALI. Secondly, we accounted for a range of potential confounding factors, including renal dysfunction and parathyroid disorders. Recognizing that these conditions can markedly affect serum phosphate levels, we removed patients with parathyroid disorders and adjusted for renal conditions in our analysis. Furthermore, we controlled for other relevant variables such as vital signs, laboratory results, and comorbidities within our Cox regression models.
Despite these advantages, several limitations warrant careful consideration and cautious interpretation of our findings. Firstly, despite controlling for known confounders, the retrospective nature of our study inherently leaves room for unidentified confounders that could impact our results. Secondly, the study’s sample size might be inadequate, potentially introducing small sample bias and selection bias. Thirdly, our study design does not allow for establishing causality between serum phosphate levels and mortality. Moreover, due to the fluctuating nature of serum phosphate, a single measurement might not provide a comprehensive view of its link to mortality over time.
Conclusion
This study demonstrated that elevated phosphate levels upon ICU admission are independently linked to a higher risk of 28-day mortality in patients with SALI. These results suggest that serum phosphate may serve as a potential prognostic marker for SALI; however, prospective studies are required to validate its clinical utility. Future research should aim to confirm these findings and investigate the mechanisms through which phosphate affects mortality in this context.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1