Neither uni- nor multi-modal exercise interventions improved single- and dual-task gait performance in physically active healthy elderly – a pilot study
Constantin W. Freitag, Martin Behrens, Robert Bielitzki, Tom Behrendt, Khaldoon O. Al-Nosairy, Francie H. Stolle, Gokulraj T. Prabhakaran, Rosalie Beyer, Cynthia Moffack Djuloun, Hagen Thieme, Michael B. Hoffmann, Lutz Schega

TL;DR
A 12-week study found that neither combined nor single resistance training improved walking or cognitive performance in active older adults, despite increased strength.
Contribution
This pilot study compares multimodal and unimodal exercise interventions on gait and cognitive performance in elderly individuals.
Findings
Neither multimodal nor unimodal interventions improved gait parameters in elderly participants.
Cognitive performance did not improve after either type of intervention.
Resistance training increased external load, suggesting neuromuscular adaptations, but no functional gains in gait or cognition.
Abstract
Aging is an inevitable process leading, inter alia, to the loss of muscle mass as well as the decrease in physical and cognitive function. These age-related impairments translate into a reduced gait performance and an increased risk of falls, which can be tackled with resistance training, Unimodal intervention (UMI). However, Multimodal intervention (MMI), i.e. combined motor-cognitive and resistance training, might be a more promising approach to increase physical and cognitive function in old adults. Therefore, this pilot study aimed to investigate the effects of MMI, compared to UMI, on gait and cognitive performance in elderly participants. We hypothesized that MMI will increase gait and cognitive performance to a larger extent than UMI. In this two-arm randomized controlled pilot study, 24 healthy active elderly participants completed the MMI (12 participants, 72.6 ± 5.4 years)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
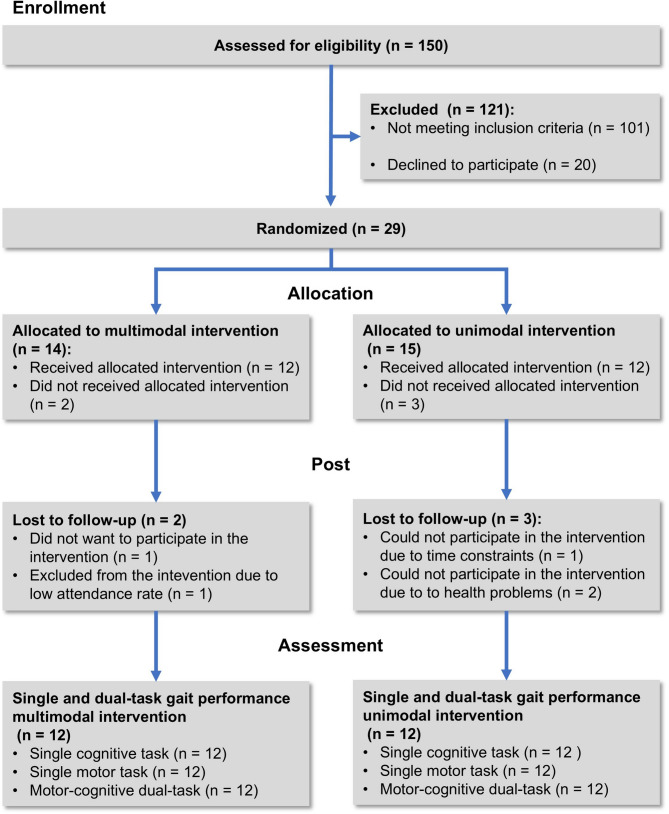 Figure 1
Figure 1- —Otto-von-Guericke-Universität Magdeburg (3121)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBalance, Gait, and Falls Prevention · Motor Control and Adaptation · Physical Activity and Health
Introduction
Aging is a continuous process resulting in, inter alia, skeletal muscle atrophy (sarcopenia) [1] and a reduction in neural drive to the muscles finally causing a decline in maximal and explosive muscle strength (dynapenia) [2, 3] and function. Moreover, aging might impair cognitive functions including decreased executive functions [4]. Both the age-related decline in physical and cognitive function can affect daily activities by deteriorating gait performance and increasing the risk of falls [5, 6], a major cause of injuries in the elderly [7].
Several spatiotemporal gait parameters, such as stride length, gait velocity, and gait variability measures have been shown to be predictive for the risk of falls [8, 9]. In particular, the minimum toe clearance (MTC) appears to be a promising marker for evaluating walking performance and perhaps the risk of falling in older adults [10]. The MTC describes the smallest distance between the ground and toe during the mid-swing phase of the gait cycle [8] and the lower the MTC and the larger its variability, the higher the risk of sustaining a fall [10]. Gait performance, i.e., motor function and control during walking, is often evaluated during motor-cognitive dual-task walking [11–16], which is characterized by performing a concurrent cognitive task during walking and often results in increased gait variability measures [8, 17]. The worsening of gait performance might be attributable to the reduced processing capacity for the motor task (central capacity sharing model) and/or the sequential neural processing of the motor and cognitive interference task (bottleneck model) [18]. Consequently, performance in at least one task diminishes, e.g., gait performance, a phenomenon known as dual-task costs (DTC). This is of particular importance, given that daily activities often require multitasking, such as walking while thinking, texting, or phoning. Importantly, a lower motor-cognitive dual-task walking performance, i.e., higher DTC, is related to a higher risk of falling [19].
Since falls can lead to fear of future falls [20], a loop of physical inactivity might begin promoting sarcopenia, dynapenia, as well as cognitive dysfunction [21], and thus, increasing the risk of falling. To counteract this, resistance training promises a suitable interventional strategy to increase neuromuscular function and functional performance in older adults [6]. In this regard, resistance training has been shown to increase postural control and gait performance in elderly [22]. Furthermore, resistance training might also have positive effects on cognitive performance due to functional (e.g., in the frontal lobe) and structural brain adaptations (e.g., lower white matter atrophy and smaller white matter lesion volumes) [23].
Further, there is evidence that motor-cognitive dual-task training (i.e., the concurrent execution of motor and cognitive tasks) [24] elicits structural and functional changes in the aging brain, which were associated with an improved cognitive performance [25–28]. Although the evidence is inconclusive, concurrent training of motor and cognitive tasks might be a more promising approach for enhancing cognitive performance compared with single motor or cognitive training [13, 29]. Given that both, the age-related decline in strength and cognitive function, have an impact on gait performance, a multimodal intervention (MMI) combining resistance training and motor-cognitive dual-task training [24] could be more effective in improving gait performance (e.g., stride length, gait velocity, MTC and their variability) than resistance training alone. This is of relevance, since these gait measures [8–10], especially recorded during dual-task walking [19], have been shown to be predictive for the risk of falls. Therefore, improving gait performance with MMI might be a promising approach for fall prevention in older adults.
As far as the authors of the present study are aware, there is no experimental trial that has investigated the effect of a stand-alone resistance training compared to a motor-cognitive dual-task training directly followed by a resistance training intervention on gait and cognitive performance in healthy elderly. Therefore, the present study compared the influence of a 12-week MMI (motor-cognitive dual-task training + resistance training) and a unimodal intervention (UMI, stand-alone resistance training, twice a week, lasting 60 min each, 24 training sessions in total) on gait performance and cognitive performance in healthy old adults. For that purpose, gait parameters (i.e., stride length, gait velocity, MTC), and their respective coefficient of variation (CoV) [8] were recorded during single-task and motor-cognitive dual-task walking before and after the training intervention. Additionally, the DTC (relative changes between single-task and dual-task performance) were calculated to assess the cognitive demands during walking [30].
It was hypothesized that the MMI leads to higher improvements in gait performance, especially during dual-task walking, and cognitive performance compared to UMI. Furthermore, a decrease in DTC was expected after the MMI.
Methods
Study design
This two-arm randomized controlled pilot study was conducted from August 2020 to December 2022. The interventions and measurements were performed in the laboratories of the Sport Science Department at the Otto von Guericke University Magdeburg. The study was carried out in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University Medical Faculty Magdeburg (32/18). Reporting was performed in accordance with the Consolidated Standards of Reporting Trials (CONSORT) Statement for randomized pilot trials [31]. The data presented in this article are part of a larger study investigating the effects of a MMI versus UMI on visual, motor, and cognitive performance as well as structural and functional brain adaptations in glaucoma patients and healthy controls (German Clinical Trial Register, ID: DRKS00022519/05.08.2020, https://drks.de/search/de/trial/DRKS00022519). All participants signed the informed consent form before participating in this study.
Participants
As mentioned above, the present data are secondary outcomes of a larger randomized controlled trial focusing on functional brain connectivity as the primary outcome. Therefore, the sample size is based on the study by Demiracka and colleagues [32], who reported significant effects of the Life Kinetik^®^ intervention (n = 21) on functional brain connectivity compared to a control group (n = 11). It should be noted that the data-acquisition/funding epoch coincided with the COVID-19 pandemic, such that the total of 24 participants was the maximum possible. Recruitment process was conducted at the Department of Ophthalmology at the University Hospital Magdeburg via the local newspaper. Participants were eligible when they met the following inclusion criteria: (i) age ≥ 60 and (ii) the ability to walk at least six minutes without support. Exclusion criteria were defined as follows: (i) eye diseases/surgeries affecting visual function, (ii) neurological disorders, (iii) rheumatism, (iv) cardiovascular disorders, (v) stroke, (vi) orthopedic diseases including arthrosis (grade II or higher), musculoskeletal impairment, tendinitis, tenosynovitis, myositis, prosthesis in the lower extremities, and joint replacements. The allocation was performed at the Department of Sport Science. Participants gave their informed consent to voluntarily participate in the present study and were randomly assigned to either the MMI or the UMI using counterbalanced randomization (allocation ratio was 1:1) by a computer-generated table of random numbers (Fig. 1). For participant characteristics see results.
Fig. 1. Study schedule of enrollment, intervention, and assessments
General procedure
All outcomes were assessed during a period of three weeks before and after the interventions, respectively. The assessors of the measurements were not blinded to the group allocation because they also supervised the interventions.
At the beginning of the measurements, participants signed the informed consent and were given the Freiburger Questionnaire on Physical Activity [33] to assess the level of physical activity. Furthermore, age, height, and weight of each participant were recorded. The complete testing procedure including the methods for recording and calculating the spatiotemporal gait parameters have been described in detail by Freitag et al. [30]. Briefly, over two consecutive days, participants performed single-tasks (at the beginning of each day) and three dual-task walking tasks at individuals’ comfort velocity over a 10 m track back and forth for 180 s, respectively. The dual-task walking tasks were conducted in a random order and in this regard, one was performed on day one and the other on day two.
During dual-task walking, the participants performed three cognitive tasks: (i) reaction time task, (ii) N-back-task, and (iii) letter fluency task with two levels of difficulty, respectively. Additionally, all cognitive tasks were performed as a separate single-task to calculate DTC for cognitive performance. DTC for gait performance were calculated using the single-task and dual-task walking performance.
Spatiotemporal gait parameters (stride length, gait velocity, MTC) and their respective CoV (CoV = 100 x standard deviation/mean) were assessed using inertial measurement units (XSENS MTW Awinda, Movella, Delft, Netherlands; sampling frequency 100 Hz) placed proximal on each foot and the sternum. The gait parameters were calculated using the algorithm developed by Hamacher et al.^8^. Due to the corona virus pandemic, participants were advised to wear a FFP2 face mask.
Intervention
Both intervention groups completed a 12-week training program with two sessions per week (i.e., a total of 24 sessions) on non-consecutive days. Each exercise session lasted 60 min and was guided by experienced instructors.
The MMI was split into the following sequences: (i) motor-cognitive training based on the Life Kinetik^®^ program [34] and (ii) resistance training. The Life Kinetik^®^ program consisted of simultaneously performed motor-cognitive dual-tasks. The progression of the exercises followed a standardized schedule. They were designed to be complex and intense enough to ensure that successful completion is initially unattainable. If the exercises were performed correctly in 6 out of 10 trials, the instructor introduced a more advanced variation of the exercise [34]. The training sessions included exercises such as: (i) balls with different colors (e.g., yellow, green, red) were thrown in a circle, whereby a corresponding name must be said for each color (e.g., yellow = persons own name, green = name of the person to whom the ball has to be thrown. (ii) Participants stand next to each other. After an announcement (e.g., left, right, front, back) the participants walked in the corresponding direction (line of vision remained the same, i.e., no turning of the body), whereby the corresponding name for each direction was varied (e.g., right = 1, left = 2, front = 3, back = 4). The duration of the motor-cognitive training and the resistance training varied from month to month (Table 1). The duration was increased and the exercises changed every month with weekly variations from the beginning of the 2th month resulting in a progressive reduction in the time for the resistance training.Table 1MMI training scheduleTraining componentsMonths 1 st Month2nd Month3th MonthLife Kinetik^®^10 min20 min30 minResistance Training40 min30 min20 minCool Down10 min10 min10 min
The UMI consisted of nine exercises. Prior to the main exercises, a 10-minute standardized warmup was performed containing fast walking and dynamic stretching of the upper and lower extremities. The resistance exercises were performed using free weights and exercise machines in a fixed order. Subjects had to perform 2 sets with 7 repetitions of each exercise using an external load (i.e., weight) that corresponded to a moderate to somewhat severe (3–4) rating on a perceived exertion (RPE) scale (Borg scale, 1–10) [35]. The exercises were metronome paced at a cadence of 30 bpm (i.e., 2 s concentric/2 s eccentric).
Both interventions were completed with a cool down of 10-min static stretching for the major muscle groups (e.g., standing side stretch, standing forward fold, overhead triceps stretch).
Due to the fact that this intervention was part of a larger study investigating the effects of a MMI versus UMI on visual, motor, and cognitive performance as well as structural and functional brain adaptations in glaucoma patients, all exercises were performed while sitting or standing because exercising in a supine position affects the intraocular pressure [36, 37], which represents a major risk factor of open angle glaucoma [38]. From the second month of the intervention period, both intervention groups trained with two training plans that were performed alternately. A detailed overview of the training program with exercise variables is provided in the Table 2. The participants were allowed to continue with their usual physical activities.
Table 2. Overview of the resistance training for the unimodal intervention and multimodal intervention throughout the intervention period. Letter in brackets indicate the major muscles involved in the exercise according to Haff and triplett (2016) [39]WeekUnimodal InterventionMultimodal InterventionMajor Muscles InvolvedWeeks 1–41. Seated leg press (A)2. Lever Pulldown (B)3. Lever seated twist (C)4. Lever chest press (D)5. Cable curl (E)6. Lever back extension (F)7. Cable pushdown (G)8. Cable upright row (H)9. Seated leg curl (I)1. Seated leg press (A)2. Lever Pulldown (B)3. Lever seated twist (C)4. Lever chest press (D)5. Cable curl (E)6. Lever back extension (F)7. Cable pushdown (G)8. Cable upright row (H)9. Seated leg curl (I)A. Gluteus maximus, Semimembranosus, Semitendinosus, Biceps femoris, Vastus lateralis, Vastus intermedius, Vastus medialis, Rectus femorisB. Latissimus dorsi, Teres major, Middle trapezius, Rhomboids, Posterior deltoidsC. External abdominal oblique, Internal abdominal obliqueD. Pectoralis major, Anterior deltoids, Triceps brachiiE. Biceps brachii, Brachialis, BrachioradialisF. Erector spinaeG. Triceps brachiiH. Deltoids, Upper trapeziusI. Semimembranosus, Semitendinosus, Biceps femorisJ. Vastus lateralis, Vastus intermedius, Vastus medialis, Rectus femorisK. DeltoidsL. Latissimus dorsi, Triceps brachiiWeeks 5–8Day 11. Seated leg press (A)2. Cable straight back seated row (B)3. Lever seated twist (C)4. Lever chest press (D)5. Cable curl (E)6. Lever back extension (F)7. Cable pushdown (G)8. Cable upright row (H)9. Lever leg extension (J)1. Seated leg press (A)2. Cable straight back seated row (B)3. Lever seated twist (C)4. Lever pec dec fly (D)5. Cable upright row (H)6. Cable curl (E)Day 21. Seated leg press (A)2. Lever pulldown (B)3. Lever seated twist (C)4. Lever pec dec fly (D)5. Reverse cable curl (E)6. Lever back extension (F)7. Cable pushdown (G)8. Dumbell seated lateral raise (K)9. Seated leg curl (I)1. Cable pushdown (G)2. Lever pulldown (B)3. Lever back extension (F)4. Lever chest press (D)5. Dumbbell seated lateral raise (K)6. Seated leg curl (I)Weeks 9–12Day 11. Seated leg press (A)2. Cable straight back seated row (B)3. Lever chest press (D)4. Lever seated twist (C)5. Cable Curl (E)6. Dumbbell seated front raise (K)7. Seated leg curl (I)8. Lever back extension (F)9. Cable pushdown (G)1. Seated leg press (A)2. Dumbbell seated front raise (H)3. Reverse cable curl (E)4. Lever chest press (D)5. Lever seated twist (C)Day 21. Seated leg press (A)2. Cable seated straight arm pulldown (L)3. Lever seated twist (C)4. Lever pec dec fly (D)5. Reverse cable curl (E)6. Seated triceps press (G)7. Dumbbell seated lateral raise (K)8. Lever leg extension (J)9. Lever back extension (F)1. Seated leg curl (I)2. Lever pec dec fly (D)3. Lever back extension (F)4. Seated triceps press (G)5. Cable seated straight arm pulldown (L)
Motor and cognitive dual-task costs
DTC were calculated as follows:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:\begin{array}{c}DTC=\frac{Single\:task-Dual\:task}{Single\:task}\times\:100\end{array}$$\end{document} \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:\begin{array}{c}DTC=\frac{Dual\:task-Single\:task}{Dual\:task}\times\:100\end{array}$$\end{document}Single task and Dual task are the single- and dual-task performance, respectively. Equation (1) was used when a higher measurement value reflected a better performance. Otherwise, when a lower measurement value reflected a better performance, equation (2) was used. Hence, positive values indicate higher DTC, while negative values reflect a better Dual task performance compared with the Single task performance.
Statistical analysis
Data were analyzed using the JASP Statistics (Version 0.19.3.0, University of Amsterdam, Amsterdam, Netherlands). Differences between groups in the anthropometric data were checked, depending on distribution of normality, with independent t-tests or Mann-Whitney test. Since previous studies have shown that repeated measures analysis of covariance (ANCOVA) to be robust against moderate violation of normality [40], nonparametric tests were not used to check for differences. Consequently, a three-way repeated measures ANCOVA with the factors INTERVENTION (MMI vs. UMI), CONDITION (single- vs. dual-task), and TIME (pre vs. post) was conducted. Due to difference in distribution of sex between groups it was used as covariate. If a violation of sphericity was detected, the Greenhouse-Geisser correction was applied. To interpret the results and to clarify the practical/clinical relevance of interventional studies it is advisable to use effect sizes [41]. Thus, the effect size partial-eta squared ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} ) as well as Cohen’s d (d) were calculated and interpreted according to Lakens [41]: small ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} ≥ 0.01, d ≥ 0.2), medium ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} ≥ 0.06, d ≥ 0.5), and large ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} ≥ 0.14, d ≥ 0.8). In case of TIME x INTERVENTION x CONITION or TIME x INTERVENTION effects as well main effects of TIME, Bonferroni-corrected post-hoc tests were performed. In case of large main effects, the results were interpreted as relevant if \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} ≥ 0.14 or d ≥ 0.8. Due to pilot character of the present study, a sample size calculation, based on the observed effect sizes, was conducted (G*Power 3.1.9.7, Heinrich Heine University Düsseldorf, Düsseldorf, Germany) to provide data on sufficient sample sizes for future randomized controlled trials. In addition, a two-way repeated ANOVA was performed with the factors INTERVENTION (MMI vs. UMI) and TIME (first, second, and third month) to analyze the progression of the external load during the resistance training (i.e., leg press, seated leg curls) as an indirect marker of neuromuscular adaptations, which could have an impact especially on the spatiotemporal gait parameters. The external load per exercise was averaged over each month.
Results
Characteristics of participants
In total, 29 healthy participants were recruited. Fourteen participants (8 females, age: 71.9 ± 5.4 years, height: 164.1 ± 8.5 cm, body mass: 72.3 ± 22.6 kg) received the MMI and 15 participants (9 females, age: 70.3 ± 5.0 years, height: 170.7 ± 9.9 cm, body mass: 78.1 ± 11.9 kg) received the UMI. The Freiburger Questionnaire on Physical Activity [33] indicated that overall physical activity was on average 10.8 h for the MMI group and 15.7 h per week for the UMI group. All participants had an attendance rate of at least 80%. Due to dropouts only data from 24 participants (12 MMI, 12 UMI) were included in the final analysis. Due to processing issues regarding the MTC and the MTC_CoV_, only 23 participants (11 MMI, 12 UMI) were included in the final analysis. Furthermore, due to technical issues during the single-task walking trial at baseline measurement only 21 participants (11 MMI, 10 UMI) were included into the final DTC analysis. Moreover, due to an extreme outlier during the N-Back task at the baseline measurement only 23 participants (12 MMI, 11 UMI) were included into the final (DTC) cognitive performance analysis. The results of the sample size calculations are presented in supplementary Table A and B. An overview of all parameters including the p-values and effect sizes is presented in supplementary Tables C-E).
Outcome measures
No relevant interactions and main effects were found for gait velocity, stride length, MTC, and their respective CoVs (Supplementary table C) as well as for cognitive performance (Supplementary table E). (Supplementary table D).
The analysis of the external load progression showed a TIME x INTERVENTION interaction for leg press (F(1.253,27.569) = 6.219, p = 0.014 \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} = 0.221). Post-hoc analysis showed a significant higher external load for the UMI compared to the MMI during the 2nd month (p = 0.023, d = 0.955, mean difference = 15.667 kg, 95% CI = 2.329–29.004%, 95% CI for d = 0.420–2.330) and the 3rd month (p = 0.014, d = 1.270, mean difference = 20.833 kg, 95% CI = 4.695–36.972%, 95% CI for d = 0.414–2.954).
Further, TIME effects were detected for leg press (F(1.253.27.569) = 46.361, p < 0.001, \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} = 0.678) and seated leg curls (F(1.305,28.705) = 21.194, p < 0.001, \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{{\upeta\:}}_{\text{p}}^{2}$$\end{document} = 0.491). Post-hoc analysis showed a significant increase in external load over the three months for the leg press: 1 st and 2nd month (p < 0.001, d = 0.498, mean difference = −8.167 kg, 95% CI = −11.136 - −5.197, 95% CI for d = 0.764 − 0.232), 2nd and 3rd month (p < 0.001, d = 0.254, mean difference = −4.167 kg, 95% CI = −6.492 - −1.841%, 95% CI for d = 0.427 − 0.081). Furthermore, the post-hoc analysis showed an increase in external load between the 1 st to 2nd months for the leg curl (p < 0.001, d = −0.436, mean difference = −2.729 kg, 95% CI = −4.296 - −1.163%, 95% CI for d = 0.739 − 0.133) and 2nd to 3rd month (p = 0.037, d = 0.147, mean difference = −0.917 kg, 95% CI = −1.788 - −0.046, 95% CI for d = 0.297 − 0.004).
Discussion
The present pilot-study investigated the effect of a 12-week MMI versus UMI on spatiotemporal gait parameters recorded during single- and dual-task walking as well as cognitive performance in healthy older adults. Contrary to our hypothesis, both training interventions failed to improve gait parameters, their respective CoVs, cognitive performance as well as motor and cognitive DTC. Nevertheless, both interventions provoked progress regarding the external load during the training period indicating increased strength capabilities due to training-induced neuromuscular adaptations.
The results of the present study revealed that none of the two interventions positively influenced gait or cognitive performance. This finding is surprising given that positive intervention effects on the dependent variables (e.g., stride length, gait velocity, MTC and their variability) were expected for both the UMI and MMI in healthy elderly. To the knowledge of the authors, no previous study has investigated the influence of a comparable MMI on gait performance, cognitive performance, as well as motor and cognitive DTC in healthy elderly participants. However, Wollesen et al. [42] showed that a progressive stand-alone resistance training and dual-task training (e.g. fast walking in combination with visual and balance tasks, 12 sessions, 60 min, 12 weeks) led to an improved gait performance in healthy elderly participants (i.e., increased step length). Furthermore, Singh et al. [43] demonstrated that a resistance training (2–3 days/week, 75 min, 24 weeks) increased cognitive performance in patients with mild cognitive impairment. Moreover, Castano et al. [44] showed that combining resistance training with a verbal fluency task (2 days/week, 60 min, 16 weeks) enhanced plasma brain-derived neurotrophic factor level, which is associated with cognitive performance, compared to traditional resistance training in healthy elderly participants.
It could be assumed that the external load used during resistance training, which was prescribed based on the RPE, might have been too low to induce neuromuscular adaptations translating in an improvement in gait performance [6]. In this regard, it should also be considered that both intervention groups had a high physical activity (10.8 h/week and 15.7 h/week, respectively), which is above the average compared to the same age (≥ 70 years, 9.9 h/per week [33]). On top of that, ST gait velocity of participants of the present study (1.26 m/s) was above the average of elderly without gait impairments (1.05 m/s) [45]. These factors suggest a potential ceiling effect, whereby participants’ high baseline activity may have limited the observable benefits of the intervention. Speculatively, the absence of improvements in gait performance due to the resistance training in both intervention groups might follow the law of diminishing returns, meaning that potential adaptations decrease with a higher fitness level [46].
Of note, the lower exercise intensity during resistance training was deliberately chosen to obtain reference data from normal participants for a companion investigation with patients with glaucoma. The present study was part of a larger randomized controlled trial investigating the effect of a MMI compared to a UMI in glaucoma patients, for which this approach was selected to keep intraocular pressure low [47]. Nevertheless, the analysis of the training progression using the external load data revealed an increase in external load over the three months period indicating neuromuscular adaptations. Although this analysis is only a crude measure of training-related strength increases, the potential neuromuscular adaptations have not led to improvements in gait performance.
Against our hypothesis, gait and cognitive performance were also not altered after the MMI. In this regard, Hamacher and colleagues [13] have shown that a six-month dancing program, which also requires the incorporation of cognitive demands into the motor task [48], significantly reduced the MTC_CoV_ compared to a combined exercises intervention in older adults (e.g., endurance training, strength training, flexibility training). This finding might be related to the fact that dancing requires the incorporation of cognitive demands into the motor task [48]. In contrast, in the Life Kinetik^®^ program, the cognitive tasks are used as distractors (additional) during the motor tasks and are thus not directly relevant for motor task completion [24]. Consequently exercises in which the cognitive task is a prerequisite for the motor task execution, might be better suited to improve gait performance compared to exercises using the cognitive task as a distractor during the motor task [24].
The present study has some limitations. First, single-task walking was always conducted before dual-task walking, which might have promoted sequential effects. However, the possible sequential effects were systematic as well as stable and might therefore have not affect group comparisons. Second, the sensitivity of the calculated gait parameters might be too low to detect differences in the dependent variables in our healthy elderly cohort. For instance, Kulmala et al. (2014) have shown that joint power of the lower extremities during walking are affected by age and shift from distal to proximal [49]. Therefore, it might be possible that other gait measures are more sensitive to the interventions used in healthy elderly people. However, it was shown that the calculated gait parameters are sensitive to differentiate between glaucoma patients and healthy controls (e.g., slower gait velocity [50] and higher MTC_CoV_ [30] in glaucoma patients). Third, the lack of improvements in gait performance might be due to a lack of isolated training of the triceps surae muscle, which is essential for plantar flexion and propulsive torque production during walking [51, 52]. This muscle group is also affected by the aging process resulting in shorter steps and a higher power production in the hip and knee joints [49]. Moreover, the triceps surae muscle is also important for remaining gait stability after stumbling [53]. Therefore, an increase in exercises dedicated to the plantar flexors is warranted, which might lead to positive changes in gait performance [51–53]. Fourth, initial cognitive status and risk of falls of the participants was not measured meaning that the theoretical association between these factors remains speculative in the study participants and is only based on the available literature [5, 24]. Thus, future studies should consider testing the cognitive status before and after the intervention. Fifth, the sensitivity of the cognitive tests might have been too low to detect improvements in executive functioning in our sample of active, healthy elderly. Therefore, future studies should record cortical brain activity (e.g., with functional near-infrared spectroscopy) during the gait and cognitive tests to monitor changes in brain activation due to the training interventions [54]. Sixth, due to the Covid-19 pandemic the recruitment of participants was problematic [55], making it not possible to involve more inactive and vulnerable elderly. Therefore, interpretation of the present results with regard to the latter population is complicated. Nevertheless, knowing the effects of the different interventions in active elderly is also an important finding to inform future studies with a higher sample size (e.g., for adjusting the exercise protocols in terms of intensity).
In conclusion, the present study showed that neither a 12-week MMI nor UMI seems to have an impact on specific gait parameters (i.e., stride length, gait velocity, MTC) or their respective CoVs in physically active healthy elderly participants.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clark BC, Manini TM. What is dynapenia? Nutrition (Burbank, Los Angeles County, Calif.). 2012;28:495–503. 10.1016/j.nut.2011.12.002.10.1016/j.nut.2011.12.002PMC 357169222469110 · doi ↗ · pubmed ↗
- 2Keating CJ, et al. Influence of resistance training on gait & balance parameters in older adults: A systematic review. Int J Environ Res Public Health. 2021;18. 10.3390/ijerph 18041759.10.3390/ijerph 18041759 PMC 791815033670281 · doi ↗ · pubmed ↗
- 3Herold F, Törpel A, Schega L, Müller NG. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements - a systematic review. Eur Rev Aging Phys Activity: Official J Eur Group Res Elder Phys Activity. 2019;16. 10.1186/s 11556-019-0217-2.10.1186/s 11556-019-0217-2PMC 661769331333805 · doi ↗ · pubmed ↗
- 4European Glaucoma Society Terminology and Guidelines for Glaucoma. 5th Edition. Br J Ophthalmol. 2021;105:1–169. 10.1136/bjophthalmol-2021-egsguidelines.10.1136/bjophthalmol-2021-egsguidelines 34675001 · doi ↗ · pubmed ↗