Association of rs4646287 Polymorphism with the Risk of Hepatitis B Virus Infection and the Progression of Hepatocellular Carcinoma in an Iranian Population
Hassan Akrami, Mohammad Reza Fattahi, Mastaneh Zeraatiannejad, Jamal Sarvari, Yousef Nikmanesh, Zahra Mansourabadi, Zahra Yazdani

TL;DR
This study shows that the rs4646287 TT genotype is linked to a lower risk of hepatitis B-related diseases and liver cancer in an Iranian population.
Contribution
The study identifies a protective role of the rs4646287 TT genotype against HBV-related diseases in an Iranian population.
Findings
The TT genotype of rs4646287 is associated with a significantly reduced risk of cirrhosis and HCC.
TT genotype carriers showed a decreased correlation between HBV infection and progression to liver diseases.
The protective effect of the TT genotype was observed in comparison to healthy controls.
Abstract
Hepatitis B virus is responsible for more than one million deaths annually, mainly due to HBV-related diseases and HCC. HBV enters hepatocytes and interacts with the NTCP. While several SNPs have been linked to HBV infection and HCC, further research is needed to clarify the precise role of SNPs. The relationship of the rs4646287 SNP with the risk of HBV infection and the progression of cirrhosis and HCC has been investigated in different populations. This study aimed to evaluate the association of the rs4646287 SNP with HBV infection, cirrhosis, and HCC in an Iranian population. The whole blood DNA was extracted from healthy individuals and patients with HBV, cirrhosis, and HCC. Primers for the C and T variants were designed using Primer1. The genotypes of the samples were identified using Tetra-ARMS PCR. The Tetra-ARMS PCR products were analyzed by electrophoresis on 2.5% agarose…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
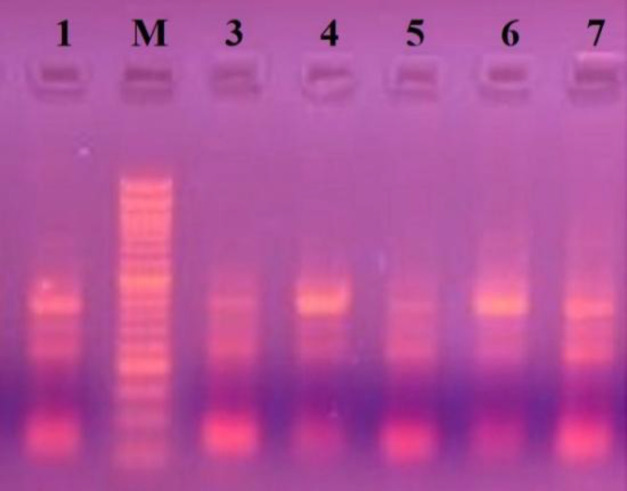 Fig. 1
Fig. 1|
|
|
|
|
| |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
| |||||
| Control | 55 | 23 | 27 | 36 | 5 | 9 | 77 | 23 | |||
| HBV | 53 | 25 | 24 | 32 | 3 | 14 | 67 | 31 | |||
| Cirrhosis | 52 | 8 | 12 | 14 | 1 | 5 | 29 | 11 | |||
| HCC | 55 | 7 | 10 | 12 | 1 | 4 | 25 | 9 | |||
|
|
|
|
|---|---|---|
| FIT-4646287 | 5'- CTG TGT GCT GCG TCT CCA GGC GT-3' | 23 |
| RIC-4646287 | 5'-CAT TAT AAG CAG AAA TCA GCA AGG GCG CG-3' | 29 |
| Fout-4646287 | 5'-GAC TAA ACC AGG GGG GAC TGG CTT GAG A -3' | 28 |
| Rout-4646287 | 5'-TTC CCC ATC AGA TGC AAT GAC ATT TCC A-3' | 28 |
|
|
|
|
|
| ||
|---|---|---|---|---|---|---|
|
|
| |||||
| Control | HBV | -0.118 | 0.142 | 0.406 | -0.40 | 0.16 |
| Cirrhosis | .800* | 0.187 | 0.000 | 0.43 | 1.17 | |
| HCC | 0.388 | 0.198 | 0.052 | 0.00 | 0.78 | |
| HBV | Control | 0.118 | 0.142 | 0.406 | -0.16 | 0.40 |
| Cirrhosis | .918* | 0.187 | 0.000 | 0.55 | 1.29 | |
| HCC | .507* | 0.199 | 0.012 | 0.11 | 0.90 | |
| Cirrhosis | Control | -.800* | 0.187 | 0.000 | -1.17 | -0.43 |
| HBV | -.918* | 0.187 | 0.000 | -1.29 | -0.55 | |
| HCC | -0.412 | 0.233 | 0.079 | -0.87 | 0.05 | |
| HCC | Control | -0.388 | 0.198 | 0.052 | -0.78 | 0.00 |
| HBV | -.507* | 0.199 | 0.012 | -0.90 | -0.11 | |
| Cirrhosis | 0.412 | 0.233 | 0.079 | -0.05 | 0.87 | |
|
|
|
|
|
|
|---|---|---|---|---|
| Control | 0.21 | - | - | - |
| HBV | 0.69 | - | - | - |
| Cirrhosis | 0.09 | - | - | - |
| HCC | 0.18 | - | - | - |
| HBV vs. Control | - | 1.02 | 0.86 | 0.810 - 1.288 |
| Cirrhosis vs. Control | - | 0.405 | 0.00 | 0.268 - 0.613 |
| HCC vs. Control | - | 0.45 | 0.00 | 0.311 - 0.667 |
| Cirrhosis vs. HBV | - | 0.411 | 0.00 | 0.275 - 0.614 |
| HCC vs. HBV | - | 0.46 | 0.00 | 0.316 - 0.665 |
| HCC vs. Cirrhosis | - | 1.08 | 0.78 | 0.627 - 1.862 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis B Virus Studies · Liver Disease Diagnosis and Treatment · Hepatitis C virus research
INTRODUCTION
Despite the availability of HBV vaccination, HBV remains a major public health problem in low- and middle-income countries. According to the World Health Organization, an estimated 254 million people were infected with this virus in 2024, with around 1.2 million new infections occurring each year. In 2022, HBV was responsible for 1.1 million deaths, primarily due to cirrhosis or HCC^[^^1^^,^^2^^]^.
HBV, cirrhosis, and HCC are closely interconnected. Indeed, most patients diagnosed with HCC have a history of cirrhosis. Research has shown that patients with cirrhosis caused by either HCV or HBV are at high risk of developing HCC^[^^3^^,^^4^^]^. Globally, HBV is recognized as one of the main causes of HCC. HBV infection may lead to HCC through direct and indirect ways. When HBV infects hepatocytes, the immune response system triggers necrosis and inflammation, resulting in the dedifferentiation and proliferation of hepatic cells to replace the dead cells. Furthermore, the integration of viral DNA into the host cell DNA causes instability and mutations within the host DNA. The long-term expression of wild-type and mutant HBx proteins, as well as wild-type and mutant large envelope proteins (viral proteins), may disrupt critical cellular processes, such as transcription. These factors, along with the inability of liver cells to repel carcinogens, can support carcinogenesis^[^^5^^]^.
Most HCC patients have a diagnosed HBV or HCV infection; however, not all HBV patients develop HCC. Studies have shown that only 20-30% of patients with HBV are at risk of developing cirrhosis or HCC^[6]^. Various factors, including viral infection, environmental conditions, and individual genetic properties, affect the likelihood of developing HCC in patients with HBV. It is also important to note that not all cirrhotic patients with HBV exhibit the same risk of progressing to HCC^[^^6^^,^^7^^]^. This observation indicates that the genetic background of the patients with HBV plays a significant role in the likelihood of developing cirrhosis or HCC.
NTCP is a glycoprotein located in the cell membrane of the hepatocytes. It acts as both a bile acid transporter and a cellular entry receptor for HBV^[^^8^^]^. The risk of developing liver cirrhosis and HCC is significantly elevated in individuals diagnosed with HBV infection. Nonetheless, the molecular mechanisms underlying the progression from HBV infection to cirrhosis and HCC are unknown^[^^9^^]^. Human genomes are most altered by SNPs, which affect both coding and non-coding regions of the genome. In coding regions, they can impact the structure and function of proteins, while in the non-coding regions, they influence gene expression. This outcome highlights the importance of studying SNPs for developing new strategies to combat HBV-linked HCC^[^^7^^,^^10^^-^^12^^]^.
Numerous studies have suggested the association of SNPs with HBV-linked HCC^[^^13^^,^^14^^]^. However, due to limitations such as the small sample size, further investigation is required to validate the association between this polymorphism and HBV-linked HCC. In this study, we investigated the relationship between the rs4646287 polymorphism and the risk of HBV infection, as well as the progression of cirrhosis and HCC in an Iranian population.
MATERIALS AND METHODS
Study design
In this study, 136 subjects were recruited from the Shahid Motahari Clinic in Shiraz, Iran, through 2022 and 2023, and subjected to genotyping using tetra-ARMS PCR. The study population consisted of 50 healthy controls, 49 patients with HBV infection, 20 with cirrhosis, and 17 with HCC. Inclusion criteria consisted of the confirmed clinical and pathological diagnosis of HBV infection, cirrhosis, and HCC, with no evidence of other infectious or inflammatory diseases. Exclusion criteria entailed individuals with viral infections and other diseases. All participants were in the range of 45 to 70 years.
Sample preparation and DNA isolation
Blood samples (5 ml) were collected from each participant through venipuncture and transferred into EDTA-containing tubes for DNA extraction. DNA was extracted using Bioneer'sAccuPrep® Genomic DNA Extraction Kit (Bioneer, Seoul, Korea), following the manufacturer’s protocol. The extracted DNA samples were stored at -20 °C until use.
Primer design
The sequence of the rs4646287 SNP was obtained from the NCBI (http://www.ncbi.nlm.nih.gov/snp). Primers for the C and T variants were designed for tetra-ARMS PCR using Primer1 (https://primer1.soton.ac.uk/ primer1.html). The specificity of the designed primers was evaluated using Gene Runner software (https://gene-runner.software.informer.com/) and confirmed through the BLAST (https://blast.ncbi.nlm. nih.gov/Blast.cgi).
Tetra-ARMS PCR and genotyping
Tetra-ARMS PCR was performed in a 10 μl reaction volume containing Taq DNA Polymerase Master Mix (2×; Ampliqon A/S, Denmark), genomic DNA (100 ng), outer and inner primers (1 mM each), 50 nM MgCl_2_ (1 µl), and DMSO (1 µl). The thermocycling conditions included an initial denaturation at 94 °C for 4 min, followed by 40 cycles of denaturation at 95°C for 30 seconds. The annealing and extension phases were carried out at 60 °C and 72 °C for 20 and 30 seconds, respectively. Finally, an additional extension was conducted at 72 °C for 5 min. The PCR products were analyzed by electrophoresis on 2.5% agarose gels, using ethidium bromide dye as a nucleic acid stain. A gel imaging system (Kimia Gene Technology Company, Iran) utilizing UV was employed to detect PCR bands.
Statistical analysis
All statistical analyses were carried out using SPSS version 25 (SPSS Inc., Chicago, IL, USA). The chi-square test was conducted to evaluate the Hardy-Weinberg equilibrium by comparing the observed and expected genotype frequencies within each group. To assess the association between genotype and disease risk, ORs, and 95% CIs were calculated by comparing the combined CC and CT genotypes with the TT genotype. The TT genotype, which was hypothesized to be associated with reduced cancer risk, served as the reference group for the null hypothesis (H_0_). One-way ANOVA was used to analyze differences in genotype frequencies treated as numeric variables across groups, with a significance cut-off of *p < *0.05. Welch's ANOVA test was performed to assess significant differences between the means of the groups, using a significance threshold of *p < *0.05. A p value of less than 0.05 was considered statistically significant for OR analysis.
RESULTS
Demographic information
The study included a total of 136 participants: 63 women (23 controls, 25 HBV-infected, 8 cirrhosis, and 7 HCC cases) and 73 men (27 controls, 24 HBV-infected, 12 cirrhosis, and 10 HCC cases). The mean age of the participants in all groups was 54.37 ± 1.07 years (SE = 0.042). As depicted in Table 1, the distributions of participants in each group were as follows: 50 healthy controls (mean age: 55 years), 49 HBV-infected cases (mean age: 53 years), 20 cirrhosis cases (mean age: 52 years), and 17 HCC cases (mean age: 55 years).
Tetra-ARMS PCR
Tetra-ARMS PCR products were separated via electrophoresis on 2.5% agarose gels. The results of Tetra-ARMS PCR are shown in Figure 1. The outer reverse and inner forward primers produced a 232 bp band (the C allele), the inner reverse and outer forward primers produced a 200 bp band (the T allele), and both outer primers produced a 380 bp band. The corresponding sequences for each primer are demonstrated in Table 2.
Relationship between genotypes and population characteristics
All study groups were assessed for potential biases related to sex and age. The genotypic frequencies showed no significant differences in sex or age among the groups. Also, there were no statistically significant differences in the sex ratio between the patient groups (HBV, cirrhosis, and HCC) and the control groups (*p *> 0.05). Overall, the analysis indicated that the rs4646287 SNP was not associated with age or gender in any of the evaluated groups within the Iranian population (*p *> 0.05).
Variant(C>T) genotype distributions
The allelic and genotypic frequencies of the rs4646287 SNP among the four study groups are presented in Table 1. Notably, genotypic distribution in all study groups conformed to the Hardy-Weinberg equilibrium. Table 3 illustrates statistically significant differences in genotype frequencies among the following groups (*p *< 0.05): cirrhosis versus control, HBV-infected individuals versus control, and HBV-infected individuals versus HCC patients. Conversely, no significant differences were observed in genotype frequencies between the cirrhosis versus HCC patients or between HBV-infected individuals versus controls (*p *< 0.05). Statistical analysis revealed no correlation between genotypes in the control group and between the cirrhosis and HCC groups (*p *> 0.05). However, a reduced likelihood of association was identified for the rs4646287 TT genotype, with odds ratios of 0.4 and a *p *value of 0.002 for the comparison between the cirrhosis and control groups. A similar trend was found between the HCC and control groups (*p *< 0.05; Table 4).
Tetra-ARMS PCR results for six samples genotyped for the rs4646287 SNP. Lane 1-7: individual samples; M: 50 bp DNA Ladder (SMOBIO Technology Inc., Taiwan).
DISCUSSION
HBV infection begins when viral preS1 peptides attach to the NTCP receptors on hepatocytes^[^^13^^]^. Several SNPs, including rs4646287, rs7154439, and rs2296651, have been identified in NTCP that are associated with HBV infection and HBV-related diseases across different populations^[14]^. However, the relationship between the rs4646287 SNP and HBV infection and HBV-related diseases, such as cirrhosis and HCC, remains unclear in the Iranian population. This study investigated the rs4646287 variant in the NTCP gene to give an insight into the effect of host genetic polymorphisms on HBV infection, cirrhosis, and HCC development. Research has shown that SNP variants, such as rs4646287, rs61745930, and rs2296651, can influence HBV infection and the development of cirrhosis and HCC^[^^15^^-^^18^^]^. A previous study conducted on the Chinese population has suggested a link between the NTCP Rs4646287 variant and HBV-related fibrosis, as well as the incidence of hepatocellular carcinoma. However, no significant association was found between the non-cirrhosis and cirrhosis groups^[^^19^^]^. A meta-analysis examining the relationship between NTCP polymorphisms and liver disease development, including HCC, indicated that the allele of rs2296651 was inversely associated with HBV infection and HCC progression. In contrast, other SNPs, including rs7154439, rs4646285, rs4646287, and rs4646296, did not show a significant effect on HBV infection or the development of cirrhosis and HCC. These observations highlight the need for further research to clarify the association between NTCP polymorphisms and the progression of liver diseases^[^^20^^]^.
Some SNPs are located in the introns of genes, and each allele of these SNPs may alter the intron-based transcription regulatory sequences, affecting transcription rates of the genes^[^^21^^,^^22^^]^. Specifically, the rs4646287SNP may act as a regulatory sequence found in the first intron that influences the NTCP transcription^[^^23^^]^. Furthermore, studies have indicated that rs4646287 may impact HBV infection and HCC^[^^19^^,^^23^^]^. In this study, we analyzed the correlation between the rs4646287SNP variant and HBV infection, liver cirrhosis, and HCC in an Iranian population. We also evaluated the rs4646287SNP variants using Tetra-ARMS PCR. Our data analysis revealed no significant correlations between the genotypes in the control and HBV groups, nor between the cirrhosis and HCC groups among the Iranian population. However, we observed a decreased likelihood of association with the TT genotype in the control, cirrhosis, and HCC groups.
Additionally, the TT rs4646287 SNP genotype seems to reduce the correlation between the HBV, control, and cirrhosis groups in the Iranian population, suggesting the protective role of the TT genotype against cirrhosis and HCC. Our findings regarding the effect of the rs4646287 variant on HBV infection in the Iranian population were consistent with previous studies^[^^14^^,^^23^^,^^24^^]^. Research conducted on the Ghanaian population revealed that only rs2296651 was linked to a high risk of HBV infection, while rs4646287 did not show such an association^[15]^. Similarly, a study involving a Thai population demonstrated that rs4646287 was not associated with HBV infection or HCC development^[^^24^^]^. However, an investigation in the Han Chinese population suggested that the rs4646287 SNP variant might be associated with an increased risk of HBV infection. They found that the “CT + TT” genotypes of the rs4646287 SNP were significantly lower in the HCC group compared to the controls^[^^23^^]^.
Cirrhosis is an advanced stage of liver disorder characterized by fibrosis and hepatic parenchymal lesions, often resulting from HBV and HCV infection^[25]^. Our findings indicated that HBV-infected patients with the rs4646287 TT genotype had a lower risk of developing cirrhosis and HCC. These results in the Iranian population align with those reported in Han Chinese individuals^[^^11^^]^. However, our data contrast with some studies conducted in China, where two studies found that the rs4646287 TT genotype is associated with a high risk of HBV-related fibrosis and HCC development^[^^19^^,^^26^^]^. The variations in our findings and those from other studies regarding the association of the rs4646287 SNP with HBV infection, HBV-related diseases, and HCC development suggest that the influence of the rs4646287 SNP might be inconsistent in different populations. These discrepancies could be attributed to differences in sample sizes. Therefore, more studies are necessary to confirm our findings and clarify the relationship between the rs4646287 SNP and HCC development.
CONCLUSION
Our findings suggest that the rs4646287TT SNP may be linked to a lower risk of HBV-related diseases and the development of HCC in the Iranian population. However, further investigations are needed to precisely clarify the role of the rs4646287 SNP in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tourkochristou E Assimakopoulos SF Thomopoulos K Marangos M Triantos CNAFLD and HBV interplay-related mechanisms underlying liver disease progression Front Immunol.2022139655483654476110.3389/fimmu.2022.965548 PMC 9760931 · doi ↗ · pubmed ↗
- 2Razavi-Shearer D Gamkrelidze I Pan C Jia J Berg T Gray R Global prevalence, cascade of care, and prophylaxis coverage of hepatitis B in 2022: A modelling study lancet Gastroenterol hepatol 2023 8108799073751741410.1016/S 2468-1253(23)00197-8 · doi ↗ · pubmed ↗
- 3Fattovich G Stroffolini T Zagni I Donato F Hepatocellular carcinoma in cirrhosis: Incidence and risk factors Gastroenterology 20041275355010.1053/j.gastro.2004.09.01415508101 · doi ↗ · pubmed ↗
- 4Najafimemar Z Tabarraei A Talei G Moradi A Prevalence and genotyping of torque teno virus in HBV/HIV and chronic HBV patients in Iran IBJ 2018225338442925392210.29252/ibj.22.5.338PMC 6058187 · doi ↗ · pubmed ↗
- 5Levrero M Zucman-Rossi J Mechanisms of HBV-induced hepatocellular carcinoma J Hepatol 20166418410110.1016/j.jhep.2016.02.02127084040 · doi ↗ · pubmed ↗
- 6Liu Q Liu G Lin Z Lin Z Tian N Lin X The association of lnc RNA SN Ps and SN Ps‐environment interactions based on GWAS with HBV‐related HCC risk and progression Mol Genet Genomic Med 202192158510.1002/mgg 3.1585 PMC 807715933432784 · doi ↗ · pubmed ↗
- 7Zhang Y-Q Peng L-J Cao Y-R Zeng Z-P Wu Y-J Shi H Risk factors for hepatocellular carcinoma in cirrhotic patients with chronic hepatitis B Genet Test Mol Biomarkers 2016209535432739158410.1089/gtmb.2016.0062 · doi ↗ · pubmed ↗
- 8Tan X Xiang Y Shi J Chen L Yu D Targeting NTCP for liver disease treatment: A promising strategy J Pharm Anal 20241491009793931085010.1016/j.jpha.2024.100979 PMC 11415714 · doi ↗ · pubmed ↗