Multisite infection with Austrian syndrome caused by non-vaccine pneumococcal serotype—case report
Frederik Juel Pontoppidan Børrild, Emil Fosbøl, Casper Roed, Melissa Hornbæk Øvre, Helle Brander Eriksen, Christian Kraef, Jannik Helweg-Larsen, Zitta Barrella Harboe, Christina Ekenberg

TL;DR
A rare and severe case of Austrian syndrome caused by a non-vaccine pneumococcal serotype is reported in an immunocompromised patient.
Contribution
The report highlights a rare multisite infection caused by a non-vaccine pneumococcal serotype in an immunocompromised individual.
Findings
Austrian syndrome was complicated by spondylodiscitis and endophthalmitis in an immunocompromised patient.
The causative serotype (23B) is not included in standard pneumococcal vaccines.
Reduced susceptibility to benzylpenicillin was observed, which is uncommon in Denmark.
Abstract
Although rare, Austrian syndrome remains a life-threatening triad consisting of pneumonia, endocarditis, and meningitis caused by Streptococcus pneumoniae. We present a case of Austrian syndrome, further complicated by spondylodiscitis and endophthalmitis, in an immunocompromised male receiving methotrexate treatment for rheumatoid arthritis. The infection was caused by a non-vaccine pneumococcal serotype (23B). Susceptibility testing showed reduced susceptibility towards benzylpenicillin, an uncommon finding in Denmark. This case illustrates some of the challenges faced in managing invasive pneumococcal disease and underlines the importance of continued awareness of this disease, particularly in immunocompromised patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
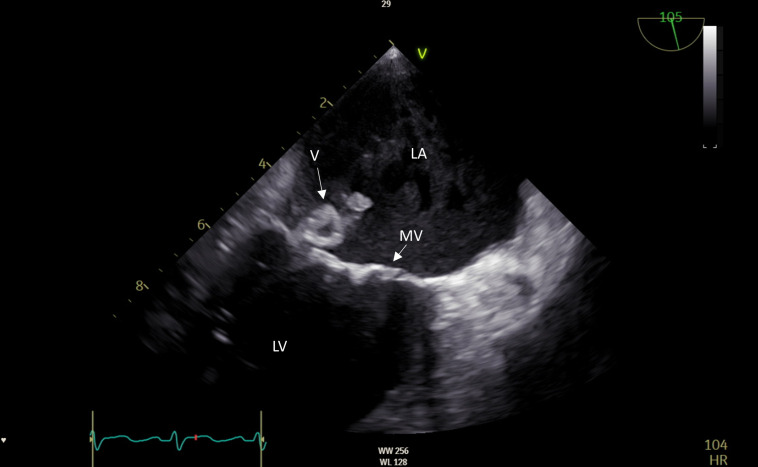 Fig 1
Fig 1| Antibiotic | Susceptibility | MIC |
|---|---|---|
| Penicillin | R | 0.250 mg/L |
| Ceftriaxone | S | 0.125 mg/L |
| Cefotaxime | S | 0.125 mg/L |
| Moxifloxacin | S | 0.250 mg/L |
| Linezolid | S | 2.000 mg/L |
| Rifampicin | S | 0.064 mg/L |
| Amoxicillin, p.o. | N/A | N/A |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Infective Endocarditis Diagnosis and Management · Infectious Diseases and Tuberculosis
INTRODUCTION
Due to the widespread use of β-lactam antibiotics and the introduction of pneumococcal vaccines, the incidence of invasive pneumococcal disease (IPD) has declined (1). Still, it remains associated with high morbidity and mortality, including in immunocompromised individuals (2). Austrian syndrome is a triad of meningitis, endocarditis, and pneumonia caused by Streptococcus pneumoniae. It is associated with a poor prognosis, and the severity of Austrian syndrome highlights the importance of early diagnosis and treatment in addition to timely vaccination. Furthermore, with the increased usage of pneumococcal vaccines, non-vaccine serotypes are emerging, emphasizing the need for continued surveillance. Here, we present a case of Austrian syndrome in a 65-year-old male undergoing treatment with methotrexate due to rheumatoid arthritis (RA).
CASE PRESENTATION
A 65-year-old male with a medical history of hypertension and rheumatoid arthritis (RA) was admitted to the hospital with a 14-day history of cough, malaise, and new-onset altered mental state. The patient received treatment with methotrexate 20 mg weekly, which is considered low-to-moderate dose (>20 mg weekly is considered moderate-severe immunosuppression) (3), and had 1 week prior to admission received a steroid injection, which may have caused a synergistic immunosuppressive effect. On examination, he appeared mildly disoriented, and a systolic murmur was noted upon auscultation. His vital signs were blood pressure of 113/75 mm Hg, pulse rate of 110, body temperature of 37.5°C, respiratory rate of 18, and oxygen saturation of 99% without supplementing oxygen. Initial blood tests showed a leukocyte count of 11.1 × 10^9^/L (3.5–8.8 × 10^9^/L), CRP of 341 mg/L (<10 mg/L), and elevated lactate dehydrogenase and liver enzymes. Given the concurrent confusion and subfebrile temperature, a lumbar puncture was done, revealing the cerebrospinal fluid (CSF) with neutrophilic pleocytosis with a white cell count of 2,240 cells/µL (<5 cells/µL), low glucose of 0.8 mmol/L (2.2–3.9 mmol/L), elevated protein of 3.1 g/L (0.15–0.5 g/L), and lactate of 12.4 mmol/L (1.1–2.4 mmol/L). Empiric treatment for bacterial meningitis was initiated, consisting of intravenously (IV) administered benzylpenicillin 1.8 g every 4 h, ceftriaxone 4 g once daily, and dexamethasone 10 mg every 6 h. Multiplex nucleic acid test (The BIOFIRE FILMARRAY Meningitis-Encephalitis Panel, BioMerieux) performed on CSF tested positive for S. pneumoniae within 2 h after the lumbar puncture. A computed tomography (CT) followed by magnetic resonance imaging (MRI) of the brain demonstrated small, scattered, primarily cortical infarctions in both hemispheres, suggesting septic emboli. The transthoracic echocardiogram (TTE) was inconclusive, while a transesophageal echocardiogram (TEE) revealed a large vegetation of the posterior mitral leaflet (Fig. 1). In relation to the vegetation, there was a perforation of the valve, and the infection extended to the annulus of the valve. Cardiac CT angiography (CTA) indicated a ruptured abscess in relation to the mitral valve, which the TEE confirmed. Furthermore, vegetations were also found on the tricuspid and on the aortic valves without substantial valve destruction. The patient underwent reconstructive surgery on both the mitral and the tricuspid valve. A follow-up TEE subsequently showed a minor residual perforation of the mitral valve, along with slight mitral regurgitation. Blood cultures yielded growth of S. pneumoniae, serotype 23B. Species identification was performed combining colony morphology, optochin susceptibility, and identification with MALDI-TOF MS Biotyper (Bruker, Bremen, Germany). A Gram stain was performed on CSF with no visible microorganisms. Several polynuclear lymphocytes were seen with a few mononuclear lymphocytes. S. pneumoniae was identified in CSF using the multiplex nucleic acid test; culture was negative. From mitral and tricuspidal tissues, S. pneumoniae was identified with an in-house 16S rRNA sequencing. No growth emerged.
First transesophageal echocardiogram (TEE) of the patient. The TEE revealed a large vegetation of the posterior mitral leaflet. Further, in relation to the vegetation, the mitral valve was perforated, and the infection extended to the annulus of the valve, and a ruptured abscess in relation to the mitral valve was found. LA: left atrium, LV: left ventricle, MV: mitral valve, V: vegetation.
Susceptibility testing was performed according to the EUCAST methodology for disc diffusion and gradient tests and interpreted using EUCAST breakpoint table 14.0 (https://www.eucast.org). For S. pneumoniae, screening with the oxacillin 1 µg disk diffusion is standard. For susceptible isolates (≥20 mm), benzylpenicillin, ceftriaxone, meropenem, and other β-lactam antibiotics can be reported susceptible. The blood culture isolate had decreased susceptibility to oxacillin (10 mm), so a supplementary gradient test was performed, which is recommended for meningitis isolates. With a minimum inhibitory concentration (MIC) of 0.250 mg/L towards benzylpenicillin, this is reported resistant according to meningitis breakpoints (S ≤ 0.06 mg/L). Ceftriaxone was susceptible with a MIC of 0.125 mg/L (S ≤ 0.5 mg/L). Supplementary susceptibility testing of the isolate was performed because of endocarditis (Table 1). Consequently, benzylpenicillin was discontinued, and moxifloxacin 400 mg twice daily per os (p.o.) was prescribed, in addition to ceftriaxone. At day 4 of hospitalization, the patient presented with visual hallucinations and blurry vision. Upon ophthalmologic examinations, the visual impairments were found to be caused by bilateral endophthalmitis. A positron emission tomography (PET) scan was performed to investigate additional infectious foci. Aside from a pneumonic infiltrate, it showed inflammatory alterations suggestive of spondylodiscitis at the Th12–L3 level.
After 6 weeks of antibiotic treatment with ceftriaxone and moxifloxacin, the patient was discharged with amoxicillin 750 mg p.o. four times daily for six additional weeks to complete treatment for spondylodiscitis.
During follow-up consultations in the outpatient clinic, the patient kept gradually improving, and he resumed working. His visual complaints, however, are expected to be permanent to some extent. The patient has later been diagnosed with epilepsy, which has been attributed to the central nervous system involvement.
DISCUSSION
We have presented a rare case of Austrian syndrome, a triad consisting of pneumonia, endocarditis, and meningitis caused by S. pneumoniae, further complicated by spondylodiscitis and endophthalmitis in an immunocompromised adult. Austrian syndrome, or Osler’s triad, is a rare phenomenon, as only 1%–3% of cases with bacterial endocarditis are caused by pneumococci (4), of whom less than 1% end up developing Austrian syndrome (5). The triad is associated with a poor prognosis, as pneumococcal endocarditis alone has a mortality rate ranging from 28% to 60% (4), while the fatality rates of pneumococcal meningitis have been reported to be 19% to 37% (6). Madu et al. conducted a systematic review of 71 cases of Austrian syndrome, reporting a case fatality of 28% in cases documented between 1991 and 2022, with the majority of studies (70%) published after 2010 (7).
The finding of S. pneumoniae with decreased susceptibility towards penicillin is a relatively uncommon finding in Denmark, as 94% of S. pneumoniae isolates in invasive infections (bacteremia and meningitis) are susceptible to benzylpenicillin (2023) (8). The pneumococcal isolate was identified as serotype 23B. In 2024 (data available up until October), six cases of IPD due to serotype 23B were registered in Denmark, of which only two were susceptible to penicillin (Statens Serum Institut, unpublished data).
Importantly, this serotype is not covered by any of the licensed pneumococcal vaccines (9). While the widespread availability of pneumococcal vaccines has proved to decrease the incidence of IPD caused by vaccine serotypes markedly, non-vaccine serotypes can cause severe disease (10, 11). In Denmark, the implementation of PCV7 and PCV13 in the Danish childhood vaccination program has decreased the incidence of vaccine serotypes significantly, although non-vaccine serotypes have increased (12). This emphasizes the importance of continuously surveying the distribution of pneumococcal serotypes causing IPD to ensure that future vaccines can be adjusted to cover the most prevalent serotypes. A Swedish study found that patients ≥65 years and patients with predisposing factors, such as immunosuppressive therapy, were more likely to have IPD caused by a non-vaccine serotype (13). Furthermore, serotype 23B has been found as a cause of severe IPD in previously healthy young, vaccinated adults (14). To our knowledge, it is not known if this specific serotype, or any other serotype in particular, is associated with the development of Austrian syndrome.
Of note, the patient in our case report had not previously received any pneumococcal vaccine but was vaccinated in the outpatient clinic after he had recovered. Unfortunately, several studies have shown that pneumococcal vaccine uptake in at-risk populations remains suboptimal (15) despite well-established guidelines (16). In Denmark, pneumococcal vaccination is recommended to high-risk individuals, including patients with rheumatic diseases receiving immunosuppressive therapy, such as methotrexate, preferably prior to initiation of immunosuppression. The cost is partially covered by a subsidy.
This case demonstrates the ongoing challenges of managing IPD. Regardless of vaccination status, awareness and suspicion of IPD should be upheld, particularly in—but not restricted to—the immunocompromised patients, in whom an atypical presentation of symptoms is not uncommon.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Myint TTH, Madhava H, Balmer P, Christopoulou D, Attal S, Menegas D, Sprenger R, Bonnet E. 2013. The impact of 7-valent pneumococcal conjugate vaccine on invasive pneumococcal disease: a literature review. Adv Ther 30:127–151. doi:10.1007/s 12325-013-0007-623397399 · doi ↗ · pubmed ↗
- 2van Aalst M, Lötsch F, Spijker R, van der Meer JTM, Langendam MW, Goorhuis A, Grobusch MP, de Bree GJ. 2018. Incidence of invasive pneumococcal disease in immunocompromised patients: a systematic review and meta-analysis. Travel Med Infect Dis 24:89–100. doi:10.1016/j.tmaid.2018.05.01629860151 · doi ↗ · pubmed ↗
- 3Kucharzik T, Ellul P, Greuter T, Rahier JF, Verstockt B, Abreu C, Albuquerque A, Allocca M, Esteve M, Farraye FA, Gordon H, Karmiris K, Kopylov U, Kirchgesner J, Mac Mahon E, Magro F, Maaser C, de Ridder L, Taxonera C, Toruner M, Tremblay L, Scharl M, Viget N, Zabana Y, Vavricka S. 2021. ECCO guidelines on the prevention, diagnosis, and management of infections in inflammatory bowel disease. J Crohns Colitis 15:879–913. doi:10.1093/ecco-jcc/jjab 05233730753 · doi ↗ · pubmed ↗
- 4Aronin SI, Mukherjee SK, West JC, Cooney EL. 1998. Review of pneumococcal endocarditis in adults in the penicillin era. Clin Infect Dis 26:165–171. doi:10.1086/5162799455526 · doi ↗ · pubmed ↗
- 5Mwana-Yile HK, Samia E, Hanane B, Claude BJ, Filali MKE. 2024. Austrian syndrome: a rare case report. Afr J Infect Dis 18:23–27. doi:10.21010/Ajidv 18i 1.438058417 PMC 10696653 · doi ↗ · pubmed ↗
- 6van de Beek D, de Gans J, Tunkel AR, Wijdicks EFM. 2006. Community-acquired bacterial meningitis in adults. N Engl J Med 354:44–53. doi:10.1056/NEJ Mra 05211616394301 · doi ↗ · pubmed ↗
- 7Madu A, Alex-Okoro T, Okoduwa A, Cotton J. 2024. Austrian syndrome: report of one case and a systematic review of case reports – new insights. Clin Med (Northfield) 24:100205. doi:10.1016/j.clinme.2024.100205 PMC 1110929338649138 · doi ↗ · pubmed ↗
- 8Slotved HC, Fuursted K. 2023. Resistance in Human Pathogens, The Danish Integrated Antimicrobial Resistance Monitoring and Research Programme DANMAP. Copenhagen, Denmark Statens Serum Institut and Technical University of Denmark