Bartonella-associated glomerulonephritis without endocarditis in a renal transplant recipient
Grace A. Schaack, Rene Bulnes, Deborah Jebakumar, Allen R. Hendricks, Andrew E. Clark

TL;DR
A renal transplant recipient developed kidney disease caused by Bartonella bacteria without heart infection, highlighting the need for careful diagnosis in immunocompromised patients.
Contribution
This case expands understanding of Bartonella-associated glomerulonephritis occurring without endocarditis in transplant recipients.
Findings
Bartonella henselae can cause glomerulonephritis in renal transplant recipients without endocarditis.
Diagnosis relies on serology and molecular testing due to poor culture sensitivity.
Immunocompromised patients with cat or flea exposure should be evaluated for Bartonella.
Abstract
Bartonella henselae is a fastidious gram-negative rod that can cause systemic disease in immunocompromised patients. Infection may be complicated by glomerulonephritis, often in the setting of culture-negative infective endocarditis. The histologic pattern of Bartonella-associated glomerulonephritis is variable and often difficult to distinguish from non-infectious causes of glomerulonephritis by histopathology. Prompt, accurate diagnosis is further complicated by the poor sensitivity of routine culture methods for the detection of B. henselae, and serology or adjunctive molecular testing is typically required for microbiologic diagnosis. A middle-aged male renal transplant recipient was admitted to our hospital with fever, nausea, vomiting, diarrhea, and laboratory evidence of acute kidney injury. A thorough infectious disease work-up revealed markedly elevated B. henselae…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
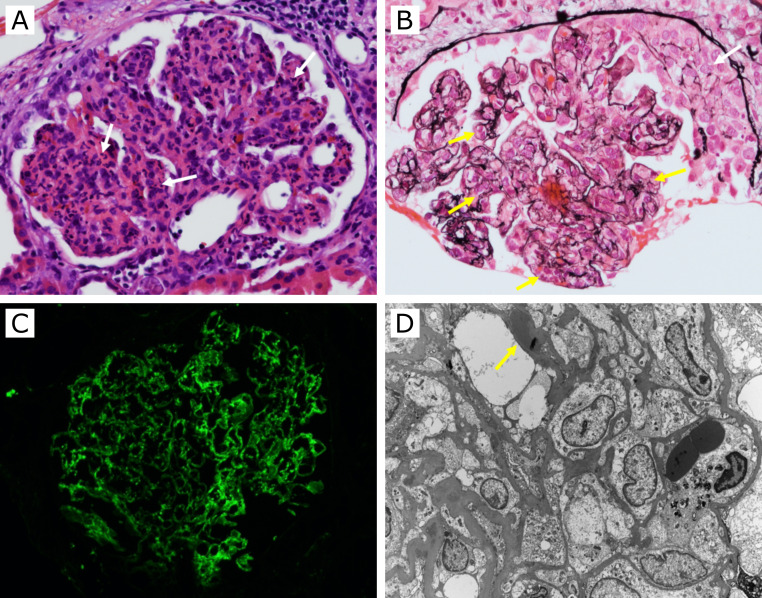 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBartonella species infections research · Rabies epidemiology and control · Traumatic Ocular and Foreign Body Injuries
INTRODUCTION
Bartonella henselae is a species of fastidious, gram-negative, pleomorphic, rod-shaped bacteria that is well-known as the causative agent of cat scratch disease (1, 2). Bartonella species are facultatively intracellular pathogens that primarily infect host erythrocytes and endothelial cells. They can infect numerous host species and are transmitted by a variety of hematophagous arthropod vectors. In the United States, the classic reservoir and vector for B. henselae are the cat and the cat flea (Ctenocephalides felis), respectively. In feline hosts, B. henselae replicates intraerythrocytically, facilitating immune evasion and bacteremia. Kittens are more likely to transmit B. henselae than adult cats, and it is estimated that approximately half of all domestic cats are or have been infected (3). Humans can become infected with B. henselae upon contact with cats and/or cat fleas and are a dead-end host (1).
Infection with B. henselae in humans typically manifests as cat scratch disease characterized by erythematous papular skin lesions at the site of inoculation, regional lymphadenopathy, fever, and fatigue (1). In immunocompromised hosts, infection is more likely to cause disseminated bartonellosis, and these patients may lack the characteristic skin lesions and lymphadenopathy seen in typical cat scratch disease (4, 5). In a review of 29 cases of B. henselae infections in solid organ transplant recipients, Psarros et al. found that the majority (72%) of these patients developed disseminated disease, lymphadenopathy was present in 41% of the cases, and skin lesions were present in only 24% of the cases (4).
Glomerulonephritis is an important complication of disseminated bartonellosis that can be challenging to accurately attribute to Bartonella infection, particularly in immunocompromised patients lacking a classical presentation of cat scratch disease. A variety of histologic patterns of glomerulonephritis may be seen on renal biopsy in the setting of bartonellosis (6–15). This variability in both clinical and histopathologic presentation makes Bartonella infection difficult to distinguish from other infectious and non-infectious causes of glomerulonephritis. B. henselae is also an important etiologic agent of culture-negative infective endocarditis, and Bartonella-associated glomerulonephritis often occurs within this setting. Rarely, however, glomerulonephritis due to Bartonella infection has been reported in the absence of definitive evidence of endocarditis (16–18). Here, we present a case of disseminated bartonellosis with glomerulonephritis in a renal transplant patient without definite endocarditis and without classic features of cat scratch disease, highlighting the importance of considering B. henselae infection in immunosuppressed individuals with relevant environmental exposures.
CASE PRESENTATION
A middle-aged male kidney transplant recipient presented to the emergency department for further evaluation after having been found to have elevated creatinine levels during a clinic visit. He reported an approximately 3-week history of malaise and watery, non-bloody diarrhea with worsening nausea and vomiting. He also reported low blood pressure readings at home, subjective fevers, and unquantified weight loss.
His past medical history was pertinent for type 1 diabetes mellitus complicated by end-stage renal disease, for which he received a deceased-donor kidney transplant. His transplant was performed 18 weeks prior to presentation and was complicated by delayed graft function. He underwent induction therapy with rabbit anti-thymocyte globulin, and his maintenance immunosuppression included mycophenolic acid, tacrolimus, and prednisone. His antimicrobial prophylaxis consisted of trimethoprim-sulfamethoxazole and valacyclovir. He resided in a house in Texas with multiple cats. He also recalled a recent flea infestation of his home, presumably attributable to his recent adoption of two rescued kittens and his numerous other cats with indoor and outdoor access.
Upon presentation, he had a fever of 38.6°C, dry oral mucosa, no abdominal distension or tenderness, and multiple lacerations on his hands and feet inflicted by his cats. No other skin findings were present. Lymphadenopathy was absent. Initial laboratory studies were notable for thrombocytopenia (86 × 10^3^/µL), hyponatremia (121 mM), hypokalemia (3.3 mM), elevated serum creatinine (5.84 mg/dL whereas at baseline 2.1 mg/dL) and hypocomplementemia (C4 and C3 levels of 13 mg/dL). He was admitted for management of acute kidney injury and was empirically started on ceftriaxone and vancomycin. Doxycycline was added to the empiric regimen for rickettsial coverage in the setting of immunosuppression and geographic risk factors.
Initial microbiologic studies, including blood cultures, stool cultures, stool examination for ova and parasites, and stool PCR via FilmArray GI Panel (BioFire Diagnostics, Inc.) were negative. Additional tests for Q fever, murine typhus, coccidioidomycosis, histoplasmosis, bartonellosis, and toxoplasmosis were ordered. On the ninth day of admission, serologic testing revealed an anti-B. henselae IgG titer of 1:8192 (normal < 128), anti-B. henselae IgM ≥ 1:20 (normal < 20), and anti-B. quintana IgG titer of 1:512 (normal < 128). Targeted PCR for Bartonella in a whole-blood specimen was negative. Rifabutin was initiated along with the continuation of doxycycline for the treatment of bartonellosis. A metagenomic sequencing assay using cell-free DNA from plasma (Karius Inc.) detected DNA from B. henselae, but this result returned after patient discharge.
Cardiac imaging by both transthoracic and transesophageal echocardiogram did not reveal any valvular vegetations. Computed tomography (CT) of the abdomen and pelvis identified mild splenomegaly (13.5 cm) and two nonspecific peripheral splenic lesions (2 and 2.7 cm in diameter) that were not investigated further. Additional studies, including chest CT, esophagogastroduodenoscopy, and colonoscopy, did not reveal evidence of direct involvement by Bartonella infection.
On the 14th day of admission, a biopsy of the renal allograft was performed and showed evidence of glomerulonephritis. Fifteen open glomeruli showed diffuse, global endocapillary hypercellularity with numerous neutrophils (Fig. 1A). Two glomeruli had cellular crescents (Fig. 1B). Moderate tubulitis and severe acute tubular injury were present with multifocal interstitial edema and moderate inflammatory cell infiltration by mononuclear leukocytes and small numbers of eosinophils. Immunofluorescence microscopy showed diffuse, segmental, granular glomerular capillary wall and mesangial positive staining by immunoglobulin A (IgA) (4 + on a 0–4 scale), immunoglobulin M (IgM) (4+), C3 (4+, Fig. 1C), C4d (4+), kappa (3+), and lambda (3+). Ultrastructural examination of two glomeruli showed severe (>80%) foot process effacement. Multiple subepithelial, subendothelial, and mesangial immune-complex-type, electron-dense deposits were seen. Some of the subepithelial deposits were “hump-shaped” (Fig. 1D). No tubuloreticular inclusions were identified. These findings were consistent with an IgA-codominant, infection-related glomerulonephritis.
Kidney biopsy. (A) H&E stain shows numerous neutrophils within a glomerulus (white arrow, ×200). (B) Jones methenamine silver stain shows global endocapillary hypercellularity (yellow arrows) and a cellular crescent (white arrow, ×200). (C) Immunofluorescence for C3 shows diffuse, segmental, granular glomerular staining (×200). (D) Electron microscopy shows severe foot process effacement and multiple subepithelial electron-dense deposits, some of which are hump-shaped (yellow arrow, ×2,550).
The patient’s gastrointestinal symptoms and fever resolved after 4 days; however, his kidney function did not recover in the short term, and he required intermittent renal replacement therapy. He ultimately completed a 2-week course of rifabutin and 3 months of doxycycline along with a prednisone taper. By the time antibiotic therapy was completed, his renal function stabilized and he no longer required dialysis.
DISCUSSION
This case illustrates several potential challenges in the diagnosis of Bartonella-associated glomerulonephritis. The patient’s immunocompromised status and exposures to cats and fleas were key elements of the history that led to early consideration of Bartonella infection despite the absence of a typical presentation of cat scratch disease. Because Bartonella species are not typically detected in routine culture, a high index of suspicion is required to ensure appropriate diagnostic test selection and correct interpretation of microbiologic and histopathologic data.
B. henselae culture is challenging, requiring extended incubation times of up to 21 days at 35–37°C in 5% CO_2_ (2). Due to the low sensitivity of culture-based methods, laboratory diagnosis relies heavily on serology (19–21). Serologic testing is currently the most reliable, sensitive, minimally invasive testing method for B. henselae, but it is important to be mindful of its limitations when interpreting results (20, 21). For example, serologic assays for Bartonella exhibit cross-reactivity with Chlamydia/Chlamydophila and with Coxiella (20). There is also serological cross-reactivity between B. henselae and B. quintana, but markedly higher titers against one species versus the other are indicative of the more likely causative agent (20). It is also notable that mildly elevated titers may be present at baseline in the general healthy population, so it is important to look for evidence of true positivity (IgG titer of at least 1:256 and/or a fourfold rise in IgG titer) through comparison of acute and convalescent samples (21). In the case presented here, the dramatically elevated anti-B. henselae IgG titer and mildly elevated anti-B. quintana IgG titer are suggestive of a true B. henselae infection resulting in production of IgG with mild cross-reactivity against B. quintana.
In addition to serology, complementary testing via histology and nucleic acid amplification and sequencing methodologies can be helpful for diagnosis (20, 21). If biopsy specimens are available, histologic examination using immunohistochemistry or nonspecific methods such as Warthin-Starry silver impregnation can help to directly visualize organisms in tissue. Targeted nucleic acid amplification testing and broader-range sequencing approaches (i.e., 16S rRNA sequencing and shotgun metagenomic approaches) may be used to identify B. henselae in patient specimens but show better sensitivity for solid tissue specimens than for blood (21). Therefore, while a positive Bartonella PCR result is supportive of a diagnosis of bartonellosis, a negative PCR result, as was seen in our case, is by no means contrary to the diagnosis. Similarly, detection of B. henselae DNA by metagenomic sequencing supports, but is not required for, bartonellosis diagnosis. Metagenomic sequencing did not provide significant diagnostic value. Metagenomic sequencing of cell-free DNA for infectious agents can also incur increased cost and turnaround time compared to serologic testing for Bartonella spp. In the case presented here, serology was sufficient to make the diagnosis of bartonellosis and was used to make diagnostic and treatment decisions. The metagenomic sequencing resulted several days later after patient discharge and did not impact management. Thus, the clinical utility of such testing should be carefully considered before ordering to avoid unnecessary costs and diagnostic redundancy.
Histopathologic investigation in the case presented here did not include direct observation of microorganisms but illustrates one of many patterns of glomerular injury that may be seen in association with bartonellosis. Several cases of Bartonella-associated ANCA-positive glomerulonephritis have been reported, highlighting the risk of misdiagnosis of vasculitis rather than infection-related glomerulonephritis (11, 13, 15). Studies have shown that while the rate of ANCA positivity can range from 18% to 33% in infective endocarditis cases, positivity can be as high as 60–75% in Bartonella-associated glomerulonephritis (15, 22, 23). Histological features on kidney biopsy show slightly higher occurrence of crescents within glomeruli in Bartonella infections compared to other microorganisms that cause infective endocarditis (83% vs 61%) (23). C3-dominant immunofluorescence staining with frequent C1q and IgM staining is common. IgA positive staining is seen most often in staphylococcal infection-associated glomerulonephritis (22, 24). Mesangial and capillary wall electron-dense deposits occur with near equal incidence in both Bartonella-associated glomerulonephritis and glomerulonephritis caused by other microorganisms (23). Subepithelial humps occur in a small percentage of cases in both Bartonella-associated and other infection-related glomerulonephritis.
Given that Bartonella-associated glomerulonephritis often occurs in the setting of culture-negative endocarditis, it is important to consider infective endocarditis when evidence of glomerulonephritis and Bartonella infection is present. The 2023 Duke-ISCVID criteria for diagnosing infective endocarditis include positive Bartonella serologies as a major diagnostic criterion, and immune-complex-mediated glomerulonephritis itself is a minor criterion (25). In this case, however, insufficient criteria were met to make the diagnosis of definite infective endocarditis. Features meeting criteria for diagnosis of infective endocarditis in this case were the microbiologic evidence of B. henselae infection, immune-complex-mediated glomerulonephritis, and fever (one major and two minor criteria). Overt signs of cardiac involvement (e.g., vegetations or other valvular abnormalities seen on cardiac imaging studies) were absent. It should be noted that this does not exclude a potential role for endocarditis in the pathophysiology of this patient’s infection. A subclinical and/or remote B. henselae endocarditis could have facilitated dissemination of the organism and resulted in glomerulonephritis. From a diagnostic standpoint, however, this case shows that B. henselae should still be considered in cases of glomerulonephritis even in the absence of a diagnosis of a concurrent endocarditis.
Glomerulonephritis associated with Bartonella infection is challenging to diagnose from both the clinical and histopathological perspectives. Delayed diagnosis and treatment could result in significant complications for immunosuppressed patients. As such, consideration of bartonellosis should be prioritized in cases of glomerulonephritis in patients with epidemiological links to Bartonella, especially in immunosuppressed individuals such as solid organ transplant recipients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mira P, Theel ES. 2024. Update on common Bartonella infections. Clin Microbiol Newsl 47:1–8. doi:10.1016/j.clinmicnews.2024.05.002 · doi ↗
- 2Okaro U, Addisu A, Casanas B, Anderson B. 2017. Bartonella species, an emerging cause of blood-culture-negative endocarditis. Clin Microbiol Rev 30:709–746. doi:10.1128/CMR.00013-1728490579 PMC 5475225 · doi ↗ · pubmed ↗
- 3Guptill L, Wu C-C, Hogen Esch H, Slater LN, Glickman N, Dunham A, Syme H, Glickman L. 2004. Prevalence, risk factors, and genetic diversity of Bartonella henselae infections in pet cats in four regions of the United States. J Clin Microbiol 42:652–659. doi:10.1128/JCM.42.2.652-659.200414766832 PMC 344466 · doi ↗ · pubmed ↗
- 4Psarros G, Riddell J, Gandhi T, Kauffman CA, Cinti SK. 2012. Bartonella henselae infections in solid organ transplant recipients: report of 5 cases and review of the literature. Medicine (Baltimore) 91:111–121. doi:10.1097/MD.0b 013e 31824 dc 07a 22391473 · doi ↗ · pubmed ↗
- 5Bos F, Chauveau B, Ruel J, Fontant G, Campistron E, Meunier C, Jambon F, Moreau K, Delmas Y, Couzi L, Korbi S, Charrier M, Viallard J-F, Luciani L, Merville P, Lazaro E, Kaminski H. 2022. Serious and atypical presentations of Bartonella henselae infection in kidney transplant recipients. Open Forum Infect Dis 9:ofac 059. doi:10.1093/ofid/ofac 05935211636 PMC 8863078 · doi ↗ · pubmed ↗
- 6Andrian T, Novel-Catin E, Triffault-Fillit C, Rabeyrin M, Barba C, Koppe L, Fouque D. 2022. Crescentic glomerulonephritis with anti-PR 3 ANCA associated with Bartonella henselae infective endocarditis. Clin Kidney J 15:1966–1968. doi:10.1093/ckj/sfac 11736158150 PMC 9494545 · doi ↗ · pubmed ↗
- 7Babiker A, El Hag MI, Perez C. 2018. Bartonella infectious endocarditis associated with cryoglobulinemia and multifocal proliferative glomerulonephritis. Open Forum Infect Dis 5:ofy 186. doi:10.1093/ofid/ofy 18630151411 PMC 6101537 · doi ↗ · pubmed ↗
- 8Bookman I, Scholey JW, Jassal SV, Lajoie G, Herzenberg AM. 2004. Necrotizing glomerulonephritis caused by Bartonella henselae endocarditis. Am J Kidney Dis 43:e 25–e 30. doi:10.1053/j.ajkd.2003.10.02714750122 · doi ↗ · pubmed ↗