Lymphatic filariasis remained silent until presentation with huge abdominal mass mimicking malignancy: a case report
S. Kafle, B. Panthi

TL;DR
A man in Nepal was diagnosed with lymphatic filariasis after presenting with a large abdominal mass that initially appeared to be cancer.
Contribution
This case report highlights an unusual presentation of lymphatic filariasis mimicking abdominal malignancy.
Findings
A 50-year-old male presented with a large mesenteric cystic mass resembling malignancy.
Cytopathological analysis confirmed the presence of Wuchereria bancrofti microfilaria larvae.
The patient improved with diethylcarbamazine treatment without further surgery.
Abstract
Lymphatic filariasis (LF) is an endemic infection seen in the tropical and subtropical regions of the world, including Nepal. It is a mosquito-borne neglected tropical disease and is caused by a nematode parasite. We reported an unusual case of LF in a 50-year-old male who presented to a tertiary hospital in Kathmandu with a complaint of a palpable abdominal mass mimicking malignancy. A CT scan revealed a large mesenteric cystic mass measuring approximately 23 × 15 cm. These findings initially directed the clinicians toward a diagnosis of malignancy, leading to blood tests for cancer markers, for example, carcinoembryonic antigen, which showed slight elevation supportive of this suspicion. Given the cystic nature of the mass and intestinal obstruction, surgical intervention was performed to place a pigtail catheter for drainage, and a fluid sample was sent for cytopathological…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig 1
Fig 1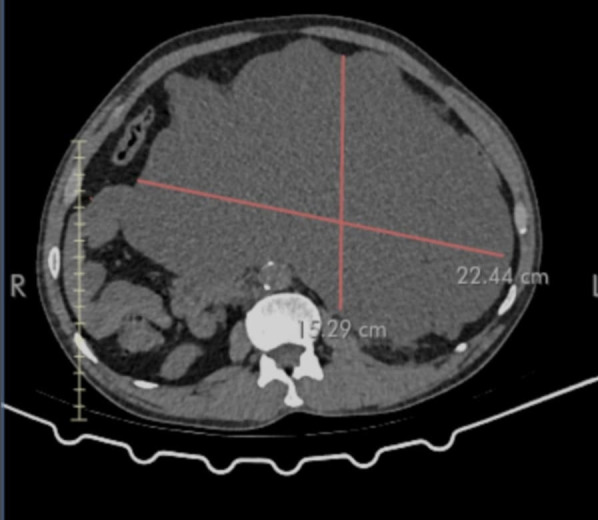 Fig 2
Fig 2 Fig 3
Fig 3| Test | Result | Unit | Reference range |
|---|---|---|---|
| CEA | 7.84 | ng/mL | <3.0 ng/mL |
| CA19.9 | <2 | Unit/mL | <37 unit/mL |
| Amylase | 39 | Unit/L | 25–125 Unit/L |
| Lipase | 42 | Unit/L | 0–160 Unit/L |
| Triacylglycerol | 0.6 | Mmol/L | 0.5–1.8 mmol/L |
| Species | Length (μm) | Key diagnostic morphologic features |
|---|---|---|
|
| 244–296 | Usually colorless sheath (Giemsa), anucleate tail, short headspace and relatively loose nuclear column |
|
| 177–230 | Usually hot-pink sheath (Giemsa), terminal and subterminal tail nuclei separated by large gaps and long headspace |
|
| 310 (avg) | Usually colorless sheath (Giemsa), terminal and subterminal tail nuclei separated by large gaps and long headspace |
|
| 304–315 | Sheath never present, tail tapered and often flexed and anucleate |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic Diseases Research and Treatment · Insects and Parasite Interactions · Parasite Biology and Host Interactions
INTRODUCTION
Lymphatic filariasis (LF) is a neglected tropical disease transmitted by mosquitoes. It is caused by various species of nematode parasite, common of them is Wuchereria bancrofti, which accounts for 90% of the cases. Some other parasites are Brugia malayi or Brugia timori (1). Mosquitoes acquire microfilariae when they feed on an infected host. The microfilariae then develop into infective larvae that are transmitted to humans during subsequent bites. It resides in the lymphatic system and can survive for 6–8 years, and releases millions of microfilariae into the bloodstream (2). The clinical features of LF are mainly related directly to the occlusion of lymphatic vessels, causing lymphangiectasia (3). It can be subclinical or cause various symptoms like hydrocele, lymphedema, elephantiasis, and acute episodes of inflammation in the lymph nodes (4). Rarely, it can present as a mesenteric cyst and may be associated with lymphatic malformations, trauma, or infections and may be asymptomatic or present with intestinal obstruction mimicking malignancy (5–7).
In Nepal, currently, 63 out of the 77 districts are endemic to filariasis, with the Tarai and subtropical regions being the most affected, which have favorable mosquito breeding conditions. The government of Nepal has launched the National Filariasis Elimination Program in 2003, aiming to eliminate LF as a public health issue by 2020. The goal was later extended to 2030 to align with the global targets set by the World Health Organization (WHO). The program targets mass drug administration (MDA) and morbidity management and disability prevention related to filariasis. It had already conducted the MDA program, administering a combination of diethylcarbamazine (DEC) and albendazole to at-risk populations once a year for six years. Additionally, it has introduced new programs using a triple-drug regimen of ivermectin, DEC, and albendazole in select districts (8). Nepal is still suffering from the curable and preventable disease—filariasis.
Here, we report an unusual presentation of LF as a mesenteric cystic lesion, whose diagnosis was confirmed by the demonstration of the microfilariae larva in the cytopathological analysis of cyst fluid.
This case report has been reported in line with the SCARE criteria (9).
CASE PRESENTATION
A 50-year-old male from a nearby hilly region presented to the emergency department of Tribhuvan University Teaching Hospital, a tertiary hospital in Kathmandu, with a complaint of an abdominal mass causing acute intestinal obstruction. He complained of severe abdominal pain, vomiting, and constipation for just 2 days. He did not have fever, chills, or weight loss. There was no history of past medical illness requiring hospital admission or any history of abdominal trauma or surgeries. He also denied any shortness of breath, chest pain, or dysuria. Vital signs were stable.
Physical examination revealed a distended abdomen with mild upper abdominal tenderness, mild guarding, and reduced bowel sounds. Murphy’s sign was negative, and there was no rebound tenderness or hepatosplenomegaly. Routine blood investigations were within normal limits. An X-ray of the abdomen showed dilated loops of the small bowel. Ultrasound of the abdomen showed an approximately 11.9 × 6.6 cm-sized multiloculated cystic lesion with internal septations in the retroperitoneum extending to the peritoneal cavity (Fig. 1). Computed tomography scan of abdomen and pelvis revealed a larger, heterogeneous, well-defined mass (22.44 × 15.29 cm) in the mesenteric region with suspicion of malignancy (Fig. 2).
Ultrasound of the abdomen showed a mass of size 11.9 × 6.6 cm with multiloculated cyst having septations.
A computed tomography scan of the abdomen and pelvis revealed a larger, heterogeneous well-defined mass (22.44 × 15.29 cm) in the mesenteric region.
A diagnosis of acute partial small bowel obstruction secondary to a mesenteric mass was made, and the patient was admitted to the surgical ward. The patient was initially managed conservatively with nil per oral, nasogastric tube insertion, intravenous fluids, antiemetics, and analgesics. Further laboratory workup revealed normal amylase, lipase, CA-19.9, and triglyceride levels, shown in Table 1. Carcinoembryonic antigen (CEA) was 7.84, which was slightly increased, supporting the suspicion of malignancy.
Peripheral blood smear revealed normal findings. Due to the persistent obstruction, an ultrasound-guided 12 F locking pigtail was introduced into the mesenteric cyst, and the cyst fluid was sent for biochemical, microbiological, and cytopathological studies. Initially, biochemical and microbiological findings were normal. However, the cytopathological study of fluid stained with Giemsa and Papanicolaou revealed multiple threadlike microfilaria larva, the morphology of which resembled Wuchereria bancrofti, confirming the diagnosis of LF (Fig. 3).
Microfilaria (larval stage of filarial parasite) in a Giemsa-stained cytopathological smear under oil immersion microscopic view (1000×).
Microbiological analysis was consistent with our diagnosis stated as “microfilaria identified- morphological consistent with Wuchereria bancrofti.”
Post-pigtail insertion, the patient developed features of acute hemorrhagic shock, for which he was shifted to intensive care and managed meticulously with IV fluids, blood transfusion, analgesics, antibiotics for possible peritonitis, and careful monitoring. Albendazole 400 mg single dose along with DEC 300 mg per oral per day after meal was given for 12 days. The patient showed significant improvement after the initiation of DEC therapy. His abdominal pain subsided, bowel sounds returned, and he was discharged from the hospital in a stable condition on day 7. On follow-up after the 12th day of commencement of DEC, the patient showed a significant symptomatic response.
DISCUSSION
The clinical features of LF are mainly due to the occlusion of lymphatic vessels, causing lymphangiectasia and W. bancrofti, which is common in Asia, mainly presents with lymphangitis, fever, elephantiasis, hydrocele, and chyluria (3, 10). Presenting as an acute abdominal condition is very rarely seen (11). Our case presented as a mesenteric cyst. Such cases are extremely rare and may present as an intra-abdominal mass (5, 7). Despite clinical signs suggesting an acute abdominal pathology, initial laboratory tests, including complete blood count with differential and serum amylase, were done as stated by Roufosse et al. (12) and were within normal limits, similar to the cases reported by Metha et al. (11). Imaging findings, including ultrasonography and contrast-enhanced CT scan, are very effective in identify the benign as well as malignant lesions (11, 13). However, despite extensive imaging evaluation, the diagnosis can only be made after pathological analysis of cyst fluid, which was also supported by the findings in our case (6, 11).
On cytopathology as well as histopathology, especially with hematoxylin and eosin stains (H&E stain) and Giemsa stain, the microfilariae are identified as thread-like organisms having terminal and subterminal nuclei in the tail region (14). Our case, W. bancrofti in Giemsa-stained slide, was with colorless sheath, short headspace, and the tail was anucleate and tapered to a point. The nuclear column was loose, and individual nuclei could be visualized throughout the column (Fig. 3). These features were typical and differentiated from similar microfilaria like B. malayi, B. timori, and Onchocerca, which have been illustrated in tabulated form in Table 2 (15).
Albendazole in combination with DEC is effective at treating LF in endemic areas. It works by clearing microfilariae and sterilizing adult filarial worms and is also used as a preventive chemotherapy strategy for the elimination of LF in a MDA program (2). Alternative drugs like doxycycline (a filaricidal drug with anti-Wolbachia action) could result in a successful eradication of microfilaricidal burden. Most filarial parasites of humans such as W. bancrofti, B. malayi, and Oncocerca spp depend on endosymbiotic Wolbachia bacteria for growth, development, fertility, and survival, whereas the host nematode likely supplies amino acids needed for Wolbachia’s development. Doxycycline permanently sterilizes female worms and reduces the adult worm longevity, inducing potent macrofilaricidal activity by the killing of adult worms. These properties are superior to other anti-filarial drugs like DEC, ivermectin, and albendazole having limited activity against adults and predominantly acting against the microfilaria progeny of female worms (16).
Usually, drug therapy is sufficient enough to resolve the symptoms and reduce the size of the cyst. However, in cases with larger size or chemotherapy resistance and with persistent obstruction, surgical removal may be the ultimate management (5). In our case, although the cyst size was large, premedical pigtail drainage already reduced the size of the cyst, and no further surgical intervention was required after medical therapy.
LF may remain asymptomatic for decades, and it may present with an abdominal mass mimicking malignancy. This case report emphasized the significance of considering LF as a differential diagnosis in patients presenting with abdominal mass or symptoms of acute intestinal obstruction, particularly in endemic areas.
Highlights
–Lymphatic filariasis (LF) is a mosquito-borne neglected tropical disease and is caused by a nematode parasite.–Various symptoms include hydrocele, lymphedema, elephantiasis, and acute episodes of inflammation in the lymph nodes, and rarely mesenteric cysts.–Mesenteric cysts can present as intra-abdominal masses mimicking malignancy.–Albendazole in combination with diethylcarbamazine is effective at treating LF in endemic areas–LF could be a differential diagnosis in acute abdominal mass with suspicion of malignancy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Newman TE, Juergens AL. 2023. Filariasis. Stat Pearls, Treasure Island (FL).
- 2World Health Organization. Lymphatic filariasis. Available from: https://www.who.int/news-room/fact-sheets/detail/lymphatic-filariasis. Retrieved 1414 Apr April 2025. Accessed , 1414 Apr April 2025
- 3Szuba A, Rockson SG. 1998. Lymphedema: classification, diagnosis and therapy. Vasc Med 3:145–156. doi:10.1177/1358836 X 98003002099796078 · doi ↗ · pubmed ↗
- 4Fauci AS, Braunwald E, Isselbacher KJ, Wilson JD, Martin JB, Kasper DL. 2001. Harrison’s principles of internal medicine. 15th ed, p 1238. Mc Graw Hill, New York.
- 5Kapoor AK, Puri SK, Arora A, Upreti L, Puri AS. 2011. Case report: filariasis presenting as an intra-abdominal cyst. Indian J Radiol Imaging 21:18–20. doi:10.4103/0971-3026.7604821431027 PMC 3056363 · doi ↗ · pubmed ↗
- 6Alqurashi HE, Alaryni AA, Alsairafi RA, Alharbi AM, Alaqla AA, Alqurashi H. 2023. Mesenteric cyst: a case report. Cureus 15:e 34325. doi:10.7759/cureus.3432536865967 PMC 9972503 · doi ↗ · pubmed ↗
- 7Ayas MF, Affas S, Hoilat GJ, Kassab I, Barawi M. 2020. A case of a mesenteric cyst mimicking a biloma. Gastroenterol Res 13:279–282. doi:10.14740/gr 1336 PMC 778127333447307 · doi ↗ · pubmed ↗
- 8Government of Nepal. Available from: https://dohs.gov.np/posts/single/lymphatic-filariasis-program. Retrieved 14 Apr 2025.