Micro‐CT for the differentiation between live birth and stillbirth: A pilot study
Giovanni Botta, Tullio Genova, Alessandro Bonsignore, Francesca Buffelli, Federico Davide Mussano, Francesco Lupariello

TL;DR
This pilot study explores using micro-CT to distinguish between live births and stillbirths by analyzing lung aeration, offering a potential alternative to traditional methods.
Contribution
The study introduces micro-CT as a novel, non-destructive method for detecting pulmonary aeration in forensic investigations.
Findings
Aerated lungs showed a mean gas volume percentage of 9.52 ± 6.77, while nonaerated lungs showed 0.58 ± 0.66.
Micro-CT can qualitatively and quantitatively detect pulmonary aeration in formalin-fixed samples.
The method may be useful in forensic cases involving neonaticide, feticide, and intrauterine fetal demise.
Abstract
The distinction between live births and stillbirths is crucial for determining the appropriate legal consequences. Historically, researchers have operated under the principle that an infant's lungs will be filled with air upon death, whereas a fetus's lungs will not. The flotation test for the lungs is the primary method still used in many jurisdictions. However, there are concerns regarding its reliability. For this reason, we conducted a pilot study to evaluate the feasibility of postmortem micro‐computed tomography (micro‐CT) for differentiating between formalin‐fixed aerated and nonaerated lungs. Lung samples from aerated (Group 1) and nonaerated (Group 2) subjects were scanned using micro‐CT. We calculated the gas volume percentage (GV%) in each sample. Group 1 (aerated lungs) showed a mean GV% of 9.52 ± 6.77, while Group 2 (nonaerated lungs) showed a mean GV% of 0.58 ± 0.66. These…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
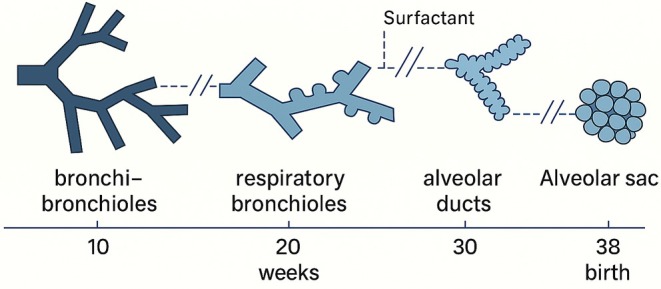 FIGURE 1
FIGURE 1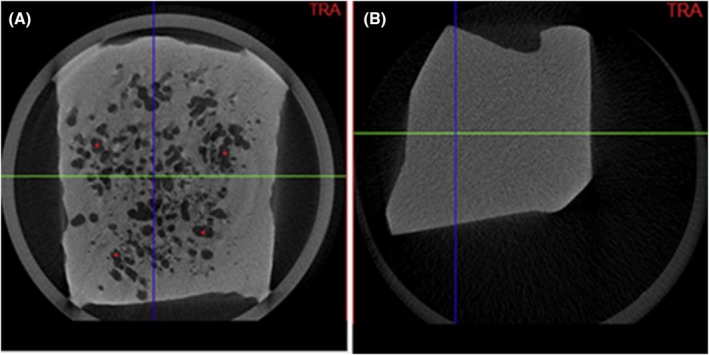 FIGURE 2
FIGURE 2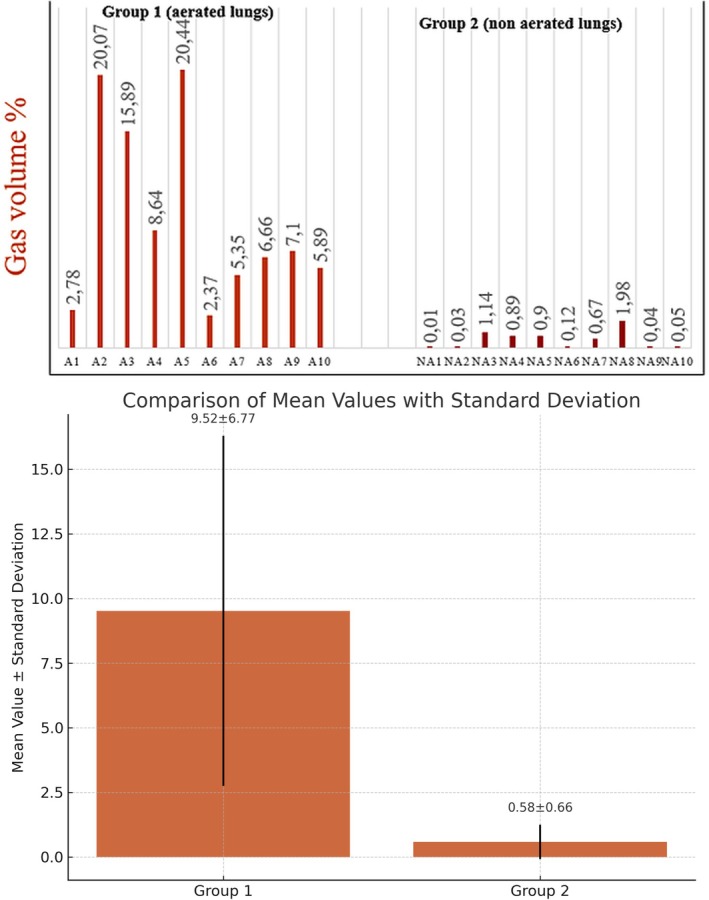 FIGURE 3
FIGURE 3| Sample | Age | Cause of death | Gestational age at birth | Execution of artificial ventilation | Presence of malformations/abnormalities |
|---|---|---|---|---|---|
| A1 | 76 years | Pulmonary thrombosis | Not applicable | Not applicable | Not applicable |
| A2 | 50 years | Traffic accident | Not applicable | Not applicable | Not applicable |
| A3 | 54 years | Traffic accident | Not applicable | Not applicable | Not applicable |
| A4 | 63 years | Acute myocardial infarction | Not applicable | Not applicable | Not applicable |
| A5 | 62 years | Ventricular arrhythmia | Not applicable | Not applicable | Not applicable |
| A6 | 1 day | Acute respiratory insufficiency due to pulmonary immaturity | 26 | Yes | No |
| A7 | 1 day | Sepsis | 38 | Yes | No |
| A8 | A few hours | Fetomaternal transfusion | 40 | No | No |
| A9 | 1 day | Nontraumatic cerebral hemorrhage | 28 | Yes | No |
| A10 | A few hours | Nontraumatic cerebral hemorrhage | 27 | Yes | No |
| Sample | Gestational age | Cause of stillbirth | Time that lasted between the demise and the autopsy | Execution of artificial ventilation | Presence of malformations/abnormalities |
|---|---|---|---|---|---|
| NA 1 | 38 + 6 | Placental abruption | 24 h | No | No |
| NA 2 | 33 | Fetomaternal transfusion | 24 h | No | No |
| NA 3 | 33 | Fetomaternal transfusion | 5 days | No | No |
| NA 4 | 39 | Umbilical knots | 5 days | No | No |
| NA 5 | 32 | Intrauterine growth restriction due to placental causes | 24 h | Yes | No |
| NA 6 | 36 | Placental abruption | 24 h | No | No |
| NA 7 | 35 + 2 | Umbilical knots | 5 days | No | No |
| NA 8 | 24 | Sepsis due to intrauterine bacterial infection | 24 h | No | No |
| NA 9 | 41 + 1 | Umbilical knots | 24 h | No | No |
| NA 10 | 38 | Fetomaternal transfusion | 24 h | No | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHomicide, Infanticide, and Child Abuse · Restraint-Related Deaths · Child Abuse and Related Trauma
Highlights
- Micro‐CT detects and quantifies lung gas, helping distinguish live birth from stillbirth.
- This method could provide a quantitative alternative to the traditional flotation test.
- Aerated lungs: GV% >2.75%; nonaerated: GV% <1.24%.
- Gas volume does not necessarily determine live versus nonlive birth.
INTRODUCTION
1
Neonaticide refers to the act of killing an infant within 24 h after birth. It is the most common form of infanticide, with the highest risk occurring on the first day of life [1]. In most jurisdictions worldwide, neonaticide is subject to significantly harsher legal penalties than feticide, making the distinction between the two critically important in medico‐legal investigations [1, 2].
Furthermore, this distinction may carry implications beyond criminal justice; for example, in civil contexts such as inheritance rights or insurance claims, determining whether the infant was born alive may influence legal recognition of personhood [1, 2]. This becomes particularly relevant in cases involving alleged medical malpractice in obstetrics, where establishing whether the infant was born alive or stillborn is crucial to determining the economic compensation owed by insurance providers.
In cases of suspected neonaticide, data obtained from a forensic autopsy can help establish: (1) the gestational age of the infant, to assess potential viability; (2) whether the infant was born alive or stillborn—an important distinction that assists legal professionals in differentiating between neonaticide, feticide, or natural deaths associated with an intrauterine fetal demise (IUFD); and (3) the cause of death [1, 3, 4].
However, establishing whether a neonate was born alive or stillborn remains particularly challenging. This determination is typically based on evidence collected at the scene, witness accounts, and postmortem analysis [3, 4]. Among the methods available, the flotation test for the lungs remains the most commonly used diagnostic tool in many jurisdictions. This test, which dates back to the observation that the lungs of a newborn who had breathed would float in water, is still employed despite its limitations [1, 3, 5]. The test is based on the assumption that aerated lungs float, while nonaerated lungs sink. However, it provides only indirect evidence of respiration.
Importantly, the flotation test does not directly demonstrate the presence of air in the lungs; rather, it indicates the presence of material with a density lower than water. As such, the test is susceptible to false positives due to the presence of other low‐density substances such as decomposition gases or air introduced during resuscitative efforts. This aspect must always be considered when interpreting a positive result—especially in legal proceedings where a diagnosis of live birth may carry severe consequences for the accused [1, 5, 6, 7].
In this context, alternative radiological methods may offer further objective criteria for lung aeration. Computed tomography (CT), widely used in clinical diagnostics since the 1970s, enables the differentiation of tissues based on radiodensity, with water set at 0 and air at −1000 Hounsfield units [1, 3, 5, 8]. This principle allows the identification of aerated versus nonaerated tissues, a concept that has been extended to postmortem investigations. Although conventional postmortem CT has demonstrated effectiveness in identifying lung gas patterns [1, 3], its resolution is limited to voxel sizes of about 1 mm^3^. In contrast, micro‐CT offers submicron resolution and has recently gained attention in various biomedical applications [9, 10]. Despite its potential, micro‐CT remains nonstandard in clinical and forensic settings due to long acquisition times, the need for mechanical stabilization, and the limitation to small sample sizes [9, 10].
Considering the above, we propose a pilot study to explore a new method for qualitatively and quantitatively distinguishing between aerated and nonaerated lungs using micro‐CT. In this manuscript, we highlight the technical aspects related to the use of micro‐CT in this field, as this application has not yet been addressed in the existing literature [7].
MATERIALS AND METHODS
2
We analyzed two groups of lung samples. Group 1 consisted of the lungs from five neonates and five adults, which were aerated (refer to Table 1). Group 2 included ten fetuses (Table 2), free of malformations at the level of the lung structure, with a gestational age between 24 and 41 weeks; therefore, characterized by both the saccular phase and the alveolar phase as shown in the following figure (see Figure 1).
Graphical representation of the development of alveolar spaces as gestational weeks progress.
For each case included in the study (see Tables 1 and 2), we collected a set of clinical and pathological data and recorded them in a dedicated Excel spreadsheet. The data collection process differed slightly between the two study groups, based on the characteristics of the subjects.
-
Group 1 (aerated lungs, five adult individuals and five neonates):
-
For the adult cases, we recorded the age at death and the documented cause of death.
-
For the neonatal cases, we recorded the following variables: age at death, cause of death, gestational age at birth, whether artificial ventilation had been performed (yes/no), and the presence or absence of malformations or structural abnormalities of the lungs (yes/no).
-
bGroup 2 (nonaerated lungs, fetal cases):
-
For each fetus, we recorded the gestational age at birth, the cause of stillbirth, the time interval between the intrauterine demise and the autopsy, whether artificial ventilation had been attempted after delivery (yes/no), and the presence or absence of pulmonary malformations or abnormalities (yes/no).
In all cases, a lung tissue sample was obtained from the apex of the right lung. Each sample measured approximately 2 cubic centimeters. All lungs had been entirely fixed in formalin prior to the sampling procedure. The apical region was chosen because it is typically the most aerated part of the lung, thus maximizing the potential to detect differences in gas distribution between the two groups.
Each sample was scanned using micro‐CT (X‐ray microtomography and SkyScan1172 Bruker) without the application of any staining compounds. The acquisition time was set to 2 h. Subsequently, we used specialized software (CTVox) for the analysis.
In the first step of our analysis, we examined the scans of the samples to determine whether the micro‐CT could identify gas within the formalin‐fixed lung samples. We calculated the radiodensity, expressed on the Hounsfield scale, using CTVox.
The second step involved identifying a quantitative measure that could serve as an indicator of the gas present in each sample, helping us distinguish between aerated and nonaerated lungs. To quantify the gas volume present in each sample, we used the software CTVox to calculate a value representing the total gas volume about the entire volume of the sample. We determined the percentage of gas volume (GV%) using the following formula: GV% = gas volume (GV) divided by the entire volume (EV) of the sample multiplied by 100; GV% = (GV/EV) × 100. We calculated the mean and standard deviation of GV% values for each group using Excel statistical formulas.
In the third step, we conducted a preliminary comparison between Group 1 and Group 2 using the previously mentioned quantitative data.
RESULTS
3
Table 1 details the individual characteristics of the cases included in Group 1 (aerated lungs), comprising five adults and five neonates. For adult cases, data reported include age at death and certified cause of death. For neonatal cases, the dataset includes age at death, cause of death, gestational age at birth, artificial ventilation status (performed: yes/no), and the presence or absence of pulmonary malformations or structural abnormalities.
Table 2 provides the corresponding data for Group 2 (nonaerated lungs), consisting of ten fetal cases. For each fetus, we documented gestational age, cause of intrauterine death, time interval between fetal demise and autopsy, artificial ventilation status postdelivery (yes/no), and the presence or absence of morphological abnormalities affecting the lungs.
Figure 2 shows that the scans could qualitatively identify gas in formalin‐fixed lung samples. This was also confirmed by calculating the radiodensity of each sample using the CTVox software and the Hounsfield scale. Nonaerated samples showed little or no gas, while aerated samples contained gas (Figure 2).
Micro‐CT scans of a Group 1 (A) sample and Group 2 sample (B); in A, aerated areas are visible ().*
For each sample, we calculated GV%. This value directly represents the gas volume relative to the entire volume of each sample. Thus, the result from the GV% formula is independent of the overall sample volume, which is essential for enabling direct comparisons between samples of different sizes. The results of the GV% formula are graphically represented in Figure 3. The means and standard deviations of GV% values were respectively: 9.52 ± 6.77 for Group 1 and 0.58 ± 0.66 for Group 2 (see Figure 3).
Graphic representation of the GV% of each sample of both groups, means, and standard deviations. A, aerated; NA, nonaerated.
Based on the mean and standard deviation values for Group 1 (mean = 9.52; SD = 6.77), none of the individual samples fell below the lower bound of the mean minus one standard deviation (i.e., 2.75). This suggests that the distribution, although dispersed, remains entirely above this threshold, indicating an overall shift of the dataset toward higher values.
According to the mean and standard deviation values for Group 2 (mean = 0.58; SD = 0.66), none of the individual samples exceeded the upper bound defined by the mean plus one standard deviation (i.e., 1.24). This indicated that the dataset was not only characterized by low central values but also tightly clustered within a narrow range, with no extreme high values observed. However, the standard deviation was slightly influenced by five out of ten cases showing lung gas volumes above the group mean (i.e., >0.58%) but still within the upper bound of 1.24%. The remaining five cases had gas volume percentages ranging from 0.01% to 0.12%, markedly lower than the group mean. A detailed review of the five higher cases suggested potential postmortem factors contributing to gas presence (see Table 2). In one case, the fetus underwent artificial ventilation after expulsion from the uterus. In three cases, autopsies were performed 5 days after fetal demise, allowing time for bacterial proliferation and gas formation. In the final case, fetal death was attributed to an infectious process, which may also have led to intrapulmonary gas accumulation through bacterial activity (Table 2).
DISCUSSION
4
In our study, micro‐CT scans successfully distinguished aerated lungs from nonaerated fetal lungs, as supported by radiodensity values (Figure 2). GV% allowed standardized comparisons across samples, with Group 1 showing higher and more dispersed values (9.52 ± 6.77), and Group 2 showing lower and tightly clustered values (0.58 ± 0.66) (Figure 3). All Group 1 values were above 2.75%, confirming a shift toward higher gas content. Group 2 values remained below 1.24%, though five cases slightly above the mean were linked to postmortem factors such as artificial ventilation, delayed autopsy, or infection (Table 2). These findings support the potential of micro‐CT as a reliable tool for assessing pulmonary aeration in forensic contexts.
Building on these results, this pilot study further highlights that micro‐CT is a promising method for differentiating between aerated and nonaerated lungs. Notably, the lengthy scanning process, the need for mechanical stabilization, and the capacity to analyze small samples do not represent limiting factors for this type of analysis. Additionally, micro‐CT can examine samples without requiring staining compounds, which eliminates the need for complex processing or significant modifications to the samples. Furthermore, this technique can study formalin‐fixed samples, allowing for later revisions. The ability to analyze lungs from already formalin‐fixed and stored organs is a significant advantage compared to conventional CT, as it enables case revision after autopsies have been completed. The preservation of air spaces occurs because formalin, being an aqueous solution, does not dissolve or compress existing gas bubbles within tissues. Instead, it fixes the surrounding tissue structure, effectively “locking in” any air that was present at the time of fixation. Moreover, formalin solution inhibits the proliferation of most microorganisms by alkylating proteins and bonding with the nitrogen atoms in purine bases. This action reduces the postmortem production of gas [11].
CONCLUSIONS
5
In conclusion, this analysis indicates that micro‐CT imaging can detect the presence of gas in the lungs and calculate gas volume percentages, which can be useful for comparison. Our sample size is still too small to establish a definitive cut‐off value for scientific and forensic applications. Similar considerations also apply to understanding the potential effects of death causes and postmortem changes on lung gas content. These preliminary findings provide a basis for future research to determine how micro‐CT might differentiate between live births and stillbirths in forensic practice.
CONFLICT OF INTEREST STATEMENT
The authors have no conflict of interest to state.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sieswerda‐Hoogendoorn T , Soerdjbalie‐Maikoe V , Maes A , van Rijn RR . The value of post‐mortem CT in neonaticide in case of severe decomposition: description of 12 cases. Forensic Sci Int. 2013;233(1–3):298–303. 10.1016/j.forsciint.2013.09.023 24314533 · doi ↗ · pubmed ↗
- 2Porter T , Gavin H . Infanticide and neonaticide: a review of 40 years of research literature on incidence and causes. Trauma Violence Abuse. 2010;11(3):99–112. 10.1177/1524838010371950 20554502 · doi ↗ · pubmed ↗
- 3Michiue T , Ishikawa T , Kawamoto O , Sogawa N , Oritani S , Maeda H . Postmortem CT investigation of air/gas distribution in the lungs and gastrointestinal tracts of newborn infants: a serial case study with regard to still‐ and live birth. Forensic Sci Int. 2013;226(1–3):74–80. 10.1016/j.forsciint.2012.12.011 23290297 · doi ↗ · pubmed ↗
- 4Schulte B , Rothschild MA , Vennemann M , Banaschak S . Examination of (suspected) neonaticides in Germany: a critical report on a comparative study. Int J Legal Med. 2013;127(3):621–625. 10.1007/s 00414-013-0841-8 23471590 · doi ↗ · pubmed ↗
- 5Guddat SS , Gapert R , Tsokos M , Oesterhelweg L . Proof of live birth using postmortem multislice computed tomography (pm MSCT) in cases of suspected neonaticide: advantages of diagnostic imaging compared to conventional autopsy. Forensic Sci Med Pathol. 2013;9(1):3–12. 10.1007/s 12024-012-9361-y 22760696 · doi ↗ · pubmed ↗
- 6Moar JJ . The hydrostatic test—a valid method of determining live birth? Am J Forensic Med Pathol. 1997;18(1):109–110. 10.1097/00000433-199703000-00027 9095314 · doi ↗ · pubmed ↗
- 7Phillips B , Ong BB . “Was the infant born alive?” A review of postmortem techniques used to determine live birth in cases of suspected neonaticide. Acad Forensic Pathol. 2018;8(4):874–893. 10.1177/1925362118821476 31240078 PMC 6491538 · doi ↗ · pubmed ↗
- 8Kirby M , Smith BM . Quantitative CT scan imaging of the airways for diagnosis and management of lung disease. Chest. 2023;164(5):1150–1158. 10.1016/j.chest.2023.02.044 36871841 PMC 10792293 · doi ↗ · pubmed ↗