Self‐help cognitive behavioral therapy for gaze anxiety in young adults: Protocol of a 3‐arms, multicenter, randomized controlled trial
Kazuki Matsumoto, Sayo Hamatani, Yoshifumi Mizuno, Akiko Maeno, Makiko Kasai, Katsunori Watanabe, Rio Kamashita, Naomi Sunami, Masatoshi Ikeda, Shinobu Nagata, Masahiko Inoue, Yasuhiro Kimura, Mizue Yokoo, Yoshihiko Kunisato, Yasuaki Akasaki, Masayuki Nakamura

TL;DR
This study will test if self-help cognitive behavioral therapy can reduce gaze anxiety in young adults.
Contribution
The study introduces a randomized trial comparing two self-help CBT formats for gaze anxiety.
Findings
The trial will assess the effectiveness of self-help CBT for reducing gaze anxiety severity.
Results will determine if self-help CBT improves access to treatment for young adults with social anxiety.
Findings will be evaluated using mixed-effects models over a 6-month follow-up period.
Abstract
Gaze anxiety (scopophobia) is a frequently observed and reported symptom that is closely associated with social anxiety disorder (SAD). Considering the efficacy of cognitive behavioral therapy (CBT) for social anxiety, it may also be beneficial for individuals with gaze anxiety. Self‐help CBT can offer a means of early intervention; however, its effectiveness remains unclear. This protocol describes the design of a clinical trial aimed at evaluating the efficacy of two self‐help CBT interventions for gaze anxiety. This multicenter randomized controlled trial is planned across 12 institutions in Japan. The participants will be young adults aged 18–30 years who report anxiety and avoidance related to gazes. The enrolled participants will be randomly assigned to either a self‐help book CBT group, a web‐based CBT group, or a control group. The severity of gaze anxiety, as the primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
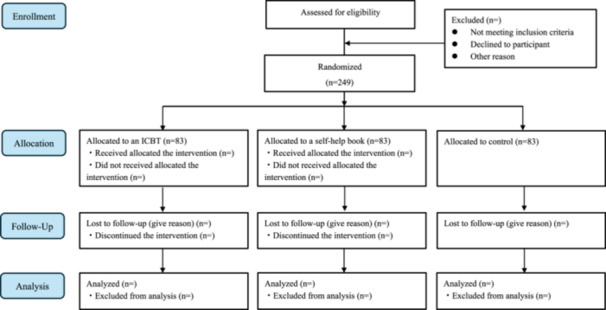 Figure 1
Figure 1| Week | Title each chapter | Introduced techniques | Page |
|---|---|---|---|
| 1 | Why do I feel anxious when people look at me? | Psychoeducation | 31 |
| 2 | Understanding the roots of your gaze anxiety | Cognitive behavioral model | 21 |
| 3 | Steps to overcoming your gaze anxiety |
Examining safety behaviors Video feedback Attention shift training Behavioral experiments Social/opinion surveys Ceasing rumination and pre‐ and post‐event processing Processing social trauma in image description | 81 |
| 4 | Let's conquer social situations one by one: Case studies |
Anxiety about being seen trembling Fear of making public mistakes and being observed Fear of blushing when looked at Fear of saying the wrong thing and being judged | 56 |
| 5 | As your “gaze anxiety” improves | Relapse prevention | 2 |
| Week | Module |
|---|---|
| 1 | Psychoeducation and case‐formulation using the cognitive behavioral model |
| 2 | Examining safety behaviors and self‐focused attention |
| 3 | Video feedback to correct negative self‐image |
| 4 | Attention shift training |
| 5 | Behavioral experiments |
| 6 | Opinion survey |
| 7 | Ceasing rumination and pre‐ and post‐event processing |
| 8 | Processing social trauma in image description |
| 9 | Schema work |
| 10 | Relapse prevention |
| Outcome | Description |
|---|---|
| LSAS‐j | The LSAS‐j includes 24 social situations related to “fear or anxiety” and “avoidance,” which participants rank on a 4‐point scale (0 = never, 4 = severe), has a total score range of 0–144. |
| SPIN | The SPIN is a self‐rating scale that measures 3 characteristic aspects of SAD: fear, avoidance, and physiological arousal. |
| PHQ‐9 | Depressive symptoms will be assessed using the Japanese version of the PHQ‐9. |
| GAD‐7 | Generalized anxiety will be assessed using the Japanese version of the GAD‐7. |
- —2024 Kagoshima University Young Researcher Support Grant
- —JSPS KAKENHI
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnxiety, Depression, Psychometrics, Treatment, Cognitive Processes · Digital Mental Health Interventions · Child and Adolescent Psychosocial and Emotional Development
INTRODUCTION
Social anxiety disorder (SAD) is a mental disorder characterized by excessive fear of scrutiny and potential embarrassment in social situations, along with anxiety about negative evaluation by others.1 SAD commonly onsets during adolescence and has a lifetime prevalence of approximately 4.0%.2 Adults and children with SAD tend to avoid eye contact,3, 4 and the tendency seems to appear in adolescence due to excessive gaze anxiety.5 Being looked at often signals the start of interaction in social situations. If gaze anxiety is severe and leads to the avoidance of others, habituation to gaze anxiety may not occur. This can maintain or even worsen gaze and social anxiety. Therefore, early intervention for people with gaze anxiety before it interferes with their daily lives is important.
Individual cognitive behavioral therapy (CBT) for SAD is significantly effective and has been recommended as a treatment option in treatment guidelines.6, 7, 8, 9 However, it is unclear how to effectively deliver this promising treatment for preventive interventions. The reason for this is that individual CBT generally has high time and monetary costs. Self‐help CBT is potentially feasible for reducing gaze anxiety, similar to its effectiveness in treating SAD. Self‐help CBT, which people can perform at home, eliminates the need to miss school or university and has lower implementation costs because there is no therapist facilitating individual sessions. For social anxiety in adolescents and young adults, self‐help CBT on websites has been shown to have an effect; however, it is unclear whether it helps with gaze anxiety.10 Self‐help CBT via books without therapist guidance has been shown to improve SAD in two previous randomized controlled trials (RCTs).11, 12 However, there is limited evidence from RCTs in Asia. Furthermore, the efficacy of self‐help CBT for treating gaze anxiety remains unclear.
A clinical trial was designed to examine the efficacy of a self‐help CBT using a book, developed with the aim of alleviating gaze anxiety, and an internet‐based CBT (ICBT) program for social anxiety. This manuscript details the protocol for this clinical trial.
METHODS AND ANALYSIS
Trial design
This study protocol is a multicenter RCT being conducted at 12 research institutions in Japan. Eligible participants will be randomly assigned in a 1:1:1 ratio to one of three groups: self‐help CBT book group, ICBT group, or control group (no‐treatment control).
Participants
Participants will be recruited from the following universities: Kagoshima University, University of Fukui, Shigakukan University, Naruto University of Education, Jin‐ai University, Hiroshima Cosmopolitan University, Teikyo University, Shujitsu University, Tottori University, Fukushima Gakuin University, Tokyo Rissho Junior College, and Senshu University. Additionally, participant enrollment will be solicited through the research project website. The predetermined inclusion and exclusion criteria outline the specific requirements that potential participants must meet for enrollment in the trial.
Inclusion criteria:
- 1.A total score of 10 or higher on a measure of gaze anxiety symptoms using the Gaze Anxiety Rating Scale (GARS).3
- 2.Enrollment as a university and graduate student aged between 18 and 30 years.
- 3.Capacity to send and receive electronic mail.
- 4.No planned transfer or withdrawal from their academic institution during the study period.
Exclusion criteria:
- 1.Presence of mental disorders, including but not limited to major depressive disorder and SAD.
- 2.A history of suicidal ideation or attempts.
- 3.Presence of a progressive medical illness (e.g., cancer).
- 4.Pregnancy or the immediate postpartum period.
- 5.Any condition or behavior deemed by the researchers to render the individual unsuitable for participation in this study (e.g., antisocial behavior).
For participants identified as being at risk for mental health conditions, the researchers from each university will inform the principal investigator (K.M.), who has been the study secretariat, to assess their eligibility by using the Mini‐International Neuropsychiatric Interview (MINI).13, 14
Intervention
Self‐help by using a book group
Participants allocated to the self‐guided book intervention will be instructed to read one chapter (approximately 30–50 pages) per week from the self‐help book on gaze anxiety in young adults, “Escaping the Fear and Anxiety of Others' Gaze.”15 This self‐help book was authored by the first author (K.M.) and published in October 2024. Table 1 presents the contents of the chapters of the self‐help book. This book has 193 pages long with wide line spacing, and we estimate it takes approximately 150 min to read. Each Monday at noon, participants in this group will automatically receive an announcement detailing the chapters to read for the week and words of encouragement.
Self‐help in ICBT group
Participants allocated to this intervention group will be instructed to engage using their own devices in an ICBT program designed to ameliorate social anxiety in adolescents and young adults. The completion of one module per week will be recommended, and automated email reminders encouraging program engagement will be sent to participants every Monday morning. The ICBT program was developed by the first author (K.M.) on the e‐learning platform learningBOX (learningBOX Inc., Tatsuno, Japan). The ICBT program is based on the model proposed by Clark and Wells.16 The program comprises 10 training sessions focusing on CBT components that are efficacious for SAD. Each module is expected to take about 15 min to complete, and the entire content can be finished in about 150 min. Table 2 outlines the treatment modules of the ICBT program.
Control group
The control group will receive no active intervention during the study period; however, the self‐help book will be sent via mail to the participants upon study completion. While participants in the control group will be permitted to seek usual care, such as counseling, they will be asked to refrain from accessing information specifically related to CBT.
Outcome
All outcome measures will be structured as web‐based questionnaires and sent to the participants' email addresses at baseline, post‐intervention (5 weeks follow‐up), 3 months follow‐up, and 6 months follow‐up. To promote participant retention and follow‐up completion, monthly email reminders will be sent from the start of the intervention until the end of the follow‐up period. Any deviations from the trial intervention will be recorded during follow‐up assessments.
The primary outcome will be the GARS used to measure the severity of clinical symptoms and rate anxiety/fear and avoidance of gaze. The GARS comprises 17 items regarding social situations involving focused gaze.3 For each item, participants will rate the degree of anxiety/fear and the frequency of avoidance on a scale from 0 (“no anxiety” or “no avoidance”) to 3 (“a lot of anxiety” or “avoid a lot”). The total GARS score ranges from 0 to 102, with higher scores indicating a greater severity of gaze anxiety. The validity and reliability of the GARS have been demonstrated in the original English and German versions.3, 17, 18 The Japanese version of the Gaze Anxiety Rating Scale (GARS‐j) was developed through translation into Japanese by the first author (K.M.) and back‐translation by the second author (S.H.), with the resulting text being reviewed by the original scale developers (please refer to the GARS‐j in the Supporting Information).19 Furthermore, the validity of the GARS‐j will be examined using baseline responses from this trial. Table 3 shows secondary outcomes.
Sample size
The sample size for this study was set at 249 (Figure 1), considering the following GPower estimated values and a 20% attrition rate (version 3.1.9.7; The GPower Team).30, 31 We set the parameters for the F tests—anova: fixed effects, omnibus, one‐way, with an effect size F = 0.25 (medium), an α error probability of 0.05, and a power (1 − β error probability) of 0.9 for three groups. These inputs yielded a noncentrality parameter of 12.94, a critical F of 3.04, an original total sample size of 207, and an actual power of 0.902.
CONSORT flow diagram showing allocation in the three groups. ICBT, internet‐based cognitive behavioral therapy.
Randomization
Eligible participants will be randomly assigned to each group at a ratio of 1:1:1, with assignments made using a block randomization method with R' “randomizr” package,32 ensuring a balance in baseline Japanese version of the Liebowitz Social Anxiety Scale (LSAS‐j) total scores of <50 or ≥50, sex (male or female), and facilities as adjustment factors. Allocation by using the randomizer will be conducted by the second author (S.H.). The randomization sequence will be concealed from researchers at each university, and the statistician will remain blinded to participants' group assignments.
Blinding
This trial will not be blinded.
Adverse events
We will instruct all participants at each university to immediately report any adverse events that occur during this trial period. If additional support is needed, participants will be referred to campus counseling services or encouraged to visit local clinics affiliated with their universities. Even if no adverse events are reported, participants scoring 10 or above on the Patient Health Questionnaire‐9 (PHQ‐9) total score during the follow‐up period will assess their mental health problem by using the MINI.13, 26 Based on the results of this assessment, participants may be recommended to see a medical doctor.
Adherence
We will assess adherence to the two interventions using two methods. In the book group, participants will be asked to report the chapters of the self‐help book read and cognitive‐behavioral techniques practiced in daily life at the initial outcome assessment. For the web‐based CBT intervention, the e‐learning system will record completed treatment modules automatically, and participants will also report cognitive‐behavioral techniques practiced in daily life at the initial outcome assessment. All participants, including the control group, will be asked to report any unintended treatments or care received during the study period.
Statistical analysis plan
Statistical analyses will be performed by the second author (S.H.) using IBM spss Statistics (IBM Corp., Armonk, NY, USA) and will adhere to the intention‐to‐treat principle. The analyst was not involved in creating the two intervention programs. The analyst will be concealed to group allocation when accessing the data. This means she will not know which specific intervention a group received or if each participant was in the control condition.
Descriptive statistics will be used to summarize demographic data (including participants' age and sex) and the severity of clinical symptoms on each scale. Group differences will be compared to determine statistical significance. As a primary analysis, mixed‐effects models will examine significant differences in the mean change in total scores on each symptom rating scale between the groups from baseline to Week 5 (1 month), Week 13 (3 months), and Week 26 (6 months) post‐intervention. If an overall significant difference is found, multiple comparisons will be conducted. For multiple comparisons, we will implement Dunnett's test to control for inflated Type I error rates.33 Effect sizes will be calculated between and within the groups. The significance level for hypothesis testing will be set at a two‐tailed α of 0.05, and 95% two‐sided confidence intervals will be calculated.
For the binary variables of treatment response, remission, and worsening, the odds and risk ratios between the groups will be analyzed using Fisher's exact test. To further evaluate the risk of worsening social anxiety, as measured by the LSAS, we will calculate the risk ratio, relative risk reduction, absolute risk reduction, and number needed to treat.
We plan to conduct a sensitivity analysis excluding participants with insufficient engagement in the self‐help intervention and those who provided implausible response patterns—specifically, patterns like straight‐lining, contradictory responses, or inconsistent responses between the GARS‐j and the LSAS‐j. Participants will be defined as having sufficient engagement if those in the self‐help book group have completed at least two chapters, and those in the ICBT group have reached the “Behavioral Experiments” treatment module. The sensitivity analysis, similar to the primary analysis, will be performed after imputing missing values using R's “mice” package.34
Ethics and dissemination
The trial protocol was approved by the Institutional Review Board of Kagoshima University Hospital (Approval Number: 240229). This clinical trial was registered at the University Hospital Medical Information Network Center (UMIN), and an overview of the research protocol is publicly available (UMIN000057484). This study's intervention program addresses cognitions and behavioral habits related to gaze and social situations that participants may find distressing, while also promoting the practice of social skills. During the research explanation, participants will be informed that they can contact researchers at any time and that they have the right to withdraw consent at any point.
RESULTS
The clinical trial will be conducted from April 1, 2025, to March 31, 2026. The case registration period will be scheduled for 2 months, from April 1 to May 31, 2025. The results of this trial, in conjunction with the execution of the predesigned statistical analyses plan, will provide novel knowledge into the effectiveness of self‐help CBT for gaze anxiety (scopophobia).
DISCUSSION
The limitations of this study include the inability to determine the true effects of the two self‐help CBT programs because the control is not a placebo (sham treatment). Because recruitment for this study will take place at universities affiliated with researchers specializing in CBT, many potential participants will have a clinical psychology background and may be able to discern the researchers' intentions if an attention control or psychoeducation condition is used as a placebo. This is because the lectures will have explained that CBT is an effective treatment for SAD, and they can find out through an internet search that CBT for SAD is covered by insurance in Japan. On the other hand, a no‐treatment control group could lead participants to seek treatment outside the study, including face‐to‐face CBT, during the observation period. Furthermore, disappointed participants might withdraw from the study, which could increase the risk of bias. Given these practical constraints, we believe it is more appropriate for the control group to be guaranteed an intervention (self‐book CBT) after the study.
Another potential limitation is that the outcomes are self‐rated psychological scales; therefore, the potential influence of positive expectations resulting from the intervention on the outcomes cannot be excluded.35 Self‐report outcomes may be susceptible to bias due to reliance on respondents' subjectivity and memory. The protocol mitigates this by employing outcomes comprising specific, behaviorally anchored questions (e.g., the GARS‐j and the LSAS‐j), which clearly define the timeframe and frequency of symptoms and aim to facilitate participants' accurate reporting of their actual symptoms. To minimize recall bias, links to the online questionnaires will be promptly emailed to participants at each assessment point. The online format of responses may also reduce socially desirable responses compared with in‐person assessments.36 This may encourage participants to report their actual clinical symptoms without hesitation.
This trial excludes participants with a formal diagnosis of SAD during screening. Consequently, the evidence presented will pertain to a non‐clinical population (young adults at high risk), which will limit its generalizability to clinical settings. The efficacy of those interventions for gaze anxiety in individuals already diagnosed with SAD should therefore be verified in a clinical setting.
This trial protocol has several strengths. Outcomes will be assessed not only post‐intervention but also at the 6‐month follow‐up, which should enhance the estimation of true effectiveness. The ITT principle allows for the derivation of unbiased conclusions regarding the effectiveness of the intervention.37 The sensitivity analyses could show the robustness of the results from the primary analysis.38 The statistical analysis plan will evaluate both continuous outcome data and clinically meaningful categorical variables (treatment response, remission, and worsening). Furthermore, the multisite design across numerous Japanese research institutions aims to achieve an adequate sample size and mitigate selection and facility biases.
This trial protocol was designed to investigate the efficacy of self‐help CBT programs on gaze and social anxiety in young adults. Despite some limitations, the multiple strengths could yield novel evidence.
AUTHOR CONTRIBUTIONS
All authors contributed to the development of this trial protocol or the formulation of the statistical analysis plan, critically reviewed this manuscript, and approved the paper for submission.
CONFLICT OF INTEREST STATEMENT
The first author (K.M.) is the author of the self‐help book used in one of the interventions. The other authors declare no conflicts of interest.
ETHICS APPROVAL STATEMENT
This clinical trial protocol has been approved by the Institutional Review Board of Kagoshima University Hospital, through review (Approval Number: 240229). This clinical trial is registered in the University Hospital Medical Information Network Center, and an overview of the research protocol is publicly available (UMIN000057484).
PATIENT CONSENT STATEMENT
N/A.
CLINICAL TRIAL REGISTRATION
University Hospital Medical Information Network (UMIN) 000057484; https://center6.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000065681.
Supporting information
Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stein MB , Stein DJ . Social anxiety disorder. Lancet. 2008;371(9618):1115–1125.18374843 10.1016/S 0140-6736(08)60488-2 · doi ↗ · pubmed ↗
- 2Stein DJ , Lim CCW , Roest AM , de Jonge P , Aguilar‐Gaxiola S , Al‐Hamzawi A , et al. The cross‐national epidemiology of social anxiety disorder: data from the World Mental Health Survey Initiative. BMC Med. 2017;15(1):143.28756776 10.1186/s 12916-017-0889-2PMC 5535284 · doi ↗ · pubmed ↗
- 3Schneier FR , Rodebaugh TL , Blanco C , Lewin H , Liebowitz MR . Fear and avoidance of eye contact in social anxiety disorder. Compr Psychiatry. 2011;52(1):81–87. 10.1016/j.comppsych.2010.04.006 21220069 PMC 9731729 · doi ↗ · pubmed ↗
- 4Kley H , Tuschen‐Caffier B , Heinrichs N . Safety behaviors, self‐focused attention and negative thinking in children with social anxiety disorder, socially anxious and non‐anxious children. J Behav Ther Exp Psychiatry. 2012;43(1):548–555. 10.1016/j.jbtep.2011.07.008 21831344 · doi ↗ · pubmed ↗
- 5Chen J , van den Bos E , Westenberg PM . A systematic review of visual avoidance of faces in socially anxious individuals: influence of severity, type of social situation, and development. J Anxiety Disord. 2020;70:102193. 10.1016/j.janxdis.2020.102193 32058889 · doi ↗ · pubmed ↗
- 6Carpenter JK , Andrews LA , Witcraft SM , Powers MB , Smits JAJ , Hofmann SG . Cognitive behavioral therapy for anxiety and related disorders: a meta‐analysis of randomized placebo‐controlled trials. Depress Anxiety. 2018;35(6):502–514.29451967 10.1002/da.22728 PMC 5992015 · doi ↗ · pubmed ↗
- 7Hoffman SG , Smits JAJ . Cognitive‐behavioral therapy for adult anxiety disorders: a meta‐analysis of randomized placebo‐controlled trials. J Clin Psychiatry. 2008;69(4):621–632.18363421 10.4088/jcp.v 69n 0415 PMC 2409267 · doi ↗ · pubmed ↗
- 8National Institute for Health and Care Exvellence . Social anxiety disorder: recognition, assessment and treatment. Clinical guideline (CG 159). 2013. https://www.nice.org.uk/guidance/cg 159 39960994 · pubmed ↗