Hepatocellular Carcinoma Confined to the Bile Duct without Hepatic Mass or Jaundice: A Case Report
Yuto Aoki, Masato Yoshioka, Yohei Kaneya, Kazuhiko Endo, Ryo Ga, Mampei Kawashima, Toshiyuki Irie, Junji Ueda, Tetsuya Shimizu, Youichi Kawano, Yukio Oshiro, Yoshiharu Nakamura, Hiroshi Yoshida

TL;DR
A rare case of liver cancer growing only in the bile duct without a mass or jaundice is reported, showing that early surgery can lead to good outcomes.
Contribution
This is the third reported case of HCC confined to the bile duct without a mass or jaundice, highlighting a rare clinical presentation and successful treatment.
Findings
HCC can present as intraductal growth without a hepatic mass or jaundice, mimicking cholangiocarcinoma.
Early surgical resection may result in favorable long-term outcomes for this rare form of HCC.
Immunohistochemistry confirmed HCC diagnosis with positive HepPar1 and negative cytokeratin 19.
Abstract
Hepatocellular carcinoma (HCC) presents as a hepatic mass and may involve vascular invasion or extrahepatic spread. However, intraductal growth within the intrahepatic bile duct is rare and is often associated with obstructive jaundice. HCCs confined to the intrahepatic bile duct without detectable hepatic mass or jaundice are rare, and diagnosis is often difficult due to clinical and radiological resemblance to perihilar cholangiocarcinoma. Moreover, such cases generally carry a poor prognosis. We report a rare case of HCC that developed exclusively within the intrahepatic bile ducts, without forming a detectable mass in the liver or causing jaundice. A 70-year-old man presented with right hypochondriac pain. Imaging revealed dilation of the intrahepatic bile ducts in the anterior sector and intraductal filling defects, particularly in the intrahepatic bile duct branch of segment 8,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
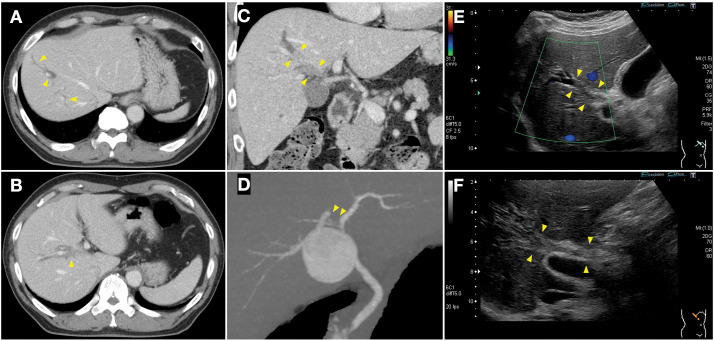 Fig. 1
Fig. 1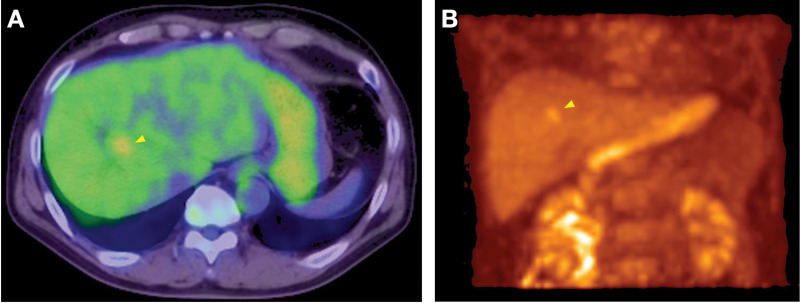 Fig. 2
Fig. 2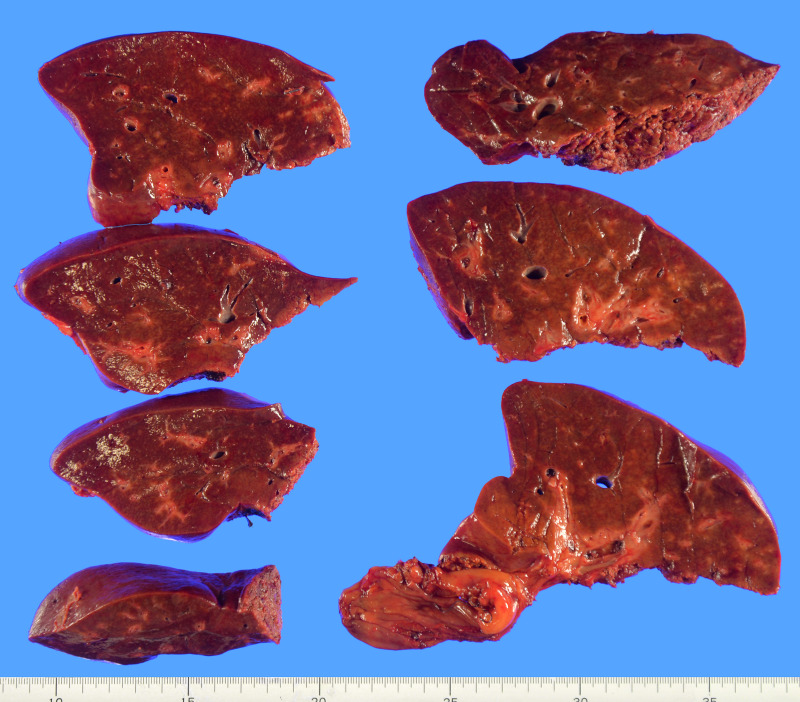 Fig. 3
Fig. 3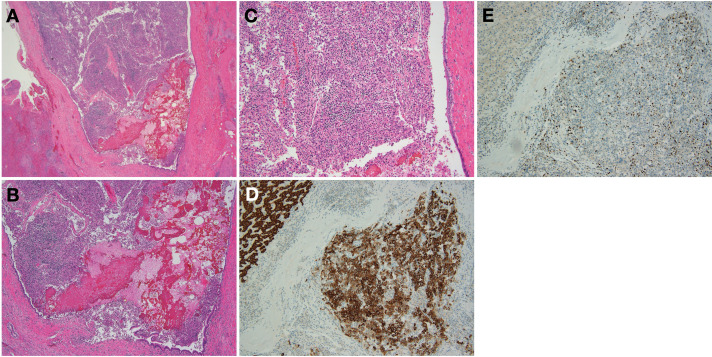 Fig. 4
Fig. 4| Parameter | Result | Unit |
|---|---|---|
| WBC | 10600 | /µL |
| RBC | 4.67 | 106/µL |
| Hb | 15.4 | g/dL |
| Ht | 45.6 | % |
| Plt | 318 | 103/µL |
| TP | 7.7 | g/dL |
| Alb | 4.4 | g/dL |
| T-Bil | 1.31 | mg/dL |
| D-Bil | 0.5 | mg/dL |
| AST | 67 | U/L |
| ALT | 73 | U/L |
| ALP | 648 | U/L |
| GGT | 859 | U/L |
| CRP | 1.50 | mg/dL |
| PT% | 109.1 | % |
| PT-INR | 0.96 | |
| APTT | 29.3 | sec. |
| D dimer | 0.7 | µg/mL |
| CEA | 4.4 | ng/mL |
| CA19-9 | 12.5 | U/mL |
| DUPAN-2 | 701 | U/mL |
| AFP | 61.9 | ng/mL |
| PIVKA-II | 27.2 | mAU/mL |
| ICGR15 | 5.6 | % |
| KICG | 0.192 |
| Author, Year | Age | Sex | Chief complaint | Jaundice | Hepatic mass | Risk Factor | T-Bil | AFP | PIVKA-II | Tumor location | Initial/Recurrence | Preoperative diagnosis | Pathological diagnosis | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kondo, 2003 | 55 | Female | General fatigue | No | Absent | None | 1 | <5 | ND | Right anterior intrahepatic bile duct | Initial | Bile duct carcinoma | Poorly differentiated HCC | Recurrence at 4 m and died at 5 m |
| Kondo, 2003 | 35 | Male | Jaundice and epigastric pain | Yes | Absent | HBV | 1.9 | 6 | 9 | Left hepatic duct | Initial | Bile duct carcinoma | Poorly differentiated HCC | Recurrence at 8 m and died at 3 y |
| Makino, 2006 | 70 | Male | Jaundice | Yes | Absent | HCV | ND | 9 | 19200 | Common bile duct–left hepatic duct | Initial | Bile duct carcinoma | Well-differentiated HCC | Recurrence-free at 1 y |
| Chang, 2010 | 54 | Male | Jaundice and right upper abdominal pain | Yes | Absent | HBV | 12.6 | Normal range | ND | Common bile duct | Initial | Bile duct carcinoma | HCC | Recurrence at 2 w, died at 1 m |
| Abe, 2012 | 72 | Female | None (routine checkup after HCC treatment) | No | Absent | HCV | ND | 2.9 | 13 | Right anterior intrahepatic bile duct | Recurrence | Recurrent HCC or bile duct carcinoma | Poorly differentiated HCC (HCC recurrence in bile duct) | Recurrence-free at 1 y |
| Alshati, 2019 | 40 | Male | Jaundice, upper quadrant pain and weight loss | Yes | Absent | HBV | 3.2 | 73.95 | ND | Left hepatic duct | Initial | HCC (biopsy via ERCP) | Poorly differentiated HCC | ND |
| Nakashima, 2025 | 74 | Male | None (routine checkup after HCV treatment) | No | Absent | HCV | Normal range | Normal range | 512 | B2–B3 | Initial | Intrahepatic cholangiocarcinoma | HCC | Recurrence at 6 m |
| Present case (Aoki, 2025) | 70 | Male | Epigastric pain | No | Absent | HCV | 1.31 | 109.1 | 27.2 | Right hepatic duct–B8 | Initial | Perihilar cholangiocarcinoma | Poorly differentiated HCC | Recurrence-free at 2 y 7 m |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Hepatocellular Carcinoma Treatment and Prognosis · Pediatric Hepatobiliary Diseases and Treatments
Abbreviations
AFP alpha-fetoprotein CA19-9 carbohydrate antigen 19-9 CEA carcinoembryonic antigen DIC-CT drip-infusion cholangiography CT DUPAN-2 Duke pancreatic monoclonal antigen type 2 EOB-MRI gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid–enhanced magnetic resonance imaging FDG fluorodeoxyglucose FLR future liver remnant HCC hepatocellular carcinoma HCV hepatitis C virus KICG kinetic indocyanine green elimination rate constant MRCP magnetic resonance cholangiopancreatography PIVKA-II prothrombin induced by vitamin K absence or antagonist-II US ultrasonography
INTRODUCTION
HCC usually presents as a liver mass that spreads through intrahepatic vascular invasion, which occurs in 15%–57% of surgically resected or transplanted cases.^1)^ By contrast, intraductal extension is relatively uncommon, observed in only 2.3%–13% of surgical and autopsy cases,^2,3)^ and is associated with poor prognosis.^4)^ Patients with intraductal extension often present with obstructive jaundice and are frequently misdiagnosed as having cholangiocarcinoma.
A few reports have described HCC with intraductal involvement in the absence of a liver mass; however, such cases are extremely rare and diagnostically challenging. Here, we present a rare case of primary HCC that manifested solely as an intraductal lesion, with no detectable hepatic mass or jaundice. Notably, the patient achieved long-term recurrence-free survival following surgery, suggesting that early intervention may offer favorable outcomes in select cases.
CASE PRESENTATION
A 70-year-old man presented to the emergency department with pain in the right hypochondrium. Non-contrast abdominal CT revealed localized dilation of the intrahepatic bile ducts, and the patient was referred to our hospital for further evaluation. Contrast-enhanced CT and abdominal US revealed dilated bile ducts in the anterior section and solid components occupying the right hepatic duct and the bile duct branch of segment 8. Coronal reconstructed CT clearly demonstrated the intraductal lesion and upstream bile duct dilatation. DIC-CT showed absence of contrast filling in the B7–8 and common bile duct stump branches, whereas other segments, including B6 and the left hepatic ducts, were normally opacified, with no evidence of choledocholithiasis (Fig. 1).
Preoperative imaging studies. (A–C) Contrast-enhanced CT (CECT). The intrahepatic bile ducts of the anterior section are dilated (A), and solid components fill the right hepatic duct and bile duct at the origin of segment B8 (B). Coronal reconstructed CECT clearly showing the intraductal lesion and upstream bile duct dilatation (C). (D) Drip infusion cholangiographic CT. A filling defect can be observed in the right hepatic duct; however, the bile ducts in the anterior section are not visualized. (E, F) Abdominal ultrasonography. Solid components can also be observed within the right hepatic and bile ducts at the origin of B8, with peripheral intrahepatic bile duct dilation. Arrowheads indicate the location of the intraductal lesion in all panels.
FDG-PET demonstrated abnormal uptake along the intrahepatic bile duct from segment 8 to the hepatic hilum (SUVmax 3.6–4.1), without evidence of lymph node or distant metastasis (Fig. 2). EOB-MRI, MRCP, and endoscopic US were not performed.
Fluorodeoxyglucose (FDG)-PET/CT findings. (A) FDG-PET/CT showing abnormal uptake along the intrahepatic bile duct from segment 8 to the hepatic hilum (SUVmax 3.6–4.1). (B) Maximum intensity projection image confirming absence of lymph node or distant metastasis. Arrowheads indicate the location of the intraductal lesion in all panels.
Laboratory investigations indicated normal CA19-9 and CEA levels, with elevated AFP and DUPAN-2. PIVKA-II levels were within normal limits (Table 1). Serological tests revealed positivity for anti-HCV antibody, while hepatitis B surface antigen and hepatitis B core antibody were negative.
Imaging and intraoperative findings confirmed tumor involvement of the right hepatic duct and the bile duct branch of segment 8, resulting in widespread bile duct dilatation throughout the right anterior sector. Complete oncological clearance and an adequate surgical margin required right hepatectomy with extrahepatic bile duct resection. Preoperative CT volumetry showed an FLR ratio of 32%, which was considered insufficient. Therefore, right portal vein embolization was performed via the ileocecal vein. After embolization, the FLR increased to 41.7%, with an estimated remnant KICG value (Krem) of 0.0767, deemed acceptable for safe resection. The patient subsequently underwent right hepatectomy and extrahepatic bile duct resection with Roux-en-Y hepaticojejunostomy. Intraoperative US revealed no hepatic masses; however, bile duct stenosis was observed. Gross examination of the resected specimen showed no distinct tumors within the liver parenchyma (Fig. 3).
Resected specimen. Macroscopic examination of the resected liver shows no detectable tumor in the hepatic parenchyma.
Histopathological examination revealed that the tumor was mainly located within the lumen of the intrahepatic bile duct and exhibited poorly differentiated hepatocellular carcinoma morphology. Although no gross hepatic parenchymal mass was identified, microscopic foci of tumor infiltration into the adjacent liver parenchyma were observed in a trabecular growth pattern without capsule or septum formation. Importantly, the tumor was not continuous with the bile duct epithelium but proliferated within the bile duct lumen.
Elastic Van Gieson staining confirmed vascular invasion, with tumor cells identified in small branches of the portal vein (Vp1) and hepatic vein (Vv1), whereas no hepatic arterial invasion (Va0) was detected. The background liver showed mild fibrosis (F1) and moderate inflammatory activity (A2), without significant steatosis or cirrhosis. Immunohistochemically, the tumor cells were positive for HepPar1 and negative for CK19, with a Ki-67 labeling index of approximately 40%, confirming the diagnosis of HCC (Fig. 4).
Histopathological findings. (A) Clusters of atypical cells are observed within the bile duct lumen (hematoxylin and eosin, ×20). (B, C) Atypical cells with pleomorphic polygonal morphology resembling hepatocyte-like cells. Cells infiltrate the surrounding hepatic parenchyma in a sponge-like trabecular pattern without forming a capsule or fibrous septum (hematoxylin and eosin, (B) ×40; (C) ×100). (D) Immunohistochemistry shows strong positivity for HepPar1 (×100). (E) The Ki-67 labeling index is approximately 40% (×100). These findings support the diagnosis of hepatocellular carcinoma arising within the bile duct lumen.
The patient developed an anastomotic leak at the jejunojejunostomy site postoperatively, necessitating surgical repair. The patient recovered without further complications and was discharged on POD 27 following the initial surgery. The patient remained recurrence-free at 2 years and 7 months after surgery, after which follow-up was discontinued because of an unrelated condition.
DISCUSSION
HCC typically presents as a mass within the liver and frequently invades the portal or hepatic veins. By contrast, intraductal growth is relatively rare and considered as a poor prognostic factor.^4)^ Among such cases, some are classified as icteric-type HCC, characterized by bile duct invasion leading to obstructive jaundice.^5)^ In previously reported cases of HCC with bile duct involvement, including icteric-type HCC, a distinct mass lesion is typically present in the liver.
However, in the present case, the tumor was limited to the intrahepatic bile duct, with no identifiable liver mass or jaundice. This may represent an early stage of icteric-type HCC in which only regional bile duct obstruction is present without involvement of the hepatic or common bile ducts. Alternatively, a small intrahepatic tumor may regress or become undetectable at the time of surgery, leaving only an intrahepatic component. In our patient, it is also possible that a microscopic lesion was present but remained below the detection threshold for imaging and histopathology. Another possibility, although speculative, is that the tumor originated from ectopic hepatocytes located within the bile duct mucosa, a phenomenon previously reported in rare pathological studies.^6,7)^
The diagnosis of HCC in the absence of a detectable hepatic mass is extremely challenging. Most reported cases of such presentation initially manifest with obstructive jaundice.^6–14)^ Several cases of HCC presenting with bile duct involvement but without a detectable intrahepatic mass have been previously reported (Table 2). While most of these cases manifested with obstructive jaundice, few were reported without jaundice. True primary HCCs confined to the bile duct without intrahepatic tumors were rare, with other cases representing recurrent disease. Although a few cases of HCC confined solely to the bile duct without jaundice have been described, these include both primary and recurrent tumors.^15)^ Reports of primary HCC presenting solely as an intraductal lesion without a hepatic mass or jaundice are exceedingly rare. To the best of our knowledge, only 2 such cases fulfilling all of the following criteria have been documented: (1) a first-time pathological diagnosis of HCC (i.e., no recurrence), (2) no identifiable hepatic mass on imaging or histopathology, (3) disease confined to the bile duct, and (4) no clinical or laboratory evidence of jaundice. One such case was included in a Japanese report by Kondo et al.,^16)^ who described 2 patients with bile duct-invading HCC without detectable hepatic tumors. However, only one of these patients met all the above criteria, whereas the other presented jaundice.
A comparable case was recently reported by Nakashima et al.^17)^ in 2025, who described an HCC confined to the intrahepatic bile duct without a hepatic mass or jaundice. Despite comprehensive preoperative endoscopic evaluations including cholangioscopy and biopsy, a definitive diagnosis was not established until after surgery. Notably, the patient developed intraductal recurrence within 6 months postoperatively.
A comparable case reported by Kondo et al.^16)^ also lacked a detectable hepatic mass and jaundice; however, the patient experienced early intrahepatic recurrence and died within 5 months of surgery. By contrast, our patient remained recurrence-free for 2 years and 7 months postoperatively despite the absence of preoperative histological confirmation. These differing clinical courses suggest that intraductal HCC without hepatic parenchymal involvement may exhibit variable biological behavior and that early surgical intervention may contribute to a favorable prognosis in select cases.
Although the number of reported cases is limited, further case accumulation may help clarify whether this presentation, characterized by the absence of a hepatic mass and jaundice, represents a distinct prognostic subgroup compared with the more common bile duct-invasive HCCs associated with intrahepatic tumors and/or obstructive jaundice.
Endoscopic procedures such as cholangioscopy or bile duct biopsy also play a crucial role in establishing the diagnosis.^18)^ However, in our case, preoperative endoscopic evaluation was not feasible, and the patient underwent surgery under a presumptive diagnosis of perihilar cholangiocarcinoma. This highlights the diagnostic challenge of intraductal HCC mimicking bile duct carcinoma in the absence of a detectable hepatic mass.
Minimally invasive liver surgery, including robotic liver resection, has recently gained attention owing to its applicability in complex resections, including those involving the biliary tract. Although not applied in this case, such approaches, particularly robot-assisted hepatectomy, may offer a future surgical option for complex biliary cases where the preoperative diagnosis is inconclusive.^19)^
CONCLUSIONS
We present a rare case of HCC manifesting solely as an intraductal lesion with no detectable hepatic mass, jaundice, or prior history of HCC. The clinical and radiological findings closely resembled those of perihilar cholangiocarcinoma, highlighting the diagnostic challenges of such cases. Although, in a similar case, early recurrence has been reported,^16,17)^ our patient was recurrence-free for over 2 years and 7 months, suggesting that early surgical intervention may contribute to favorable long-term outcomes. Further case accumulation is essential to better understand prognosis and optimize diagnostic and therapeutic strategies.
These findings emphasize the importance of recognizing intraductal HCC in the differential diagnosis and suggest that prompt surgical intervention before the development of jaundice or a hepatic mass may help to improve long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rodríguez-Perálvarez M, Luong TV, Andreana L, et al. A systematic review of microvascular invasion in hepatocellular carcinoma: diagnostic and prognostic variability. Ann Surg Oncol 2013; 20: 325–39.23149850 10.1245/s 10434-012-2513-1 · doi ↗ · pubmed ↗
- 2Kojiro M, Kawabata K, Kawano Y, et al. Hepatocellular carcinoma presenting as intrabile duct tumor growth. A clinicopathologic study of 24 cases. Cancer 1982; 49: 2144–7.6280834 10.1002/1097-0142(19820515)49:10<2144::aid-cncr 2820491026>3.0.co;2-o · doi ↗ · pubmed ↗
- 3Nakashima T, Okuda K, Kojiro M, et al. Pathology of hepatocellular carcinoma in Japan: 232 consecutive cases autopsied in ten years. Cancer 1983; 51: 863–77.6295617 10.1002/1097-0142(19830301)51:5<863::aid-cncr 2820510520>3.0.co;2-d · doi ↗ · pubmed ↗
- 4Yang X, Qiu Z, Ran R, et al. Prognostic importance of bile duct invasion in surgical resection with curative intent for hepatocellular carcinoma using PSM analysis. Oncol Lett 2018; 16: 3593–602.30127966 10.3892/ol.2018.9108 PMC 6096155 · doi ↗ · pubmed ↗
- 5Lin TY, Chen KM, Chen YR, et al. Icteric type hepatoma. Med Chir Dig 1975; 4: 267–70.173942 · pubmed ↗
- 6Schmelzle M, Matthaei H, Lehwald N, et al. Extrahepatic intraductal ectopic hepatocellular carcinoma: bile duct filling defect. Hepatobiliary Pancreat Dis Int 2009; 8: 650–2.20007086 · pubmed ↗
- 7Tsushimi T, Enoki T, Harada E, et al. Ectopic hepatocellular carcinoma arising in the bile duct. J Hepatobiliary Pancreat Surg 2005; 12: 266–8.15995818 10.1007/s 00534-004-0963-y · doi ↗ · pubmed ↗
- 8Makino T, Nakamori S, Kashiwazaki M, et al. An icteric type hepatocellular carcinoma with no detectable tumor in the liver: report of a case. Surg Today 2006; 36: 633–7.16794800 10.1007/s 00595-006-3214-9 · doi ↗ · pubmed ↗