Handgrip and contralateral knee flexion strength as key predictors of daily physical activity in severe knee osteoarthritis
Daisuke Urashima, Tomofumi Kinoshita, Tatsuhiko Kutsuna, Kunihiko Watamori, Takashi Tsuda, Yusuke Horita, Kazunori Hino, Masaki Takao

TL;DR
Handgrip and contralateral knee strength are linked to higher physical activity in severe knee osteoarthritis patients.
Contribution
Identifies handgrip and contralateral knee flexion strength as predictors of physical activity in severe knee osteoarthritis.
Findings
Handgrip strength significantly correlates with activity at 3.0–3.9 METs.
Contralateral knee flexion strength predicts activity at 4.0–4.9 METs.
Abstract
Association between handgrip and knee muscle strength and physical activity in severe knee osteoarthritis In this study, factors associated with physical activity in patients with end‐stage knee osteoarthritis were investigated using a high‐precision wearable monitor. It was hypothesised that affected‐side knee muscle strength would significantly relate to objectively measured activity. A total of 58 patients with end‐stage knee osteoarthritis scheduled for total knee arthroplasty were recruited, between September 2024 and April 2025, and evaluated. Evaluations included handgrip strength, skeletal muscle index, and isokinetic knee extension and flexion strength. Daily physical activity was monitored for 1 month using a wearable device, which recorded the average time spent at different metabolic equivalent (MET) levels. Activity intensity was recorded in 0.1‐MET increments from 1.0…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1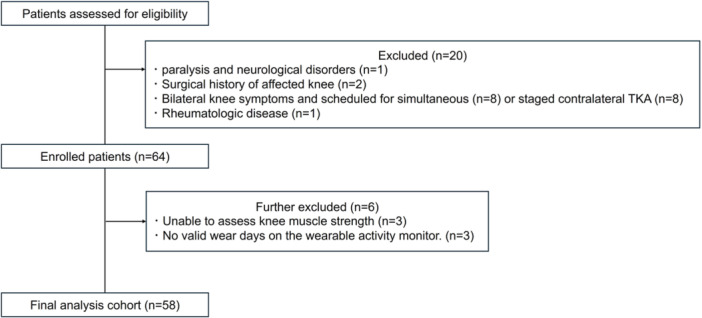 Figure 2
Figure 2| LPA (<3METs) | MVPA (≥3METs) |
|---|---|
| Sitting at a chair (1.0 METs) | Walking: 2.5mph (3.0 METs) |
| Ironing (2.0 METs) | Walking upstairs (4.7 METs) |
| Cooking (2.0 METs) | Walking: 4.0mph (5.0 METs) |
| Stretching and yoga (2.5 METs) | Jogging (7.0 METs) |
| Washing dishes (2.5 METs) | Running: 5 mph (8.3 METs) |
| Slow‐paced walking: 2.0 mph (2.8 METs) | Walking upstairs quickly (8.8 METs) |
| Mean ± SD | |
|---|---|
| Age | 64.4 ± 8.6 (45–87) |
| BMI | 26.3 ± 4.2 (16.1–35.4) |
| HKA on affected side (°) | 9.4 ± 6.0 (−13 to 24) |
| Maximum knee extension angle on the affected side (°) | −6.8 ± 6.4 (−25 to 0) |
| Maximum knee extension flexion on the affected side (°) | 121.2 ± 10.2 (90–140) |
| Median (IQR) | |
|---|---|
| Steps | 1715.6 (653.9–3310.9) |
| MVPA (min) | 38.8 (22.9–66.1) |
| 1.0–1.9 METs (min) | 517.9 (438.4–611.4) |
| 2.0–2.9 METs (min) | 157.8 (132.4–196.1) |
| 3.0–3.9 METs (min) | 35.2 (18.1–46.2) |
| 4.0–4.9 METs (min) | 5.2 (2.1–8.2) |
| 5.0–5.9 METs (min) | 1.3 (0.8–1.6) |
| 6.0–6.9 METs (min) | 0.4 (0.12–0.80) |
| 7.0–7.9 METs (min) | 0.02 (0–0.17) |
| ≥ 8.0 METs (min) | 0.03 (0–0.11) |
| Mean ± SD | |
|---|---|
| Surgical side knee extension muscle strength | 38.5 ± 19.0 |
| Contralateral side knee extension muscle strength | 45.1 ± 23.1 |
| Surgical side knee flexion muscle strength | 19.1 ± 14.4 |
| Contralateral side knee flexion muscle strength | 21.2 ± 14.6 |
| Handgrip strength | 22.3 ± 7.9 |
| SMI | 6.5 ± 1.4 |
| Physical activity | Knee muscle strength | |||||||
|---|---|---|---|---|---|---|---|---|
| Surgical side knee extension | Contralateral side knee extension | Surgical side knee flexion | Contralateral side knee flexion | |||||
|
|
|
|
|
|
|
|
| |
| Age | −0.356 | 0.006 | −0.273 | 0.038 | −0.481 | 0.0001 | −0.324 | 0.013 |
| MVPA | 0.246 | 0.062 | 0.357 | 0.005 | 0.225 | 0.088 | 0.266 | 0.043 |
| 1.0–1.9 METs | −0.061 | 0.649 | −0.049 | 0.709 | 0.061 | 0.649 | −0.013 | 0.917 |
| 2.0–2.9 METs | −0.003 | 0.981 | 0.109 | 0.413 | −0.053 | 0.691 | −0.126 | 0.345 |
| 3.0–3.9 METs | 0.231 | 0.079 | 0.335 | 0.01 | 0.202 | 0.127 | 0.228 | 0.083 |
| 4.0–4.9 METs | 0.276 | 0.035 | 0.364 | 0.004 | 0.302 | 0.021 | 0.368 | 0.004 |
| 5.0–5.9 METs | 0.196 | 0.138 | 0.269 | 0.04 | 0.153 | 0.249 | 0.271 | 0.039 |
| 6.0–6.9 METs | 0.074 | 0.576 | 0.137 | 0.304 | 0.175 | 0.186 | 0.184 | 0.166 |
| 7.0–7.9 METs | 0.003 | 0.980 | −0.002 | 0.984 | 0.047 | 0.723 | −0.075 | 0.574 |
| ≥ 8.0 METs | 0.156 | 0.240 | 0.099 | 0.455 | 0.137 | 0.493 | −0.104 | 0.603 |
| Handgrip strength | SMI | |||
|---|---|---|---|---|
|
|
|
|
| |
| Age | −0.421 | 0.001 | −0.613 | <0.0001 |
| MVPA | 0.365 | 0.004 | 0.139 | 0.295 |
| 1.0–1.9 METs | −0.045 | 0.737 | 0.017 | 0.894 |
| 2.0–2.9 METs | −0.071 | 0.592 | −0.021 | 0.874 |
| 3.0–3.9 METs | 0.347 | 0.007 | 0.121 | 0.363 |
| 4.0–4.9 METs | 0.397 | 0.002 | 0.089 | 0.503 |
| 5.0–5.9 METs | 0.245 | 0.0638 | 0.077 | 0.562 |
| 6.0–6.9 METs | 0.103 | 0.441 | 0.071 | 0.596 |
| 7.0–7.9 METs | −0.068 | 0.609 | 0.022 | 0.150 |
| ≥ 8.0 METs | 0.114 | 0.392 | 0.109 | 0.581 |
|
| 95%CI |
| ||
|---|---|---|---|---|
| Average time at 3.0–3.9 METs intensity | Age | −0.211 | −1.270 to 0.282 | 0.207 |
| Sex | 0.349 | −5.201 to 42.499 | 0.123 | |
| BMI | −0.339 | −2.995 to −0.281 | 0.019 | |
| Handgrip strength | 0.571 | 0.209–2.709 | 0.023 | |
| Average time at 4.0–4.9 METs intensity | Age | −0.294 | −0.464 to 0.010 | 0.06 |
| Sex | 0.107 | −3.036 to 6.803 | 0.446 | |
| BMI | −0.238 | −0.783 to 0.026 | 0.066 | |
| Contralateral side knee flexion muscle strength | 0.487 | 0.080–0.365 | 0.003 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOsteoarthritis Treatment and Mechanisms · Total Knee Arthroplasty Outcomes · Lower Extremity Biomechanics and Pathologies
INTRODUCTION
Muscle weakness, particularly in the quadriceps and surrounding knee musculature, is a well‐recognised factor for the onset and progression of knee osteoarthritis (KOA) [6, 16, 18]. In addition to local deficits, systemic conditions, such as sarcopenic obesity, have also been reported as risk factors [27]. Muscle weakness is biomechanically detrimental and associated with increased pain and functional limitations; insufficient thigh muscle strength has even been suggested as a predictor for eventual surgical intervention such as total knee arthroplasty (TKA) [3]. Conversely, greater knee extensor strength has been linked to a reduced risk of joint space narrowing, underscoring its protective role [21]. Taken together, these findings highlight muscle strength as central to the prevention and management of KOA. However, in patients with severe KOA awaiting TKA, it remains unclear which specific muscle strength parameters or body composition measures are most relevant for sustaining daily physical activity.
Some studies have reported associations between muscle strength and physical activity in patients with mild‐to‐moderate KOA [2, 23]. Although most studies focused on knee extensor strength, some also emphasised the importance of knee flexors [23]. However, prior studies primarily relied on temporary outcome measures such as patient‐reported outcome measure or walking tests, which might not accurately reflect actual daily activity. Clarifying how muscle strength influences objectively measured daily activity would provide valuable insights into targeted interventions to maintain function and delay disease progression in patients with KOA.
To address this research gap, a high‐precision wearable activity monitor capable of capturing metabolic equivalent (MET) intensity in fine increments was employed to investigate the associations of handgrip strength, knee muscle strength, and skeletal muscle index (SMI) with intensity‐specific physical activity. It was hypothesised that knee muscle strength on the affected side and SMI could be associated with engagement in high‐intensity physical activities. Furthermore, identifying these associations might provide clinically relevant targets for individualised preoperative rehabilitation strategies in patients with severe KOA. Ultimately, these insights might contribute to the development of more effective, individualised preoperative rehabilitation strategies for managing patients with advanced KOA.
METHODS
This prospective study was conducted in accordance with the principals of the Declaration of Helsinki and approved by the Institutional Review Board. Written informed consent was obtained from all patients. The study included patients scheduled for unilateral TKA at our institution and who did not have severe knee pain symptoms on the contralateral side. The participants were consecutively recruited between September 2024 and April 2025 from those who agreed to participate and provided informed consent. The exclusion criteria were: paralysis or neurological disorders, a prior surgical history of the affected knee joint, rheumatologic disease, or bilateral knee symptoms scheduled for simultaneous bilateral TKA or staged contralateral TKA. All patients had KOA with varus deformity. All knees had severe KOA, with Kellgren–Lawrence grade IV on the surgical side.
Daily activities
In this study, daily physical activity was monitored using a wearable physical activity monitor (Active‐style Pro HJA‐750C, Omron Healthcare, Kyoto, Japan; Figure 1) for 30 consecutive days preoperatively as the primary outcome. This device records daily step counts and time spent in physical activities, classifying activity intensity in 0.1‐MET increments starting from 1.0 MET (Table 1) [13, 15, 17]. Regarding analysis, the detected activities were categorised into the following ranges: 1.0–1.9, 2.0–2.9, 3.0–3.9, 4.0–4.9, 5.0–5.9, 6.0–6.9, 7.0–7.9 and ≥8.0 METs. The participants were instructed to wear the device for 30 days; a valid day was defined as at least 10 h of wear time, according to previous studies [28]. We then calculated the average daily step count, average time spent in physical activities ≥1.0 METs, and average daily duration of moderate‐to‐vigorous physical activity (MVPA, ≥3.0 METs) on valid days. The accuracy and validity of this device have been confirmed in previous reports [13, 15, 17].
Wearable activity monitor with a lithium coin battery. It identifies walking and daily activities, recording physical activity data every 10 s to enable detailed data analysis.
Muscle strength and body composition
Handgrip strength was measured twice in each hand using a digital dynamometer; the maximum value was adopted for analysis. SMI was assessed once using a body composition analyser (InBody 770; InBody Co., Ltd., Seoul, Japan). Knee extension and flexion strength were assessed isokinetically using a dynamometer (Cybex NORM; Cybex International, USA). The participants performed five consecutive maximal knee extension/flexion movements; the peak torque value was adopted as the representative value. These measurements were assessed 1 day before TKA as secondary outcomes.
Statistical analyses
The normality of each variable was tested using the Shapiro–Wilk test, which indicated that all physical activity measures were non‐normally distributed. Therefore, correlations between physical activity and muscle parameters (handgrip strength, SMI, and knee extension and flexion strength) were assessed by Spearman's rank correlation coefficient. To identify independent factors associated with physical activity, multiple linear regression analyses were performed with age, sex, and BMI fitted as fixed covariates, and muscle parameters as candidate predictors using a stepwise selection method. Non‐significant variables were automatically excluded from the model. Statistical significance was set at p < 0.05. All analyses were performed using SPSS Statistics version 28.0 (IBM Corp., Armonk, NY, USA). Since this was an exploratory observational study with a fixed number of available patients, an a priori power analysis was not performed.
RESULTS
During the study period, 84 patients were screened. Among these, one patient with paralysis and neurological disorder, two with a prior surgical history of the affected knee, one with rheumatologic disease, and 16 with bilateral knee symptoms scheduled for simultaneous (n = 8) or staged contralateral TKA (n = 8) were excluded. In addition, six patients were excluded due to missing muscle strength assessment (n = 3) or insufficient valid wear days with the activity monitor (n = 3). Finally, data of 58 patients (10 men and 48 women) were included in the analysis (Figure 2). The baseline characteristics are presented in Table 2.
Flowchart of patient selection and inclusion in the final analysis cohort.
The median duration of MVPA ( ≥ 3.0 METs) was 38.8 min/day (Table 3). Table 4 presents the knee extension and flexion muscle strength using knee muscle strength measurements. Using the bivariate correlation analysis, the average daily duration of activities at 4.0–4.9 METs significantly correlated with knee flexion and extension muscle strength in both the affected and contralateral sides (ρ = 0.276, 0.364, 0.302 and 0.368; p = 0.035, 0.004, 0.021 and 0.004, respectively; Table 5) and handgrip strength (ρ = 0.397, p = 0.002; Table 6). In addition, the average daily duration of MVPA significantly correlated with knee flexion and extension muscle strength in the contralateral side and handgrip strength (ρ = 0.357, 0.266 and 0.365; p = 0.005, 0.043 and 0.004, respectively; Tables 5 and 6).
In the stepwise multiple regression analysis for the average daily duration of activities at 3.0–3.9 METs, handgrip strength was determined to be a significantly associated factor (β = 0.571, p = 0.023, 95% CI: 0.209–2.709, R² = 0.175; Table 7), whereas SMI and knee muscle strength variables were excluded from the model. Furthermore, regarding intensity levels of 4.0–4.9, contralateral knee flexion strength was identified as a significant associated factor, whereas SMI, handgrip strength, affected side knee extension and flexion strength and contralateral knee extension strength were excluded from the models (β = 0.487, p = 0.003, 95% CI: 0.080–0.365, R² = 0.329; Table 7). Using the stepwise multiple regression analyses, no explanatory variables remained in the models for the average daily duration of activities at 1.0–1.9, 2.0–2.9, 5.0–5.9, 6.0–6.9, 7.0–7.9 and ≥8.0 METs, indicating that none of the candidate factors were significantly associated with these outcomes.
DISCUSSION
This study evaluated factors related to physical activity in patients with end‐stage KOA using a high‐precision wearable physical activity monitor, and the primary finding is that, in patients with end‐stage KOA, handgrip strength predicted ambulatory‐level physical activity, whereas contralateral knee flexion strength was associated with engagement in moderate‐intensity physical activity. Although previous studies have primarily focused on knee extensor strength, the present findings suggest that, in patients with severe KOA requiring TKA, contralateral knee flexor strength may have a greater influence on ambulatory function in daily life. In contrast, SMI, which reflects whole‐body muscle mass, was not significantly correlated with physical activity levels in this population. This finding was of particular interest, as it contradicted the original hypothesis. To the best of our knowledge, this is the first study to concurrently evaluate SMI, handgrip strength, and both affected and contralateral knee flexor strength and investigate their associations with objectively measured physical activity using a wearable activity monitor.
In patients with KOA who experience severe pain and mobility limitations, muscle strength has been extensively reported as a critical determinant of physical function [2, 5, 23]. Chun et al. demonstrated that in patients with severe KOA, muscle strength was the only significant factor associated with performance deterioration [2]. In the present study including patients with advanced KOA scheduled for TKA, contralateral knee flexion strength was a significant determinant of daily physical activity. Greater contralateral strength may reduce the load on the affected knee and facilitate compensatory strategies that preserve functional capacity. Similarly, Bade et al. highlighted that postoperative contralateral limb function is a key determinant of rehabilitation outcomes after TKA [1].
Previous studies have identified specific muscle groups influencing function in patients with KOA. Preoperative quadriceps strength has consistently been shown to predict walking ability and activities of daily living (ADLs) [14], while Lopes et al. reported reduced hamstring strength in patients with KOA compared with healthy individuals, emphasising its role in rehabilitation [12]. Moreover, reductions in muscle output have been linked to clinically important declines in Western Ontario and McMaster Universities Arthritis Index (WOMAC) functional activity [19]. Furthermore, improvements in hamstring strength have been associated with better WOMAC functional scores, mobility, and stair‐climb performance [20]. The present study adds to this evidence by demonstrating that contralateral knee flexion strength is associated with moderate‐intensity physical activity in patients with severe KOA. In contrast to earlier research that primarily relied on PROMs or functional tests [8, 24, 25], the use of a wearable activity monitor enabled an objective evaluation of daily activity. These findings suggest that maintaining contralateral knee flexion strength is essential for preserving ADL in patients with severe KOA, consistent with reports indicating that preoperative activity levels facilitate early postoperative recovery [5].
In addition to periarticular knee muscles, broader indicators such as handgrip strength and sarcopenia have gained attention in recent years [27]. Sarcopenic obesity has been identified as a risk factor for the onset of KOA; [26, 27] delayed postoperative recovery has been observed in patients with sarcopenia [22], highlighting the relevance of systemic muscle assessment. Among these, handgrip strength has been linked to WOMAC functional activity [11] and to stair‐climbing ability after TKA [7]. In the present study, although SMI was not significantly associated with physical activity, handgrip strength showed significant correlation with ambulatory‐level activity (3.0–3.9 METs/day). This aligns with findings in previous reports indicating that functional outcomes are more strongly influenced by muscle quality than by muscle mass alone [4, 9, 10]. The relatively advanced age of our cohort might also have contributed to the lack of association between SMI and activity. Overall, handgrip strength might serve as a practical screening tool for identifying patients at risk of reduced ADL performance in routine clinical practice.
This study has some limitations. First, the sample size was relatively small, and the cohort consisted solely of patients with severe KOA, whose physical activity levels might vary widely. Since this was an exploratory observational study with a fixed number of available patients, an a priori power analysis was not performed, which might have limited the statistical power of the study. Second, the relationship between pain and physical activity was not assessed, despite pain being a potential confounding factor. Furthermore, the observation period was restricted to the preoperative phase; thus, future studies are needed to clarify how preoperative factors, including muscle strength, influence long‐term postoperative outcomes. Another limitation of this study is that preoperative rehabilitation programs were not standardised among the participants. Detailed information on the frequency, content, and participation in rehabilitation was not available for each individual. In addition, comorbidities and preoperative physical activity indices (e.g., UCLA activity score, ASA classification, frailty index), which might influence activity levels, were not systematically collected in this study. This lack of information might have introduced residual confounding and should be addressed in future research. The major limitation of this study is that the alignment and Kellgren–Lawrence grade of the contralateral knee were not evaluated in all cases. Although we selected patients scheduled for unilateral TKA who did not report pain symptoms in the contralateral limb, structural degeneration in the contralateral knee might still have influenced physical activity. Therefore, further validation in a larger cohort with detailed assessment of contralateral alignment and Kellgren–Lawrence grade is warranted to strengthen the robustness and generalisability of findings of this study. However, previous studies have reported that patients with KOA exhibit reduced hamstring strength during both isometric and concentric contractions compared with pain‐free controls [12]. Therefore, in the present study, which included patients without contralateral knee pain, the potential influence of contralateral deformity on the results is likely to have been minimal. Despite these limitations, the findings that handgrip strength predicted lower‐intensity activity and that contralateral knee flexion strength was linked to higher‐intensity levels are relevant because they might have clinical implications in optimising preoperative and perioperative rehabilitation strategies in patients undergoing TKA.
CONCLUSION
In severe knee osteoarthritis, handgrip strength may screen patients at risk of reduced activity, while contralateral knee flexion strengthening in preoperative rehabilitation could help optimise management strategies.
AUTHOR CONTRIBUTIONS
Daisuke Urashima: Writing–original draft; investigation. Tomofumi Kinoshita: Conceptualisation; methodology; investigation; formal analysis; writing–review and editing. Kazunori Hino: investigation; writing–review and editing. Tatsuhiko Kutsuna, Kunihiko Watamori, Takashi Tsuda, and Yusuke Horita: Investigation. Masaki Takao: Conceptualisation; writing–review and editing.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
ETHICS STATEMENT
This study was approved by the Institutional Review Board of Ehime University (identification number: 2409007). All participants provided written informed consent.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bade MJ , Kittelson JM , Kohrt WM , Stevens‐Lapsley JE . Predicting functional performance and range of motion outcomes after total knee arthroplasty. Am J Phys Med Rehabil. 2014;93:579–585.24508937 10.1097/PHM.0000000000000065 PMC 4350663 · doi ↗ · pubmed ↗
- 2Chun SW , Kim KE , Jang SN , Kim KI , Paik NJ , Kim KW , et al. Muscle strength is the main associated factor of physical performance in older adults with knee osteoarthritis regardless of radiographic severity. Arch Gerontol Geriat. 2013;56:377–382.10.1016/j.archger.2012.10.01323164547 · doi ↗ · pubmed ↗
- 3Culvenor AG , Wirth W , Ruhdorfer A , Eckstein F . Thigh muscle strength predicts knee replacement risk independent of radiographic disease and pain in women: data from the Osteoarthritis Initiative. Arthritis Rheum. 2016;68:1145–1155.10.1002/art.39540 PMC 549484726663882 · doi ↗ · pubmed ↗
- 4Cho YK , Jung HN , Kim EH , Lee MJ , Park JY , Lee WJ , et al. Association between sarcopenic obesity and poor muscle quality based on muscle quality map and abdominal computed tomography. Obesity. 2023;31:1547–1557.37133436 10.1002/oby.23733 · doi ↗ · pubmed ↗
- 5Fujita R , Ota S , Yamamoto Y , Kataoka A , Warashina H , Hayashi T , et al. Factors associated with physical activity following total knee arthroplasty for knee osteoarthritis: a longitudinal study. BMC Musculoskelet Disord. 2024;25:178.38413902 10.1186/s 12891-024-07306-3PMC 10898134 · doi ↗ · pubmed ↗
- 6Gong Z , Li S , Cao P , Ruan G , Zhang Y , Zeng Q , et al. The association between quadriceps strength and synovitis in knee osteoarthritis: an exploratory study from the osteoarthritis initiative. J Rheumatol. 2023;50:548–555.36521912 10.3899/jrheum.220538 · doi ↗ · pubmed ↗
- 7Hashimoto S , Hatayama K , Terauchi M , Saito K , Higuchi H , Chikuda H . Preoperative hand‐grip strength can be a predictor of stair ascent and descent ability after total knee arthroplasty in female patients. J Orthop Sci. 2020;25:167–172.30904204 10.1016/j.jos.2019.03.003 · doi ↗ · pubmed ↗
- 8Holm PM , Kemnitz J , Bandholm T , Wernbom M , Schrøder HM , Skou ST . Muscle function tests as supportive outcome measures for performance‐based and self‐reported physical function in patients with knee osteoarthritis: exploratory analysis of baseline data from a randomized trial. J Strength Condit Res. 2022;36:2635–2642.10.1519/JSC.000000000000384033021580 · doi ↗ · pubmed ↗