Necrotizing Pneumonia Complicated by Bartonella-Associated Culture-Negative Endocarditis in an Immunocompetent Adult
Teja Koi, Patrick Yue, Ashley Huggett

TL;DR
A healthy adult developed severe lung infection and endocarditis caused by Bartonella, a hard-to-detect bacteria, highlighting the need for better diagnostic approaches.
Contribution
This case highlights the importance of considering zoonotic pathogens like Bartonella in culture-negative endocarditis.
Findings
Bartonella was diagnosed using serologic testing and echocardiography despite negative blood cultures.
The patient had necrotizing pneumonia and complications like empyema and bronchopleural fistula.
Early recognition of zoonotic pathogens is critical for effective treatment and avoiding complications.
Abstract
Bartonella-related culture-negative endocarditis (CNE) is an infrequent and difficult diagnosis, due to the organism’s unique growth characteristics and frequent negative cultures. We describe a case of a 42-year-old previously healthy male with necrotizing pneumonia complicated by empyema and bronchopleural fistula. Despite signs of systemic inflammation and infection, multiple blood cultures remained negative. Our diagnosis was made with serologic testing, which revealed elevated Bartonella antibody levels, and echocardiographic findings of endocarditis. Bartonella species are zoonotic, time-dependent, Gram-negative bacteria most often transmitted by arthropod vectors. Cats often serve as reservoirs of the organism. Because of ambiguous clinical manifestations, early recognition is challenging unless there is initial suspicion of a zoonotic etiology. We hope this case emphasizes…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
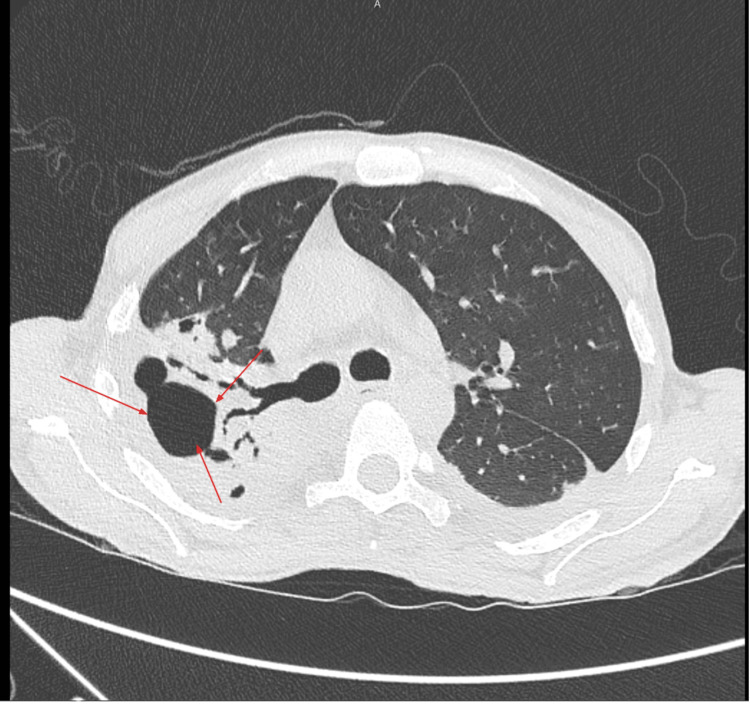 Figure 1
Figure 1| Test | Result | Reference Range |
| WBC | 18.8 K/μL | 4.0-11.0 K/μL |
| Hemoglobin | 6.5 g/dL | 13.5-17.5 g/dL |
| MCV | 57.1 fL | 80-100 fL |
| Platelets | 586 K/μL | 150-400 K/μL |
| Sodium | 130 mmol/L | 135-145 mmol/L |
| CO₂ | 18 mmol/L | 22-28 mmol/L |
| TSH | 29.231 mIU/L | 0.4-4.5 mIU/L |
| Free T4 | 0.64 ng/dL | 0.7-1.9 ng/dL |
| RPR HIV | 1:64, Negative | Non-reactive, non-reactive |
| Location | Finding | Size |
| Right upper lobe | Necrotic abscess | 6.0 x 3.2 x 5.1 cm |
| Right middle lobe | Bronchopleural fistula | Small |
| Left pleural space | Loculated empyema | Multiloculated |
| Modality | Findings |
| TTE | EF 51-55%, poor valve visualization |
| TEE | EF 25-30%, mobile mass on aortic valve, trace AR |
| Test | Result |
| Pleural fluid culture | Streptococcus constellatus |
| BAL culture | MRSA |
| Blood cultures | Negative x multiple |
| Bartonella serology |
|
| Q fever serology | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBartonella species infections research · Infective Endocarditis Diagnosis and Management · Streptococcal Infections and Treatments
Introduction
Infective endocarditis (IE) is a severe infection resulting from inflammation of the endocardial surface, most notably the cardiac valves. Blood culture-negative endocarditis (CNE) occurs in 5-31% of IE cases, frequently due to prior antibiotic use, difficult-to-culture organisms, or atypical zoonotic pathogens [1-3]. *Bartonella *spp. are Gram-negative, facultative intracellular bacteria increasingly recognized as causes of CNE, particularly in patients with pertinent epidemiologic exposures [4]. *Bartonella henselae *is primarily transmitted via domestic cats, while B. quintana is associated with human body lice [5].
Both species can cause subacute or chronic infection, often presenting with nonspecific systemic symptoms, such as malaise, fatigue, low-grade fevers, or weight loss, which can delay diagnosis. Complications may include valvular damage, heart failure, and systemic embolization. Because *Bartonella *spp. are intracellular and slow-growing, standard blood cultures often fail to detect infection, making serologic testing and echocardiography essential [5]. This case highlights an unusual presentation of Bartonella-associated CNE with concurrent necrotizing pneumonia and empyema in an adult male.
Case presentation
A 42-year-old man with a history of asthma presented to the emergency department with worsening dyspnea for the past two weeks, a productive cough with yellow sputum, and intermittent fatigue. He denied fevers, weight loss, or chest pain. He has two pet indoor-outdoor cats, but he denied any recent travel, alcohol use, drug use, homelessness, or incarceration.
On arrival, the patient was tachypneic (RR: 26), tachycardic (HR: 112), and hypoxic (88% on room air, improving to 98% on a 2L nasal cannula). The physical exam revealed decreased breath sounds bilaterally; no murmurs on cardiac exam. Relevant laboratory findings included leukocytosis, microcytic anemia, thrombocytosis, hyponatremia, elevated alkaline phosphatase, and hypothyroidism (Table 1). The patient's initial labs suggested a very low hemoglobin; however, he did not require a transfusion as repeat labs indicated a hemoglobin level of >7 g/dL and the patient did not present with any signs of active bleeding. Serology for syphilis was reactive by rapid plasma reagin (RPR) (1:64). HIV and hepatitis panels were non-reactive.
Contrast-enhanced CT chest/abdomen/pelvis imaging revealed bilateral multifocal consolidations with cavitation in the right upper lobe (6.0 x 3.2 x 5.1 cm) and large necrotic abscesses, which were consistent with necrotizing pneumonia (Figure 1). There was evidence of a right-sided bronchopleural fistula and a large loculated left pleural effusion (Table 2). The procedure to place a left-sided pigtail catheter for drainage was performed by pulmonology; analysis confirmed empyema with neutrophilic predominance, and cultures grew Streptococcus constellatus. Bronchoalveolar lavage grew methicillin-resistant *Staphylococcus aureus *(MRSA).
Axial chest CT shows a large, thick-walled cavitary lesion in the right upper lobe with multiple internal air-fluid levels and surrounding parenchymal consolidation
Wide-spectrum antibiotics, vancomycin, cefepime, and metronidazole, were given, yet inflammatory markers remained elevated. Blood cultures were persistently negative. A transesophageal echocardiogram (TEE) was ordered, and it showed a mobile echodensity on the aortic valve with trace aortic regurgitation and reduced EF (25-30%) (Table 3).
Given the patient’s history of cat exposure and negative cultures, zoonotic testing was pursued. *Bartonella *serologies returned positive: B. henselae IgG 1:512 and *B. quintana *IgG 1:1024. Q fever serologies were negative (Table 4).
Based on the clinical and serologic data, the patient was diagnosed with Bartonella-associated CNE. The patient directed therapy with doxycycline 100 mg BID. Rifampin was avoided due to potential drug-drug interactions with alprazolam, which he was taking for his anxiety. Benzathine penicillin was changed to continuous infusion IV penicillin G due to coexisting latent syphilis. The patient was set to receive a six-week course of antibiotic therapy and follow-up at the outpatient clinic to reassess.
Discussion
This case highlights the diagnostic challenges associated with CNE, particularly when *Bartonella *species are the cause. Although CNE represents a minority of IE cases, *Bartonella *has emerged as a leading etiology when epidemiologic exposures are present [2,3]. Its intracellular biology and atypical growth requirements explain persistently negative blood cultures, which can delay diagnosis and treatment.
*B. henselae *and *B. quintana *are small, intracellular, Gram-negative bacilli with differentiated epidemiologic features. *B. henselae *infection is classically known for being associated with exposure to domestic cats with close contact, such as scratches, bites, and contact with cat fleas, which are vectors of the bacteria. *B. quintana *is classically affiliated with poor hygiene, homelessness, and infestation with the human body louse, many of whom are socioeconomically disadvantaged [4,5]. Both species can cause subacute or chronic infection, including IE that can develop in a subacute manner over several weeks to months [4,5]. *Bartonella *IE is complicated to recognize early because the clinical symptoms often start insidiously with non-specific systemic symptoms of malaise, weight loss, and low-grade fevers.
Diagnosis requires integration of serology, imaging, and molecular methods where available. IgG titers ≥1:800 are strongly predictive of *Bartonella *endocarditis in the appropriate context [6-9]. Polymerase chain reaction (PCR) of blood or excised valve tissue can provide confirmatory evidence, but it is not always available, and sensitivity varies. Next-generation sequencing (NGS) of microbial 16S rDNA is an emerging tool in cases where cultures and serologies are inconclusive, especially in immunocompromised hosts [10]. In this patient, markedly elevated *Bartonella *titers along with TEE-confirmed vegetations supported the diagnosis.
Management requires prolonged antimicrobial therapy. Doxycycline for at least six weeks is standard, often combined with an aminoglycoside or rifampin for synergistic activity [11,12]. Rifampin was contraindicated here due to drug interactions, so doxycycline monotherapy was used. While doxycycline alone is generally considered less desirable, the treatment was administratively acceptable given that the patient was clinically stable and not exhibiting clinical complications related to embolization. The patient was hospitalized for a prolonged period due to necrotizing pneumonia and empyema, for which they required hospitalization, an ideal situation to ensure completing the full course of antibiotics as an inpatient.
Necrotizing pneumonia is an aggressive pulmonary process marked by cavitation, liquefactive necrosis, and parenchymal destruction. It is most commonly linked to highly invasive organisms such as S. aureus, Klebsiella pneumoniae, and members of the *Streptococcus anginosus *group and is typically encountered in patients who are critically ill or immunocompromised [13,14]. When described in the context of endocarditis, necrotizing pneumonia is usually secondary to septic emboli originating from infected valves rather than a concurrent destructive pulmonary infection. The presence of widespread parenchymal necrosis, empyema, and bronchopleural fistula alongside CNE, therefore, represents the intersection of two severe disease processes that rarely occur together.
What makes this case particularly distinct is the coexistence of Bartonella-associated CNE with necrotizing pneumonia in an otherwise healthy host. Although more than one hundred cases of *Bartonella *endocarditis have been published, most involve isolated cardiac disease or patients with well-recognized risk factors, such as homelessness, HIV infection, or other immunosuppressive states [5,7]. To date, *Bartonella *has not been reported in association with necrotizing pneumonia as a parallel process. The combination of destructive lung infection requiring invasive drainage and valve involvement with persistently negative blood cultures broadens the known clinical spectrum of *Bartonella *infection. It also highlights the importance of recognizing that overlapping pulmonary and cardiac manifestations may reflect two distinct but simultaneous infectious pathways, particularly when initial diagnostic testing does not point to a single unifying cause [5,13,14].
Conclusions
*Bartonella *species are important causes of CNE and should remain a key diagnostic consideration in patients with negative blood cultures, unexplained valvular vegetations, and a history of animal exposure, particularly to cats. This case adds to the literature by documenting the rare coexistence of *Bartonella *endocarditis with necrotizing pneumonia, empyema, and a bronchopleural fistula in an adult male - an unusual presentation that broadens the recognized spectrum of *Bartonella *infection. To conclude, this case highlights the need for vigilance in diagnosing culture-negative endocarditis and awareness of the rare complications that may accompany it.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis Clin Infect Dis Li JS Sexton DJ Mick N 6336383020001077072110.1086/313753 · doi ↗ · pubmed ↗
- 2Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases Clin Infect Dis Fournier PE Thuny F Richet H 1311405120102054061910.1086/653675 · doi ↗ · pubmed ↗
- 3Blood culture negative endocarditis: analysis of 63 cases presenting over 25 years Heart Lamas CC Eykyn SJ 2582628920031259182310.1136/heart.89.3.258PMC 1767579 · doi ↗ · pubmed ↗
- 42015 ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM)Eur Heart J Habib G Lancellotti P Antunes MJ 307531283620152632010910.1093/eurheartj/ehv 319 · doi ↗ · pubmed ↗
- 5Bartonella, a common cause of endocarditis: a report on 106 cases and review J Clin Microbiol Edouard S Nabet C Lepidi H Fournier PE Raoult D 8248295320152554039810.1128/JCM.02827-14PMC 4390654 · doi ↗ · pubmed ↗
- 6Diagnostic methods: current best practices and guidelines for identification of difficult-to-culture pathogens in infective endocarditis Cardiol Clin Houpikian P Raoult D 2072172120031287489410.1016/s 0733-8651(03)00028-6 · doi ↗ · pubmed ↗
- 7Bartonella species, an emerging cause of blood-culture-negative endocarditis Clin Microbiol Rev Okaro U Addisu A Casanas B Anderson B 7097463020172849057910.1128/CMR.00013-17PMC 5475225 · doi ↗ · pubmed ↗
- 8Bacillus cereus and related species Clin Microbiol Rev Drobniewski FA 32433861993826939010.1128/cmr.6.4.324PMC 358292 · doi ↗ · pubmed ↗