Intraoperative transesophageal echocardiography under aortic arch branch blood flow monitoring in a patient with an aberrant left subclavian artery: a case report
Yasutaka Suzuki, Takahiro Kawaji, Hidefumi Komura, Satoshi Komatsu, Naohide Kuriyama, Tomoyuki Nakamura

TL;DR
A patient with a rare blood vessel anomaly safely underwent a heart imaging procedure during surgery with proper monitoring.
Contribution
This case demonstrates a safe approach to TEE in patients with an aberrant left subclavian artery using imaging and monitoring.
Findings
TEE was safely performed in a patient with a right-sided aortic arch and ALSA.
Bilateral radial arterial pressures and cerebral oxygen saturation monitoring were effective.
No neurological or upper-limb deficits occurred post-surgery.
Abstract
Transesophageal echocardiography (TEE) is widely used in cardiac and non-cardiac surgeries with major hemodynamic fluctuations. In patients with vascular anomalies near the esophagus, such as an aberrant left subclavian artery (ALSA), TEE may pose a risk of vascular compression. However, no guidelines exist. Case presentation. A 19-year-old woman with biliary atresia underwent living donor liver transplantation. Preoperative imaging showed a right-sided aortic arch with ALSA coursing posterior to the esophagus, and ALSA compression was considered a risk during TEE. Therefore, bilateral radial arterial pressures and regional cerebral oxygen saturation (rSO₂) were monitored. The TEE probe was inserted under videolaryngoscopic guidance without resistance or hemodynamic disturbance, and no arterial waveform attenuation or rSO₂ changes occurred. Transplantation was uneventful, and the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
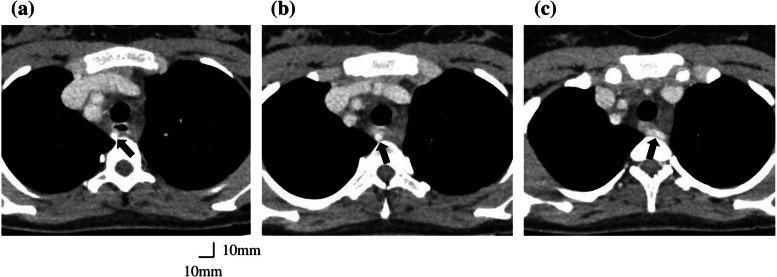 Figure 1
Figure 1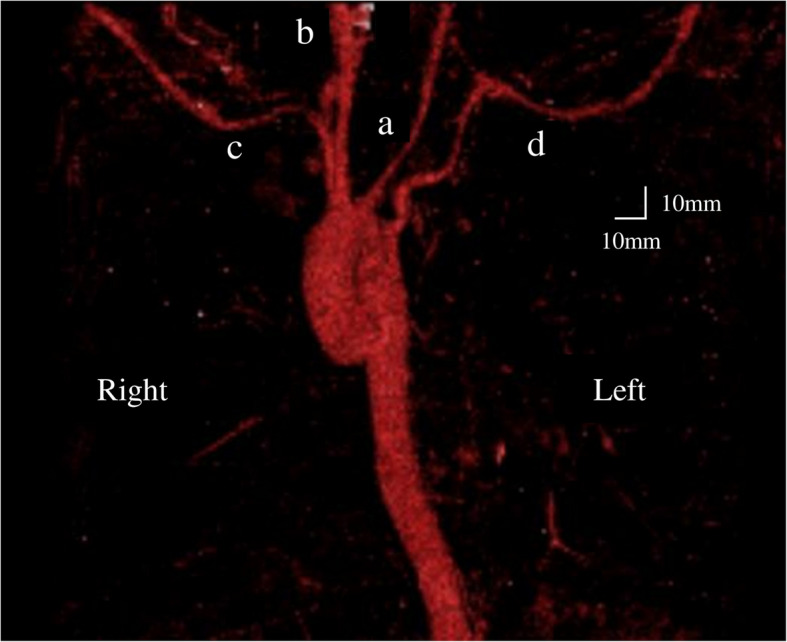 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Cardiac Valve Diseases and Treatments · Congenital Heart Disease Studies
Background
Transesophageal echocardiography (TEE) is a useful tool in cardiac anesthesia, including for risk management of complications and surgical decision-making [1]. TEE is now widely used not only in cardiac surgery but also in non-cardiac surgeries where drastic hemodynamic changes are expected or in cases of unexplained intraoperative hypotension [2]. Although TEE is considered minimally invasive, caution is required as probe insertion and manipulation may cause oropharyngeal, esophageal, or gastric trauma [3]. In particular, in patients with vascular anomalies adjacent to the esophagus, such as an aberrant subclavian artery (ASA), there may be an increased risk of vascular compression or injury [4–11]. However, no guidelines exist regarding preventive strategies. Here, we report a case of a living donor liver transplantation in a patient with an aberrant left subclavian artery (ALSA), in whom perioperative TEE during anesthesia was safely performed under arch branch blood flow monitoring.
Case presentation
A 19-year-old woman (height, 152 cm; weight, 50 kg) with congenital biliary atresia underwent Kasai portoenterostomy shortly after birth. Postoperatively, jaundice was well controlled, and she was regularly followed up. However, in recent years, she developed recurrent cholangitis and progressive cirrhosis, including massive splenomegaly, making it necessary to undergo a living-donor liver transplantation with her older sister as the donor. Preoperative contrast-enhanced CT demonstrated a right-sided aortic arch with a left subclavian artery coursing between the esophagus and vertebral column (Fig. 1). Three-dimensional vascular reconstruction revealed sequential branching of the left common carotid, right common carotid, right subclavian, and left subclavian arteries from the proximal segment of the right-sided aortic arch (Fig. 2). The left common carotid artery was narrower than the right common carotid artery. The left subclavian artery originated from the most distal segment of the right-sided aortic arch and coursed posterior to the esophagus, identifying it as ALSA. The patient had no symptoms of dysphagia. Although the patient had previously undergone endoscopic variceal ligation for esophageal varices, preoperative upper gastrointestinal endoscopy revealed no varices with red color signs and no obvious protruding lesions.Fig. 1. Thoracic contrast-enhanced computed tomography images. (→): Aberrant left subclavian arteryFig. 2Three-dimensional computed tomography with vascular reconstruction. The left common carotid (a), right common carotid (b), right subclavian (c), and left subclavian arteries (d) branched sequentially from the proximal segment of the right-sided aortic arch. The left common carotid artery is narrower than the right common carotid artery. The left subclavian artery arises from the most distal portion of the right sided aortic arch and courses posterior to the esophagus, consistent with an aberrant left subclavian artery
Given the risk of pronounced bleeding—particularly owing to adhesions from prior Kasai portoenterostomy and massive splenomegaly—we planned intraoperative TEE for careful hemodynamic monitoring. Pulmonary artery catheterization and advanced arterial pressure waveform analysis were considered as alternatives, but TEE was selected as it provides direct, real-time anatomic and functional cardiac assessment. However, because the ALSA coursed posterior to the esophagus, we anticipated a risk of vascular compression during TEE probe insertion and manipulation. Therefore, we added bilateral radial arterial pressures and regional cerebral oxygen saturation (rSO2) monitoring to detect compression-related changes. Worrisome attenuation of the left radial waveform or cerebral desaturation during probe insertion would have prompted immediate probe withdrawal and a switch to pulmonary-artery–catheter–based monitoring.
The patient underwent intraoperative monitoring, including electrocardiography, peripheral oxygen saturation, non-invasive blood pressure, processed electroencephalography (EEG) monitoring with SedLine® (Masimo Corp., Irvine, CA, USA), and rSO₂, which was measured using the O3® Regional Oximetry system (Masimo Corp., Irvine, CA, USA). Baseline rSO₂ values were 52% on the right and 59% on the left. General anesthesia was induced with 60 mg of propofol, remifentanil at 0.1 μg/kg/min, fentanyl 100 μg, and rocuronium 50 mg, using a rapid sequence induction and intubation technique. Following tracheal intubation, invasive arterial catheters were placed in both radial arteries, revealing a 15–20 mmHg lower pressure in the left radial artery compared to the right. A triple-lumen central venous catheter for drug administration and a 12-Fr sheath introducer for large-volume fluid infusion were inserted via the right internal jugular vein. The TEE probe (X7-2t transducer; Philips Healthcare, Andover, MA, USA; tip dimensions approximately 17 mm × 13 mm) was inserted under videolaryngoscopic guidance with careful visualization of the esophageal inlet. No resistance was encountered during insertion, and no significant changes were observed in left radial artery pressure or left-sided rSO₂. Blood flow assessment of ALSA was attempted using TEE, but assessment distal to the stenotic site was limited. General anesthesia was maintained with 3.5% desflurane, remifentanil at 0.4 μg/kg/min, and rocuronium at 7 μg/kg/min, along with noradrenaline at 0.05–0.1 μg/kg/min as a vasopressor. Throughout the intraoperative period, TEE manipulation did not cause attenuation or loss of the left radial arterial pulse waveform, nor did it result in significant rSO₂ differences between the right and left sides. In addition, the patient state index, a processed EEG parameter, remained stable at approximately 30. The procedure was prolonged due to adhesion dissection and hepatic artery reanastomosis. However, there were no major complications, including those related to the anhepatic phase or hepatic ischemia–reperfusion injury, and the surgery was successfully completed as planned. The TEE probe was removed postoperatively without blood contamination. The total durations of surgery and anesthesia were 1,362 and 1,217 min, respectively. Estimated blood loss was 5,414 g, and urine output was 2,900 mL. The patient received 4,100 mL of crystalloid, 2,250 mL of 5% albumin, 2,800 mL of packed red blood cells, 6,720 mL of fresh frozen plasma, 150 mL of cryoprecipitate, and 400 mL of platelet concentrate.
Postoperatively, the patient was transferred to the intensive care unit (ICU) under sedation with propofol at 4 mg/kg/h. Upon emergence from anesthesia, she exhibited no neurological deficits or upper limb dysfunction. Her postoperative course was uneventful; she was extubated on postoperative day 4 and discharged from the ICU on postoperative day 8.
Discussion
This case shows that TEE can be performed safely in patients with an aberrant subclavian artery (ASA), despite a potentially increased risk of vascular compression. Preoperative imaging and intraoperative monitoring provided an extra safety net, confirming the absence of compression and ensuring that immediate corrective action would have been possible.
ASA is a congenital vascular anomaly in which the subclavian artery arises abnormally from the aortic arch and passes adjacent to the esophagus, predisposing it to compression by a TEE probe. Eight previous reports (five pediatric, three adult) described ASA compression during TEE, all showing loss of ipsilateral radial arterial waveform that resolved after probe withdrawal [4–11] (Table 1). The narrower esophagus in infants presumably increased their risk of compression. Of the five pediatric cases, four involved ARSA—including two with Down syndrome (trisomy 21)—and one involved ALSA with a right-sided aortic arch. Among the three adult cases, two involved ARSA and one ALSA associated with a right-sided aortic arch. ARSA is frequently associated with Down syndrome, particularly in patients with congenital heart disease [12], while ALSA is typically linked to a right-sided aortic arch and is rarer [13]. ASA was identified preoperatively in four of the five pediatric cases but in only one of the three adult cases (Table 1), suggesting underrecognition in adult non-cardiac surgery. Table 1. Review of the literature on aberrant subclavian artery (ASA) compression during transesophageal echocardiography (TEE)Author/year Reference NoAgeComorbiditiesSurgical procedureTypes of ASAMonitoringDiagnosis of ASA compressionTEE probe maneuverBensky AS/1995 [4]5 monthsDown syndromeAVSD repairARSARight radial arterial pressureWaveform dampened,, recovered after TEE withdrawalConfirmed by normal ascending aortic pressureContinuedKoinig H/2003 [5]7 weeksDown syndromeAVSD repairARSARight radial arterial pressureContralateral NIBP and pulse oximetryWaveform loss, recovered after TEE withdrawalContralateral normalRemovalPark SY/2010 [6]75 yearsCoronary artery diseaseOff-pump coronary artery bypass graftARSARight radial arterial pressureRight femoral arterial pressureWaveform loss, recovered after TEE withdrawalFemoral normalChanged to smaller probeSierra RL/2011 [7]62 yearsHepatocellular carcinomaHepatectomyARSARight radial arterial pressure and pulse oximetryContralateral NIBP and pulse oximetryWaveform loss, recovered after TEE withdrawalContralateral normalRemovalGarg V/2012 [8]8 monthsVSD tricuspid regurgitationVSD repairARSARight radial arterial pressureContralateral (leg) NIBP and pulse oximetryWaveform loss, recovered after TEE withdrawalContralateral (leg) normalRemovalLee WI/2013 [9]1 yearsTOFTOF toal corrective surgeryALSALeft radial arterial pressureFemoral arterial pressure and contralateral pulse oximetryWaveform loss, recovered after TEE withdrawalFemoral and contralateral normalRemovalHattori K/2016 [10]6 monthsAVSDVSD closureARSARight radial arterial pressureContralateral pulse oximetryWaveform loss, recovered after TEE withdrawalContralateral normalChanged to smaller probeApatov DA/2020 [11]54 yearsAortic stenosis History of CoAAortic Valve ReplacementARSARight and left radial arterial pressureContralateral NIBPWaveform loss, recovered after TEE withdrawalContralateral normalContinuedAVSD Atrioventricular Septal Defect, ARSA Aberrant Right Subclavian Artery, NIBP Non-Invasive Blood Pressure, VSD Ventricular Septal Defect, TOF Tetralogy of Fallot, ALSA Aberrant Left Subclavian Artery, CoA Coarctation of the Aorta
In our case, preoperative contrast-enhanced CT revealed ALSA and narrowing of the left carotid artery. Because the circle of Willis provides only limited collateral flow [14], ischemia of the left arm and left cerebral hemisphere was a concern. Bilateral radial arterial pressures and regional cerebral oxygen saturation (rSO₂) were continuously monitored during TEE probe insertion. Although rSO₂ is less sensitive for vertebrobasilar ischemia [15], it is clinically useful for detecting cerebral hypoperfusion [16]. As an alternative, transcranial Doppler could be considered for evaluating vertebral artery blood flow; however, its continuous intraoperative use was deemed impractical. Therefore, rSO₂ was selected in the present case. To our knowledge, rSO₂ monitoring has not previously been reported in TEE-related ASA compression, and its potential value, demonstrated by the present study, warrants further investigation.
The 2010 ESC guidelines recommend preoperative imaging in patients with aortic or esophageal disease, but offer no specific intraoperative monitoring strategies [1]. Furthermore, growing evidence supports the safety and utility of TEE in liver transplantation anesthesia [17–20]. In these various settings, targeted monitoring of arch branch perfusion—as performed in the current study—may help detect otherwise unrecognized ASA compression and guide timely probe adjustment or removal.
As TEE use expands in non-cardiac surgery, the potential for unrecognized ASA compression increases, underscoring the importance of preoperative vascular assessment. While ASA may pose a risk during TEE, our case suggests that with appropriate imaging and monitoring, TEE can be used safely even in patients with arch anomalies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee WI, Kim DH, Chae YJ, et al. Compression of the left subclavian artery caused by a transesophageal echocardiography probe in an infant with a right-sided aortic arch: a case report. Anesth Pain Med. 2013;8:196–198. https://www.anesth-pain-med.org/upload/pdf/Apm 008-03-11.pdf.