Sugar-sweetened beverages and the risk of hyperuricemia and gout: a meta-analysis
Yuejie Lu, Yinuo Wang, Renjie Huang, Hejing Pan, Zhijun Xie, Chengping Wen, Lin Huang, Xuanlin Li

TL;DR
Drinking sugary beverages increases the risk of high uric acid and gout, especially in men.
Contribution
This study provides a comprehensive meta-analysis on the link between sugar-sweetened beverages and gout/hyperuricemia.
Findings
SSB intake significantly increases the risk of hyperuricemia and gout.
Fructose consumption is strongly linked to higher gout risk.
Males show higher risk increases from SSB and fruit juice than females.
Abstract
This meta-analysis aimed to investigate the association between sugar-sweetened beverages (SSBs), fructose, and the risk of gout and hyperuricemia. Following PRISMA guidelines, we systematically searched PubMed, EMBASE, and Cochrane Library for observational studies from inception to March 2025. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were pooled using random/fixed-effects models. Subgroup analyses explored sex. Heterogeneity (I2) and publication bias were assessed. A total of 22 studies (235,790 participants) were included. SSB intake significantly increased the risk of hyperuricemia (OR = 1.33, 95% CI: 1.23–1.44) and gout (OR = 1.21; 95% CI 1.11–1.32). Fruit juice (FJ) showed a modest association with hyperuricemia (OR = 1.15, 95% CI: 1.02–1.29) and an increased risk of gout (OR = 1.28; 95% CI 0.96–1.72). Fructose consumption was strongly associated with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
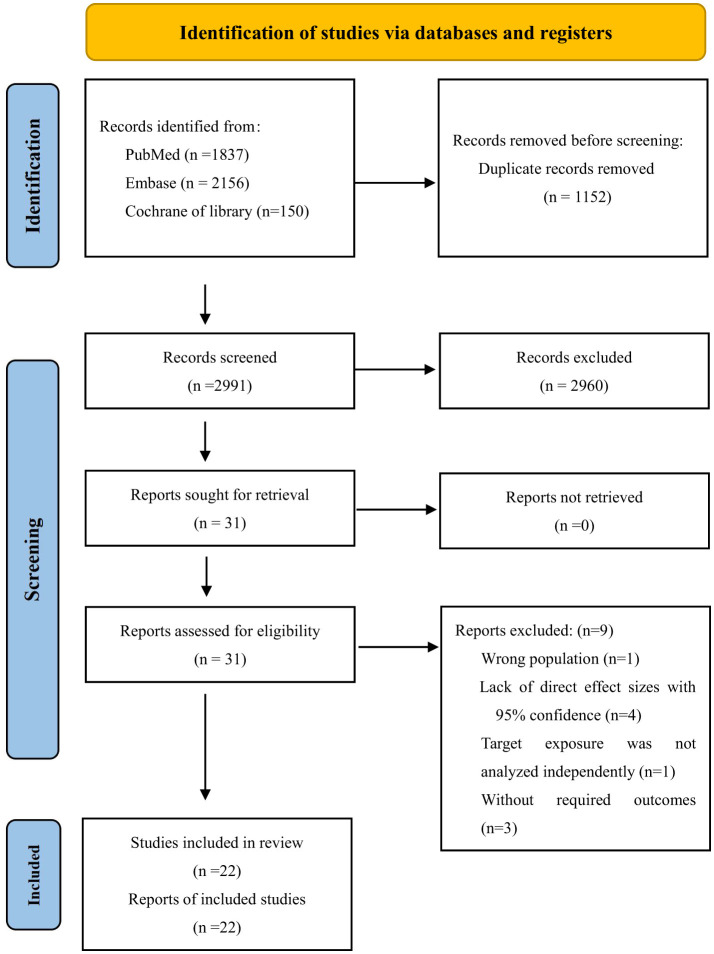 Figure 1
Figure 1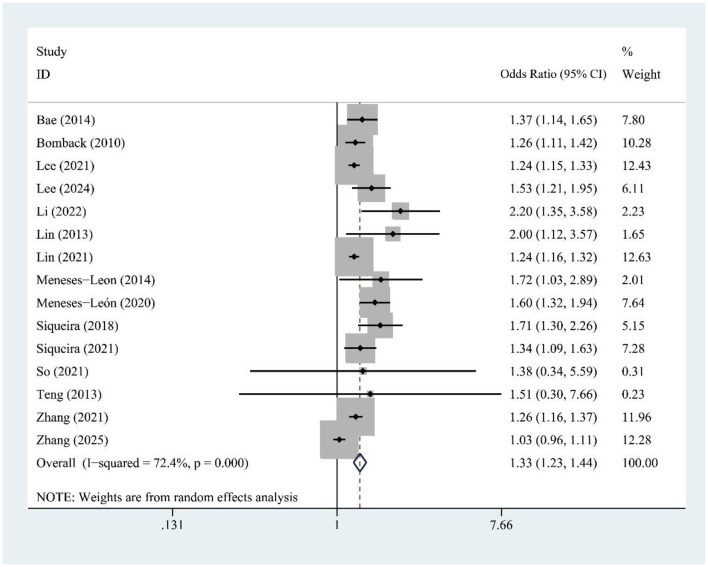 Figure 2
Figure 2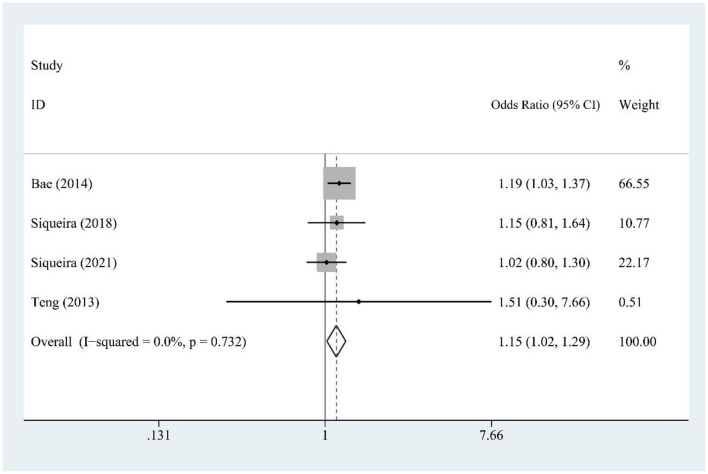 Figure 3
Figure 3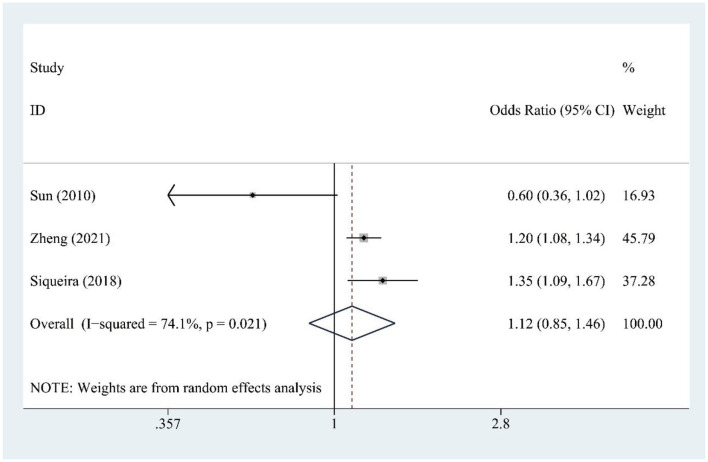 Figure 4
Figure 4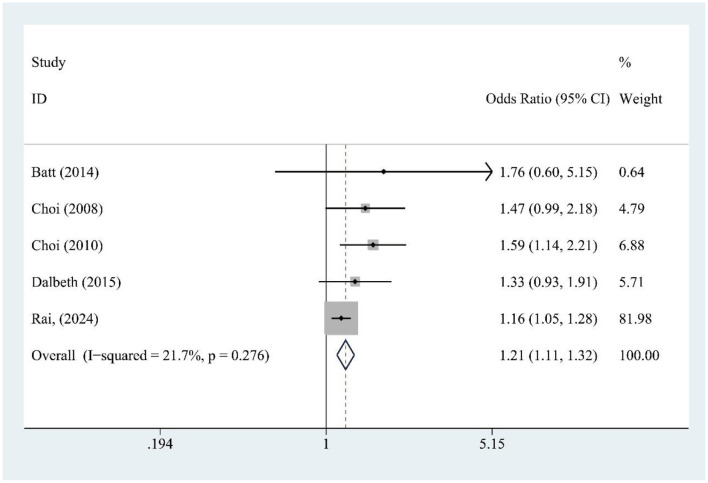 Figure 5
Figure 5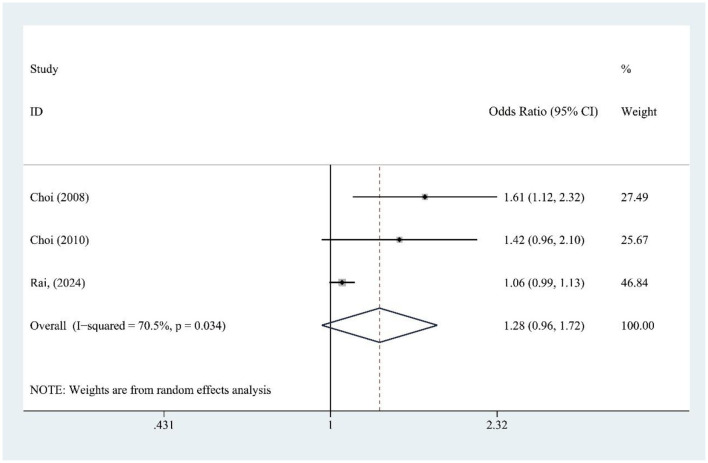 Figure 6
Figure 6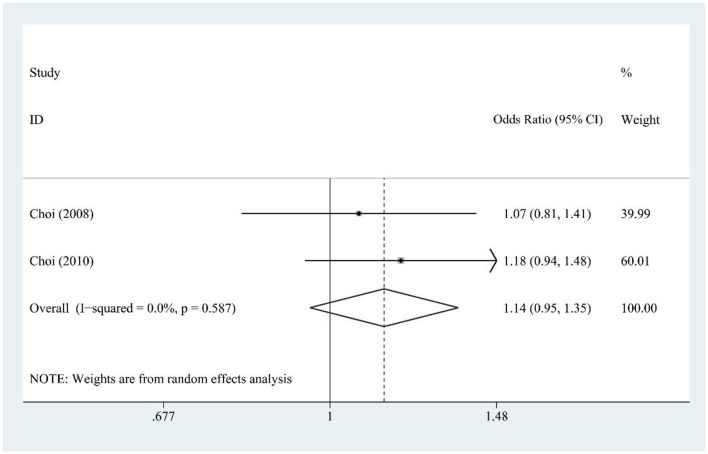 Figure 7
Figure 7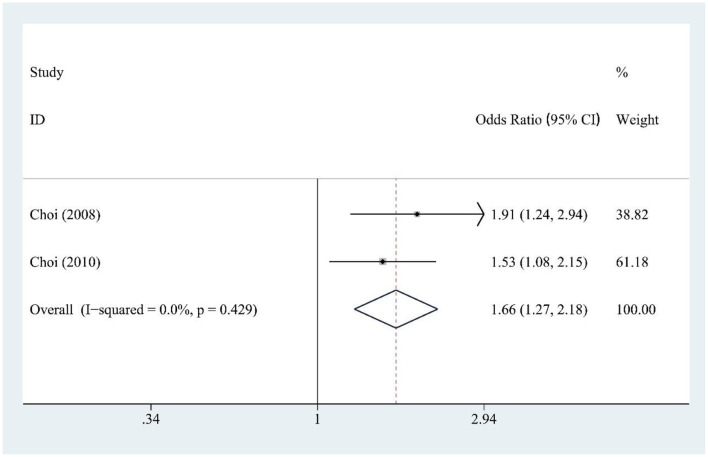 Figure 8
Figure 8|
|
|
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| Choi et al. | 2008 | USA | 40–75 | M | 46,393 | Cohort study | SSB DSD FJ | FFQ | Gout | ACR criteria | 12 |
| Choi et al. | 2010 | USA | 30–55 | F | 78,906 | Cohort study | SSB DSD FJ | FFQ | Gout | ACR criteria | 22 |
| Bomback et al. | 2010 | USA | 45–64 | M/F | 9,451 | Cohort study | SSB | FFQ | Hyperuricemia | NR | 3 |
| Meneses-León et al. | 2020 | Mexico | 18–85 (45.8 ± 12.9) | M/F | 1,300 F: 978 M: 322 | Cohort study | SSB, DSD | FFQ | Hyperuricemia | The uricase colorimetric method | 14 |
| Siqueira et al. | 2021 | Brazil Mexico | 35–74 (51.3 ± 8.9) | M/F | 10,072 M: 4,151 F: 5,921 | Cohort study | SSB FJ | FFQ | Hyperuricemia | The uricase colorimetric method | 4 |
| Rai et al. | 2024 | USA | M: 53.8 ± 9.8 F: 50.9 ± 7.2 | M/F | 122,679 M: 43,703 F: 78,976 | Cohort study | SSB FJ | FFQ | Gout | ACR criteria | 26 |
| Zhang et al. | 2025 | China | 22–87 (48.48 ± 11.82) | M/F | 10,883 M: 6,449 F: 4,434 | Cohort study | SSB | Simple Question | Hyperuricemia | Laboratory | 2 |
|
| |||||||||||
| Batt et al. | 2014 | New Zealand European Caucasian | 57.9 (17–94) Case: 63.8 (23–94) Control: 44.4 (17–79) | M/F | 592 Case: 412 Control: 18 | Case-control study | SSB | Simple Question | Gout | Self reported Physician diagnosed | / |
| New Zealand (Maori) | 47.1 (17–81) Case: 54.2 (23–81) Control: 42.7 (17–80) | 502 Case: 190 Control: 312 | |||||||||
| New Zealand (Pacific Islander) | 44.6 (17–86) Case: 47.7 (18–81) Control: 39.9 (17–6) | 540 Case: 323 Control: 217 | |||||||||
| Atherosclerosis Risk In Communities | 53.8 (44–5) Case: 4.5 (45–5) Control: 3.8(44–5) | 7,075 Case: 148 Control: 6,927 | |||||||||
|
| |||||||||||
| Dalbeth et al. | 2015 | New Zealand | 49.5 | M/F | 2,578 | Cross-sectional study | SSB | Self-reported | Gout | Clinically ascertained by ARA | / |
| Bomback et al. | 2010 | USA | 45–64 | M/F | 15,745 | Cross-sectional study | SSB | FFQ | Hyperuricemia | NR | / |
| Teng et al. | 2013 | Singapore | 45–74 (57.6 ± 7.9) | M/F | 483 | Cross-sectional study | SSB | FFQ | Hyperuricemia | Direct enzymatic assay | / |
| Bae et al. | 2014 | Korea | M: 62.5 ± 9.6 F: 61.6 ± 9.8 | M/F | 9,400 M: 3,564 F: 5,836 | Cross-sectional study | SSB | FFQ | Hyperuricemia | Laboratory | / |
| Meneses-Leon et al. | 2014 | Mexico | 18–70 M: 42.6 ± 11.6 F: 43.0 ± 12.2 | M/F | 6,705 M: 1,956 F: 4,749 | Cross-sectional study | SSB | FFQ | Hyperuricemia | Enzymatic Colorimetric method | / |
| Li et al. | 2022 | China | 42.7 ± 14.2 | M | 620 | Cross-sectional study | SSB | FFQ | Hyperuricemia | Laboratory | / |
| Lin et al. | 2013 | China | 12–16 | M/F | 2,727 | Cross-sectional study | SSB | FFQ | Hyperuricemia | Modified hexokinase enzymatic method | / |
| Lee et al. | 2024 | Korean | 19–64 | M/F | 2,881 M: 1,066, F: 1,815 | Cross-sectional Study | SSB | FFQ | Hyperuricemia | The uricase colorimetric method | / |
| Siqueira et al. | 2018 | Brazil Mexico | 35–74 50 ± 8.4 | M/F | 7,173 M: 3,325, F: 3,848 | Cross-sectional study | SSB FJ | FFQ | Hyperuricemia | The uricase colorimetric method | / |
| Lee et al. | 2021 | Korea | 53.1 ± 8.3 | M/F | 167,752 | Cross-sectional study | SSB | Simple question | Hyperuricemia | NR | / |
| Zhang et al. | 2020 | China | >18 | M | 25,507 M: 13,013 F: 12,494 | Cross-sectional study | SSB | FFQ | Hyperuricemia | Enzymatic colorimetric test | / |
| Lin et al. | 2021 | USA | ≥18 | M | 15,338 M: 7,580 F: 7,758 | Cross-sectional study | SSB | 24-h dietary recall | Hyperuricemia | NR | / |
| So et al. | 2020 | Korea | 47 ± 16.4 | M | 10,175 M: 4,300 F: 5,875 | Cross-sectional Study | SSB | 24-h dietary recall | Hyperuricemia | NR | / |
|
| |||||||||||
| Choi et al. | 2008 | USA | 40–75 | M | 755 | Cohort study | Fructose | FFQ | Gout | ACR criteria | 12 |
| Choi et al. | 2010 | USA | 30–55 | F | 78,906 | Cohort study | Fructose | FFQ | Gout | ACR criteria | 22 |
|
| |||||||||||
| Sun et al. | 2010 | USA | 20–80 | M/F | 9,384 | Cross-sectional study | Fructose | 24-h dietary recall | Hyperuricemia | The uricase colorimetric method | / |
| Siqueira et al. | 2018 | Brazil Mexico | 35–74 | M/F | 7,173 M: 3,325 F: 3,848 | Cross-sectional study | Fructose | FFQ | Hyperuricemia | The uricase colorimetric method | / |
| Zheng et al. | 2021 | USA | 21–91 | M/F | 4,576 | Cross-sectional study | Fructose | FFQ | Hyperuricemia | The uricase colorimetric method | / |
|
|
|
|
| |
|---|---|---|---|---|
|
| ||||
|
| ||||
| Female | 8 | 1.29 (1.10–1.50) | 37.2 | 0.132 |
| Male | 8 | 1.37 (1.16–1.63) | 80.1 | 0.000 |
|
| ||||
| Female | 3 | 1.13 (0.95–1.35) | 13.4 | 0.315 |
| Male | 3 | 1.15 (0.97–1.38) | 0.0 | 0.721 |
- —National Natural Science Foundation of China10.13039/501100001809
- —National Key Research and Development Program of China10.13039/501100012166
- —Key Research and Development Program of Zhejiang Province10.13039/100022963
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGout, Hyperuricemia, Uric Acid · Alcohol Consumption and Health Effects · Diet, Metabolism, and Disease
1 Introduction
Gout is a metabolic disorder characterized by hyperuricemia which is defined as a serum urate level exceeding 7.0 mg/dl in men and 5.7 mg/dl in women (1). This condition leads to the formation of monosodium urate crystals, resulting in painful recurrent flares and tissue damage (2–4). The prevalence of gout varies globally, ranging from < 1 to 6.8%, with an incidence of 0.58−2.89 cases per 1,000 person-years (5). In addition to its acute symptoms, gout and hyperuricemia are strongly associated with a range of comorbidities, including hypertension, diabetes mellitus, metabolic syndrome, and cardiovascular diseases (6). Whilst gout can be eradicated with urate-lowering therapy and reduce the risk of recurrence by controlled diet, treatment options remain suboptimal (7, 8). Various factors contribute to the development of gout, including comorbidities, genetic pre-disposition, obesity, environmental influences, and dietary habits (6, 7, 9). Among these, diet plays a critical role in the onset and progression of the disease. Excessive consumption of sugar, particularly fructose, places an additional strain on the kidneys and has been linked to the development of chronic kidney disease, which in turn increases the risk of gout and hyperuricemia (10).
Sugar-sweetened beverages (SSBs) are a major source of added sugars in the diet (11). From 1990 to 2018, the global consumption of SSBs among children and adolescents increased by 23% (12), and a model estimated that 184,000 deaths/year worldwide attributable to SSB consumption (13). There is compelling evidence that the consumption of SSBs is directly associated with the risk of cardiovascular disease, cancer, neurological disorders, ectopic fat accumulation, and endocrine/metabolic outcomes (14, 15).
SSB consumption is increasingly recognized to increase the risk of gout and hyperuricemia. A meta-analysis of prospective studies noted an adverse association between SSB and juice intake and incident gout. However, the scope of the analysis was limited to a smaller number of studies (16). Another meta-analysis established a significant positive association between SSB intake and the risk of gout and hyperuricemia, though its inclusion of literature remains constrained (17). To address these limitations, we therefore performed the updated meta-analysis additional study with a new collection of 11 newly published studies after 2017, aimed to overcomes the challenges of small study inclusion, thereby enhancing the reliability and comprehensiveness of the findings, and to fill the gap in quantitative evidence regarding the impact of SSBs and dietary fructose as modifiable risk factors for hyperuricemia and gout.
2 Method
The meta-analysis followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (18). The protocol was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the approval number CRD420251040227.
2.1 Data sources
A comprehensive search of PubMed, EMBASE, and the Cochrane Library databases was conducted up to March 7, 2025. The search was performed by two independent investigators using both Medical Subject Headings (MeSH) and keywords. The terms included “Sugar-Sweetened Beverages,” “Artificially Sweetened Beverages,” “Fructose,” “Gout,” and related outcomes such as “Hyperuricemia” and “Uric Acid.” Search details are provided in Supplementary Tables S1–S3.
2.2 Eligibility criteria
We included observational studies that were (1) case-control, cohort, or cross-sectional in design, and (2) investigated the relationship between sugar-sweetened beverages (SSBs) or fructose and the risk of gout or hyperuricemia.
Studies were excluded if they did not report relative risks (RRs), hazard ratios (HRs), or odds ratios (ORs) with corresponding 95% confidence intervals (CIs), as well as reviews, conference abstracts, case reports, editor letters, duplicate publications, and studies without relevant outcomes.
2.3 Study selection
Two reviewers (YN Wang and YJ Lu) independently screened the titles and abstracts of articles, excluding duplicates and irrelevant studies. Full texts of potentially eligible studies were retrieved and assessed for eligibility. Disagreements were resolved by a third reviewer (XL Li).
2.4 Data extraction
Data extraction was performed independently by the two aforementioned reviewers (YN Wang and YJ Lu), following systematic review guidelines (19). Pre-designed forms were used to extract data on the first author, year of publication, country, age, sex, sample size, study type, exposure and outcome assessments, and follow-up duration. Any discrepancies were resolved through discussion with XL Li.
2.5 Risk of bias
The Agency for Healthcare Research and Quality (AHRQ) checklist (https://www.ncbi.nlm.nih.gov/books/NBK35156/) was used to assess the quality of cross-sectional studies, categorizing them as low (< 4 “yes” responses), medium (4–6 “yes” responses), or high (>7 “yes” responses).
For longitudinal studies, the Newcastle-Ottawa Scale (NOS; http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) was used, with studies classified as low (0–3), moderate (4–6), or high (7–9) quality based on their star ratings.
2.6 Statistical analysis
We extracted adjusted ORs, RRs, HRs, and 95% CIs to evaluate the associations between exposures and outcomes. Given design heterogeneity, we treated HR/RR as relative risk proxies and OR as a prevalence ratio under low-prevalence assumptions (20, 21). Heterogeneity was assessed using Cochran' χ^2^ test (P < 0.1) and I^2^ statistic (I^2^ > 50% indicating substantial heterogeneity). For low heterogeneity (P ≥ 0.1, I^2^ ≤ 50%), fixed-effects models (Mantel–Haenszel) were used, while random-effects models (DerSimonian–Laird) were applied for moderate/high heterogeneity. Sensitivity analyses excluded studies based on design to test robustness, and subgroup analyses were performed by sex and design to explore heterogeneity. Publication bias was evaluated using funnel plot inspection and Egger's regression (P < 0.05). Statistical analyses were conducted using Stata 14.0 (Stata Corp, TX, USA).
3 Result
3.1 Study selection
Our search strategy identified 4,143 articles. After removing 1,152 duplicates, 2,991 abstracts were reviewed in detail. Of these, 2,960 were excluded based on title and abstract screening. Among the remaining 31 studies, nine were further excluded for the following reasons: one study reported an incorrect population, four lacked effect values or CIs, one did not analyze the target exposure independently, and three did not meet the eligibility criteria. Ultimately, 22 studies were included in the systematic review (22–43). A flowchart of the selection process is shown in Figure 1. Excluded studies and their reasons are listed in Supplementary Table S4.
PRISMA flowchart of study selection.
3.2 Study characteristics
This meta-analysis included 22 studies, with a total of 235,790 participants, published up to January 12, 2025. The studies were diverse: 14 cross-sectional, seven prospective cohort, and one case-control. Most assessed SSB and fructose intake using validated FFQs, while some relied on 24-h recalls or self-reported questionnaires. Diagnostic criteria for hyperuricemia and gout were well-defined across most studies. Follow-up durations ranged from 2 to 22 years. Key confounders adjusted for included age, sex, BMI, energy intake, alcohol, hypertension, diabetes, and dietary factors. The studies represented a global population, with participants from Asia (China, South Korea, and Singapore), North America (USA, Mexico), South America (Brazil), and Oceania (New Zealand). Key study characteristics are summarized in Table 1.
3.3 Quality assessment
Cross-sectional studies had an average AHRQ score of 7.81/11 (Supplementary Table S5), and longitudinal studies scored 7.63/9 on the NOS, indicating overall good quality (Supplementary Table S6).
3.4 SSB and hyperuricemia risk
The meta-analysis of 15 studies found a significant association between SSB consumption and increased hyperuricemia risk [OR = 1.33, 95% CI (1.23, 1.44), I^2^ = 72.4%, P = 0.000] (Figure 2). Despite high heterogeneity, sensitivity analysis confirms result stability (Supplementary Figure S1).
Forest plot of the association between sugar-sweetened beverage (SSB) consumption and hyperuricemia risk.
3.5 FJ and hyperuricemia risk
Fruit juice (FJ) intake (four studies) was modestly associated with hyperuricemia risk [OR = 1.15, 95% CI (1.02, 1.29), I^2^ = 0.0%, P = 0.732] (Figure 3).
Forest plot of the association between fruit juice (FJ) consumption and hyperuricemia risk.
3.6 Fructose and hyperuricemia risk
Fructose consumption (three studies) was not significantly associated with hyperuricemia risk [OR = 1.12, 95% CI (0.93, 1.85), I^2^ = 74.1%, P = 0.021] (Figure 4). Moderate heterogeneity indicates some variability. Sensitivity testing showed no substantial changes in the findings (Supplementary Figure S2).
Forest plot of the association between fructose consumption and hyperuricemia risk.
3.7 SSB and gout risk
SSB consumption (five studies) was significantly associated with increased gout risk [OR = 1.21, 95% CI (1.11, 1.32), I^2^ = 21.7%, P = 0.276] (Figure 5), with low heterogeneity supporting consistent findings.
Forest plot of the association between sugar-sweetened beverage (SSB) consumption and gout risk.
3.8 FJ and gout risk
FJ intake (three studies) was not significantly associated with gout risk [OR = 1.28, 95% CI (0.96, 1.72), I^2^ = 70.5%, P = 0.034] (Figure 6), though high heterogeneity suggests variability among studies. Sensitivity analysis confirms result stability (Supplementary Figure S3).
Forest plot of the association between fruit juice (FJ) consumption and gout risk.
3.9 DSD and gout risk
DSD consumption (two studies) showed no significant association with gout risk [OR = 1.14, 95% CI (0.95, 1.35), I^2^ = 0.0%, P = 0.587] (Figure 7), with no heterogeneity indicating reliable findings.
Forest plot of the association between diet soft drink (DSD) consumption and gout risk.
3.10 Fructose and gout risk
Fructose intake (two studies) was significantly associated with increased gout risk [OR = 1.66, 95% CI (1.27, 2.18), I^2^ = 0.0%, P = 0.429] (Figure 8), showing a strong and consistent effect across studies.
Forest plot of the association between fructose consumption and gout risk.
3.11 Subgroup analysis
Among females (eight studies), SSB intake was significantly associated with higher hyperuricemia risk [OR = 1.29, 95% CI (1.10, 1.50), I^2^ = 37.2%, P = 0.132] (Table 2). Males (eight studies) showed a stronger association [OR = 1.37, 95% CI (1.16, 1.63), I^2^ = 80.1%, P = 0.000] (Table 2).
For FJ, no significant association with hyperuricemia risk was found in either females (three studies) [OR = 1.13, 95% CI (0.95, 1.35), I^2^ = 13.4%, P = 0.315] or males (three studies) [OR = 1.15, 95% CI (0.97, 1.38), I^2^ = 0.0%, P = 0.721] (Table 2).
3.12 Publication bias
For SSB and hyperuricemia, Begg's test showed no significant bias (P = 0.181), but Egger's test suggested small-study effects (P = 0.012; Supplementary Figure S4A). No bias was detected for FJ (P = 1.000, P = 0.243) or fructose (P = 1.000, P = 0.279; Supplementary Figures S4B, C). Publication bias for SSB and gout was inconclusive, with marginal significance for bias in Egger's test (P = 0.047; Supplementary Figure S5A). No significant bias was found for FJ and gout (Supplementary Figure S5B), and DSD and gout (Supplementary Figure S5C). Fructose and gout analysis was inconclusive due to the small sample size (Supplementary Figure S5D).
4 Discussion
4.1 Main findings
The findings of this meta-analysis of 235,790 participants suggest that SSB consumption is at significantly increased risks of hyperuricemia and gout, and the risk is higher in males than in females. The findings also emphasize the need for early intervention and continuous monitoring of people with large SSB consumption.
4.2 Comparison with previous meta-analyses
In recent years, increasing numbers of observational studies have reported the increased risk of hyperuricemia and gout in people with SSB consumption. Previous meta-analysis (16), based on three studies, concluded that a history of SSB consumption was associated with a 1.77 (1.20–2.61; I^2^ = 0.0%) times increased risk of incident gout, and FJ consumption was associated with a 2.08 (1.40–3.08; I^2^ = 0.0%) times increased risk of incident gout. However, the number of studies included in this study was too small and did not explore the association between SSBs and hyperuricemia. Another meta-analysis (17) based on nine studies, showed SSB consumption was associated with a 1.35 (1.18–1.55, I^2^ = 40.1%) times increased risk of incident gout, a 1.33 (1.06–1.66, I^2^ = 0.0%) times increased risk of prevalent gout, and a 1.35 (1.19–1.52, I^2^ = 41.4%) times increased risk of hyperuricemia. But this study did not analyze SSBs separately from FJ. In this meta-analysis, we found that consumption of SSBs was associated with a 1.33-fold increased risk of hyperuricemia and a 1.21-fold increased risk of gout. Consumption of FJ was linked to a 1.15-fold increased risk of hyperuricemia and a 1.28-fold increased risk of gout. Additionally, we analyzed that fructose consumption was associated with a 1.12-fold increased risk of hyperuricemia and a 1.66-fold increased risk of gout. Also, DSD consumption was found to have a 1.14-fold increased risk of gout. The subgroup analysis indicated that the risk of SSBs and FJ for hyperuricemia was higher in male.
This study had several advantages over previous meta-analysis. Firstly, our study incorporated the most recent and most comprehensive data to obtain a more complete understanding of the associations. Secondly, we examined the risk of developing hyperuricemia and gout for SSBs, FJ, fructose, and DSD consumption separately, with subgroup analyses by gender.
4.3 Potential underlying mechanisms
SSB-associated hyperuricemia and gout risks arise through interconnected metabolic pathways. Glucose from SSBs fuels purine synthesis via the pentose phosphate pathway, increasing phosphoribosyl pyrophosphate availability for nucleotide formation (44). Excessive glucose intake—a cardinal manifestation of nutrient surplus—activates mTOR/HIF-1α signaling. This dual activation drives anabolic shifts and oxidative stress, while simultaneously inducing insulin resistance. Collectively, these perturbations culminate in proximal tubule dysfunction, thereby impairing renal urate excretion (45–47).
Fructose uniquely drives hyperuricemia through direct hepatic metabolism. Its phosphorylation by fructokinase generates fructose-1-phosphate (F1P), depleting adenosine triphosphate (ATP) and inorganic phosphate (Pi). This impairs adenosine diphosphate (ADP) phosphorylation, trapping F1P while adenylate kinase converts accumulating ADP to adenosine monophosphate (AMP)—a direct uric acid precursor. Concurrently, ATP/Pi depletion attenuates feedback inhibition of urate production, amplifying hyperuricemia (33, 48). While chronic intake downregulates urate excretion transporters thereby reducing uric acid excretion (49). Emerging evidence implicates fructose-mediated gut microbiota alterations in gout pathogenesis (50), suggesting novel therapeutic targets. These mechanisms underscore the importance of SSB reduction in metabolic disorder prevention strategies.
Women have a higher rate of urate excretion and a lower rate of post-secretory reabsorption of renal tubular urate compared to men (51), which may be due to the effect of estrogen (52). This evidence is consistent with the results of our subgroup analysis.
4.4 Clinical recommendations
SSB intake is associated with a higher risk of hyperuricemia and gout, especially in males. Clinically, it is common to routinely inquire about the intake history of SSBs in patients with obesity, hypertension, and chronic kidney disease. In combination with the WHO and WCRF/AICR recommendations and our findings, we recommend reducing the consumption of free sugars or added sugars to below 25 g/day and limiting the consumption of sugar sweetened beverages to less than one serving a week (approximately 200–355 ml/week). Nevertheless, adherence to this precise threshold may be impractical across diverse socioeconomic and cultural contexts. A more feasible public health objective is to prioritize reduction in SSB consumption overall, as any decrease confers benefit. Achieving this requires complementary policy interventions—such as SSB taxation, marketing restrictions, improved nutrition labeling, and enhanced access to healthier beverages—to enable sustained population-level behavior change. To change sugar consumption patterns, especially for children and adolescents, a combination of widespread public health education and policies worldwide is urgently needed (14). In particular, male patients should be more strictly restricted from consuming SSBs due to a higher risk associated with gender differences.
4.5 Strengths and limitations
This meta-analysis robustly links SSB intake to hyperuricemia and gout risks across diverse populations (n = 235,790), with methodological strengths including PRISMA adherence, sensitivity analyses, and high-quality study inclusion. Limitations encompass: (1) causal inference constraints from 14 cross-sectional studies (of 22) due to potential reverse causality (e.g., post-diagnosis SSB reduction); (2) elevated heterogeneity likely attributable to variations in study design, exposure/outcome assessment, intake units, recall bias, diet/lifestyle factors, residual confounders, dietary patterns, and diagnostic criteria, potentially affecting results despite robust sensitivity analyses; (3) limited statistical power for DSD/fructose analyses, along with feasibility challenges in defining heterogeneous beverage categories, such as distinguishing between natural and added-sugar juices or artificial and non-caloric sweeteners, due to the necessitated reliance on prior classifications that may confound outcomes; and (4) geographic bias toward predominantly Asia and North America, non-uniform SSB assessment methods, and unspecified serum urate assays in some studies, all of which potentially contribute to publication bias. Evidence quality is anticipated to improve with future updates, more high-quality studies, broader geographic data, and standardized measurements.
5 Conclusions
SSB intake is associated with a higher risk of hyperuricemia, especially in males, and a modest increase in the risk of gout. FJ intake posed a slight risk for hyperuricemia and gout. Fructose intake was not significantly associated with hyperuricemia risk but significantly associated with gout risk. DSD intake posed a slight risk for gout. The results highlight the need to reduce and continuous monitor SSB intake, especially in high-risk populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen-Xu M Yokose C Rai SK Pillinger MH Choi HK. Contemporary prevalence of gout and hyperuricemia in the United States and decadal trends: the National Health and Nutrition Examination Survey, 2007-2016. Arthritis Rheumatol. (2019) 71:991–9. 10.1002/art.4080730618180 PMC 6536335 · doi ↗ · pubmed ↗
- 2Fitz Gerald JD. Gout. Ann Intern Med. (2025) 178:ITC 33–48. 10.7326/ANNALS-24-0395140063960 · doi ↗ · pubmed ↗
- 3Pillinger MH Mandell BF. Therapeutic approaches in the treatment of gout. Semin Arthritis Rheum. (2020) 50:S 24–30. 10.1016/j.semarthrit.2020.04.01032620199 · doi ↗ · pubmed ↗
- 4Latest guidance on the management of gout. BMJ. (2018) 362:k 2893. 10.1136/bmj.k 289330021789 · doi ↗ · pubmed ↗
- 5Dehlin M Jacobsson L Roddy E. Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol. (2020) 16:380–90. 10.1038/s 41584-020-0441-132541923 · doi ↗ · pubmed ↗
- 6Richette P Bardin T. Gout. Lancet. (2010) 375:318–28. 10.1016/S 0140-6736(09)60883-719692116 · doi ↗ · pubmed ↗
- 7Wu Z Yang X He Y Ni J Wang J Yin K . Environmental factors and risk of gout. Environ Res. (2022) 212:113377. 10.1016/j.envres.2022.11337735500858 · doi ↗ · pubmed ↗
- 8Hainer BL Matheson E Wilkes RT. Diagnosis, treatment, and prevention of gout. Am Fam Physician. (2014) 90:831–6.25591183 · pubmed ↗