Beyond Carrier Status: CFTR Heterozygosity as an Overlooked Clinical Risk Factor for Pancreatitis
Lucas D. Richter, Douglas M. Ruderfer, Josh F. Peterson, Lisa A. Bastarache

TL;DR
This study shows that being a carrier of a CFTR gene variant increases the risk of pancreatitis in women, but this risk is often overlooked in clinical practice.
Contribution
The study identifies CFTR heterozygosity as a novel clinical risk factor for pancreatitis that is not widely recognized.
Findings
CFTR carriers had a 4.68 times higher risk of acute pancreatitis compared to non-carriers.
CFTR carrier status was not clinically linked to pancreatitis diagnoses in medical records.
Integrating carrier screening results into EHRs could improve early diagnosis and personalized care.
Abstract
This study assessed the effect of CFTR pathogenic variant status, detected during prenatal carrier screening, for the incidence and clinical recognition of cystic fibrosis‐related phenotypes. Data were queried from the Vanderbilt University Medical Center clinical genetic database (CGdb), which includes clinically reported pathogenic variants and electronic health records (EHRs) from 2001 to 2023. Based on carrier screening results, we identified individuals heterozygous for a pathogenic CFTR variant and those who tested negative. Logistic regression tested associations between CFTR carrier status and 11 cystic fibrosis (CF)‐related phenotypes. A phenome‐wide association study (PheWAS) was performed to identify additional phenotypic associations, and manual chart review was conducted to evaluate recognition and clinical application of CFTR carrier status in patients diagnosed with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
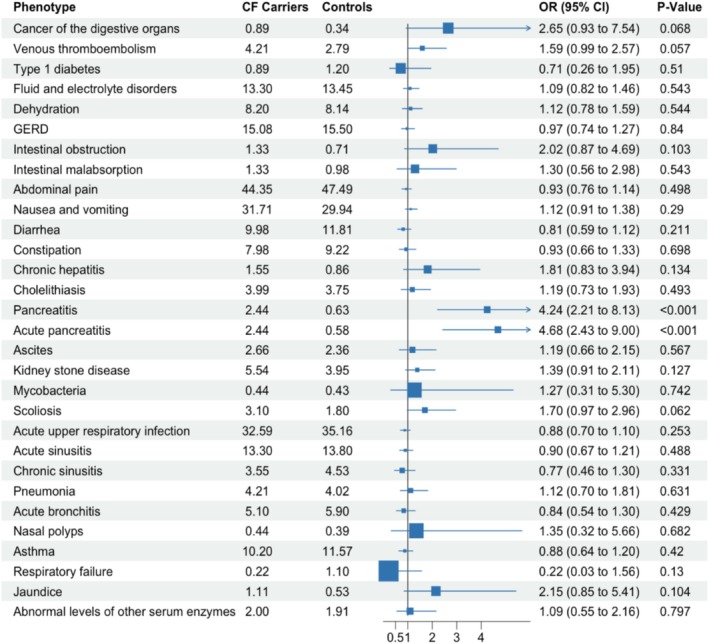 FIGURE 1
FIGURE 1| Metric | Value |
|---|---|
|
| 12 082 |
| Age (mean ± SD) | 34.42 ± 8.06 |
| Year of follow‐up (mean ± SD) | 7.39 ± 5.27 |
| EHR race/ethnicity | |
| White | 8397 (69.5%) |
| Black | 1605 (13.3%) |
| Hispanic | 1006 (8.3%) |
| Asian | 379 (3.1%) |
| Multiple/other | 392 (3.2%) |
| Unknown | 303 (2.5%) |
|
| 451 (3.7%) |
- —National Human Genome Research Institute (NHGRI) of the National Institutes of Health (NIH)10.13039/100000051
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCystic Fibrosis Research Advances · Pancreatitis Pathology and Treatment · Pediatric Hepatobiliary Diseases and Treatments
Introduction
1
Cystic fibrosis (CF) is a genetic disorder caused by variants in the CFTR gene, affecting multiple organ systems, including the lungs, pancreas, and digestive tract. CF manifests when an individual inherits two pathogenic variants in CFTR. While individuals carrying a single pathogenic CFTR variant do not develop classical CF, numerous population‐based studies suggest a modestly elevated risk of CF‐related phenotypes—most consistently pancreatitis—while effect sizes for respiratory conditions are small and sometimes nonsignificant.
Understanding of CFTR carrier risks has evolved [1]. Early studies found no significant differences between CFTR carriers and controls [2]. However, as sample sizes grew, risk factors began to emerge [3]. For example, in a study of over 1000 CFTR carriers, respiratory infections including sinusitis, bronchitis, and pneumonia were more common [4]. The largest study to date, involving nearly 20,000 CFTR carriers, found increased risk for 56 CF‐related phenotypes across multiple organ systems, including the bone, endocrine, respiratory, digestive, and reproductive systems [5]. Additionally, CFTR heterozygosity has been shown to be a strong risk factor for chronic pancreatitis (CP), with one study estimating that CFTR contributed to 24% of idiopathic CP cases [6]. Many additional studies have linked carrier status to CF‐related phenotypes, though reported risk profiles vary [4, 5, 7].
Despite extensive evidence suggesting CFTR carriers are at increased risk for certain conditions, clinical significance for individuals remains questionable. CFTR heterozygosity is a reported risk factor when discovered through genetic testing for pancreatitis. However, patients identified as CFTR carriers through non‐diagnostic testing, such as prenatal carrier screening, are not typically informed of risk [8, 9], Hence, the personal health implications for CFTR carriers identified through routine prenatal screening remain poorly understood. More studies are needed that examine clinical relevance in screened patients.
This study examines the personal health implications of CFTR carrier status using a cohort of over 12,000 women who underwent carrier screening. We address two key questions: (1) Are the CFTR‐related phenotypes identified in previous studies more prevalent among women found to be CFTR carriers through prenatal screening? (2) How do clinicians utilize this information? Notably, because CFTR carrier status is identified outside a diagnostic context, it is unclear if this information is typically correlated with patient symptoms. Our findings indicate that CFTR carriers identified via screening are more likely to have pancreatitis. However, clinicians often do not correlate these phenotypes to the CFTR genotype, even among symptomatic patients.
Methods
2
Data Used in This Study
2.1
Data was drawn from the clinical genetic database (CGdb), a database of clinical genetic tests extracted from electronic health records (EHRs) [10]. Included patients received prenatal screening for CFTR, either as a single gene or panel, from 2001 to 2023. Patients with a single pathogenic CFTR variant were considered carriers. We excluded patients with conflicting or biallelic variants [11]. Isolated findings of poly‐T tract polymorphisms were treated as benign. CFTR variants were annotated as residual versus minimal function (Table S1) [12]. Carrier screening tests and International Classification of Diseases (ICD) codes were restricted to those that occurred after age 15. Visit days were defined using ICD entry dates; the visit years variable was defined as the number of unique years a patient visited VUMC. ICD codes were translated to phecodeX [13].
Testing for Associations With Known
CFTR ‐Related Phenotypes
2.2
We attempted replication of the findings of Miller et al. in our cohort, using their reported 56 CF‐related phenotypes as targets of our analysis. We mapped 43 of these phenotypes to phecodeX, excluding those lacking relevance or a suitable phecode representation (Table S2). Prevalences of the CF‐related phenotypes were computed for carriers and unaffected controls. For respiratory phenotypes, we performed power calculations for detecting odds ratios (OR) of 1.5 and 2.0, and those from Miller et al. using a significance level (alpha) of 0.05 and assuming a two‐sided test. Using logistic regression, we tested for association between CFTR carrier status and target CF‐related phenotypes with at least 40 cases, using the phecode as the independent variable and carrier status as the main dependent variable. We included covariates for age at last visit, last year, EHR‐defined race/ethnicity, and number of visit years. To detect associations beyond those included in the targeted analysis, we conducted a phenome‐wide association (PheWAS) of CFTR carrier status using the same logistic regression model described above.
Assessing the Clinical Use of
CFTR Carrier Status in Affected Individuals
2.3
Chart review assessed whether clinicians linked carrier status to pancreatitis. Manual review was conducted by a genetic counselor, and information extracted included dates of pancreatitis diagnoses and whether CFTR carrier status was mentioned as a potential underlying cause.
Results
3
Cohort
3.1
The analysis included 12 082 women who underwent carrier screening, of which 451 carried a pathogenic CFTR variant. (Table 1.) We observed a carrier frequency of 3.73%, which is modestly higher than previously reported for North American populations [14]. The majority of the variants (n = 385; 85.4%) were minimal function, while the remainder were residual function (n = 67; 14.9%).
Underutilization and Misuse of ICD Codes Indicating
CFTR Carrier Status
3.2
Only 253 CFTR carriers (56.1%) received an ICD code indicating CFTR carrier status (ICD‐9 V83.81 or ICD‐10 Z14.1). Additionally, 22 patients with negative screening tests had an ICD for CFTR carrier status, 10 of whom tested positive for a poly‐T tract polymorphism alone, and the remainder whose screening tests were entirely negative.
Targeted Association Results
3.3
24 of 43 CF‐related phenotypes had an elevated prevalence among CFTR carriers (Table S3). The targeted logistic regression analysis revealed two statistically significant phenotypes: Acute pancreatitis (phecode GI_554.11) and Pancreatitis (GI_554.1, the parent phecode of GI_554.11). None of the eight respiratory phenotypes were statistically significant. (Figure 1). Six of eight respiratory phenotypes were powered at ≥ 80% to detect OR ≥ 2; all were underpowered to detect ORs reported in Miller et al. (Table S4). In a PheWAS of 1130 phenotypes, only pancreatitis and acute pancreatitis were significant following Bonferroni correction (Table S5).
Forest plot comparing the likelihood of CF‐related phenotypes between CF carriers and controls. The x‐axis displays odds ratios (ORs) with 95% confidence intervals, and corresponding p‐values. An OR > 1 indicates increased odds of the phenotype among CF carriers relative to controls. Notably, pancreatitis and acute pancreatitis show significantly elevated odds in CF carriers (p < 0.001).
Assessing for Clinical Correlations Among
CFTR Carriers With Pancreatitis
3.4
Acute pancreatitis was rare in the cohort, with a prevalence of 2.44% among CFTR carriers and 0.63% among controls. However, the likelihood of being a CFTR carrier given an acute pancreatitis diagnosis was quite high; nearly one in seven patients with pancreatitis (14.1%). Among the 11 CFTR carriers who developed pancreatitis, one (9.1%) carried a residual function variant, and 10 (91%) had minimal function variants vs. 14.9% of the overall cohort; this difference was not statistically significant (Fisher's exact test, p > 0.05). Chart review corroborated all pancreatitis diagnoses in CFTR carriers and demonstrated that carrier screening results were never used for diagnostic refinement. Seven patients had confirmed pathogenic CFTR variants prior to their pancreatitis diagnosis with a mean of 5 years from genetic testing to pancreatitis diagnosis. Four patients received CFTR testing after their pancreatitis diagnosis: two following pancreatitis panels yielding only monoallelic CFTR variants, which led to expanded carrier screening for family planning; one with first‐trimester pancreatitis, screened within 1 month; and one 12 years after initial pancreatitis. Only the two patients tested after a pancreatitis panel had clinical recognition of CFTR‐mediated risk. Of the six patients with noted etiological basis for pancreatitis, three had gallstone‐related, and three post‐Endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis.
Discussion
4
In this study, we found that women identified as CFTR carriers through prenatal carrier screening have a significantly higher risk of developing pancreatitis. This result aligns with previous studies linking CFTR heterozygosity to pancreatitis [1, 3, 5, 6]. Our study has several strengths. First, we identified CFTR carriers using clinical genetic testing, ensuring the accuracy of our genotyping data. Second, our study was conducted in a real‐world clinical population, allowing us to evaluate the clinical significance of CFTR carrier status in a practical, real‐world scenario.
Our review of patient records indicates that the connection between carrier status and pancreatitis diagnosis is typically overlooked. This oversight is likely due, in part, to the way genetic test results are stored in the EHR. In most cases, carrier screening results were saved as PDF documents, making them difficult to search and integrate into clinical workflows [10]. Additionally, pancreatitis diagnoses often occurred years after the CFTR carrier status was first documented, further complicating the recognition of this connection.
We did not observe an increased risk for respiratory conditions, which have been observed even in studies based on smaller cohorts. Several factors may explain this discrepancy. First, while we were powered to detect associations for six respiratory phenotypes with moderate effect sizes, we were underpowered to detect smaller effect sizes reported in larger studies, including Miller et al. Second, most prior studies identified CFTR carriers using ICD claims data or inferred carrier status based on CF diagnoses in first‐degree relatives. These methods may introduce bias through undetected compound heterozygosity, ascertainment bias from the selective detection of CFTR variants in a population, or misclassification due to incorrect ICD codes (as observed in this study). Third, previous studies were based on heterogeneous cohorts, encompassing pediatric and adult patients. Our study focused on women of reproductive age. These cohort differences may influence the relationship between CFTR carrier status and CF‐related phenotypes.
Additionally, our study highlights a potential path for future research by leveraging clinical genetic testing data to explore genotype–phenotype relationships without requiring new genotype data from research settings. As clinical genetic data continues to accumulate in electronic health records, multi‐institutional collaborations and integration with national biobanks could improve power to assess lower‐penetrance CFTR‐related outcomes.
Although carrier screening tests are not intended for diagnostic purposes, our findings suggest that these results may have significant personal health implications. While only a small proportion of CFTR carriers develop pancreatitis, a significant subset of patients with pancreatitis were found to be CFTR carriers. While routine follow‐up may not be necessary for every CFTR carrier, a system that alerts clinicians to a patient's CFTR carrier status could be highly valuable when pancreatitis is diagnosed or suspected. Implementing EHR infrastructure that organizes and stores genetic test results would allow for more effective clinical utilization, ensuring that CFTR carrier status is readily available—and clinically actionable—if patients present with relevant symptoms. However, barriers to implementation remain. Most clinical genetic test results are currently stored in unstructured, non‐computable formats, limiting their accessibility for clinical decision support [10]. Additionally, clinician awareness of actionable findings may be limited, and variability across EHR systems complicates the integration of structured genetic data into clinical workflows. This study highlights one use‐case among many for how integrating genetic test results into the EHR could improve patient care.
Integrating genetic data into clinical workflows may enhance precision medicine and improve outcomes for individuals with CFTR variants [15, 16]. Identifying pathogenic CFTR variants in patients with pancreatitis clarifies etiology, enables timely diagnosis, and guides management—potentially including CFTR modulators (e.g., ivacaftor), which are currently only approved for patients with formal diagnoses of CF. However, preliminary reports suggest potential benefit for patients with CFTR‐related pancreatitis, but reported benefits and risks are inconsistent [17, 18, 19]. Overlooking CFTR status may lead to diagnostic delays, misaligned treatments, and potentially unnecessary procedures such as ERCP, which can increase complications or even trigger pancreatitis [1, 7]. Making genetic carrier status searchable in EHRs could enable clinicians to implement proactive screening and prevention strategies, such as promoting lifestyle changes to reduce pancreatitis risk or monitoring for gastrointestinal cancers.
This study has limitations. First, it was conducted in a single academic medical center. To establish the generalizability of our findings, external replication is needed. Second, because our cohort is relatively young, we may have missed significant associations with CF‐related phenotypes that occur later in life, such as degenerative pulmonary diseases and cancers. Indeed, we found digestive system cancers were 2.7 times higher in CFTR carriers than controls, echoing a finding reported in a UK biobank study of older CFTR carriers—although not significant in the 44 cases analyzed here [20]. Additional longitudinal data is needed to fully evaluate later onset conditions and phenotypes that might present more commonly in men—not represented here. Third, CFTR testing in our cohort was primarily performed with limited panels, consistent with standard practice at the time. Therefore, we cannot exclude the possibility of undetected second CFTR variants, modifier alleles, or other pancreatitis‐associated gene variants (i.e., SPINK1, PRSS1, or CTRC). Finally, while our cohort was larger than many previous studies of CFTR carriers, we were underpowered to detect associations for rare phenotypes or small effect sizes.
Conclusion
5
This study highlights the clinical significance of CFTR carrier status that is incidentally discovered through carrier screening, pointing out a potential missed opportunity to correlate these genetic findings with clinical diagnoses. It also illustrates the differences between research observations and real‐world clinical scenarios, emphasizing the potential to leverage clinical genetic testing data to enhance patient care.
Author Contributions
L.A.B.: conceptualization. L.A.B. and L.D.R.: data curation. L.A.B.: formal analysis. L.A.B., L.D.R.: investigation. L.A.B. and L.D.R.: methodology. L.A.B.: visualization. L.A.B. and L.D.R.: writing – original draft. L.A.B., L.D.R., D.M.R., and J.F.P: writing – review and editing. L.A.B.: supervision.
Ethics Statement
This study was reviewed by the Vanderbilt University Medical Center IRB 171011. All clinical data were de‐identified prior to use.
Conflicts of Interest
L.D.R. and J.F.P. declare no conflicts of interest. L.A.B. receives royalties from Nashville Biosciences, and D.M.R. has served on advisory boards for Illumina and Alkermes and has received research funds unrelated to this work from PTC Therapeutics and Sanofi.
Peer Review
The peer review history for this article is available at https://www.webofscience.com/api/gateway/wos/peer‐review/10.1111/cge.14780.
Supporting information
Data S1. Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1P. M. Polgreen and A. P. Comellas , “Clinical Phenotypes of Cystic Fibrosis Carriers,” Annual Review of Medicine 73 (2022): 563–574.10.1146/annurev-med-042120-020148 PMC 888470135084992 · doi ↗ · pubmed ↗
- 2W. Y. Hallett , A. G. Knudson, Jr. , and F. J. Massey, Jr. , “Absence of Detrimental Effect of the Carrier State for the Cystic Fibrosis Gene,” American Review of Respiratory Disease 92 (1965): 714–724.5846055 10.1164/arrd.1965.92.5.714 · doi ↗ · pubmed ↗
- 3C. Castellani , C. Quinzii , and S. Altieri , “A Pilot Survey of Cystic Fibrosis Clinical Manifestations in CFTR Mutation Heterozygotes,” Genetic Testing 5 (2001): 249–254.11788092 10.1089/10906570152742317 · doi ↗ · pubmed ↗
- 4P. M. Polgreen , G. D. Brown , and D. B. Hornick , “CFTR Heterozygotes Are at Increased Risk of Respiratory Infections: A Population‐Based Study,” Open Forum Infectious Diseases 5 (2018): ofy 219.30397620 10.1093/ofid/ofy 219PMC 6210382 · doi ↗ · pubmed ↗
- 5A. C. Miller , A. P. Comellas , and D. B. Hornick , “Cystic Fibrosis Carriers Are at Increased Risk for a Wide Range of Cystic Fibrosis‐Related Conditions,” Proceedings of the National Academy of Sciences of the United States of America 117 (2020): 1621–1627.31882447 10.1073/pnas.1914912117 PMC 6983448 · doi ↗ · pubmed ↗
- 6E. Masson , J. M. Chen , and M. P. Audrézet , “A Conservative Assessment of the Major Genetic Causes of Idiopathic Chronic Pancreatitis: Data From a Comprehensive Analysis of PRSS 1, SPINK 1, CTRC and CFTR Genes in 253 Young French Patients,” P Lo S One 8 (2013): e 73522.23951356 10.1371/journal.pone.0073522 PMC 3738529 · doi ↗ · pubmed ↗
- 7A. O. Nielsen , S. Qayum , and P. N. Bouchelouche , “Risk of Asthma in Heterozygous Carriers for Cystic Fibrosis: A Meta‐Analysis,” Journal of Cystic Fibrosis 15 (2016): 563–567.27324553 10.1016/j.jcf.2016.06.001 · doi ↗ · pubmed ↗
- 8J. L. Deignan , C. Astbury , and G. R. Cutting , “CFTR Variant Testing: A Technical Standard of the American College of Medical Genetics and Genomics (ACMG),” Genetics in Medicine 22 (2020): 1288–1295.32404922 10.1038/s 41436-020-0822-5PMC 8268680 · doi ↗ · pubmed ↗