Risk factors for angiotensin converting enzyme inhibitor angioedema in a South African population
Cascia Day, Lovemore Mapahla, Melissa Ribeiro, Mimi Deetlefs, Cathryn McDougall, Adelein Engelbrecht, Erika Jones, Sarah Pedretti, Jonny Peter

TL;DR
This study identifies Black genetic ancestry and calcium channel blocker use as risk factors for angioedema caused by ACE inhibitors in a South African population.
Contribution
The study characterizes ACEI angioedema risk factors in a diverse African population, highlighting novel associations with genetic ancestry and drug use.
Findings
Black genetic ancestry was a significant risk factor for ACEI angioedema.
Calcium channel blocker use increased the risk of ACEI angioedema.
Most angioedema cases occurred after several years of ACEI treatment.
Abstract
Angiotensin converting enzyme inhibitors (ACEI) have proven mortality and morbidity benefit in hypertension, ischemic heart disease, heart failure, and renal disease and are among the most prescribed medications globally. ACEI angioedema (AE-ACEI) is a potentially life-threatening adverse drug reaction that is reported to occur more frequently in African American populations. However, the clinical profile of AE-ACEI is poorly characterized in diverse African populations. A case-controlled cohort study with enrolment of AE-ACEI cases and drug-tolerant controls in Cape Town, South Africa. Univariable and multivariable analysis was performed. Controls were defined as patients tolerating ACEI for a minimum of two years. Cases were defined as patients who had angioedema while using an ACEI, patients with a history of angioedema while not on an ACEI were excluded. Cases and controls were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
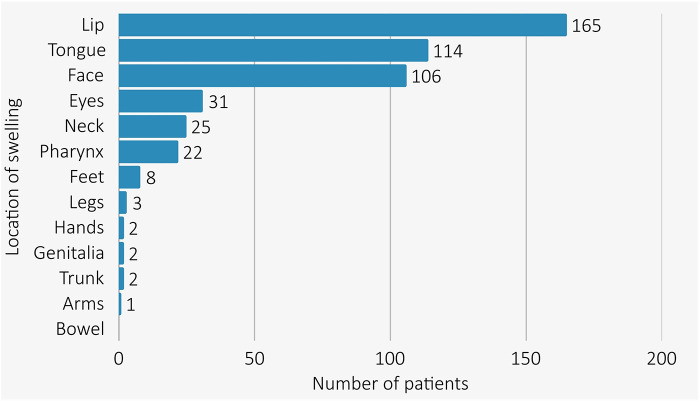 Figure 1
Figure 1| Intrinsic patient risk factors | Environmental factors |
|---|---|
| African race as risk factor ( | Habits |
| Age greater than or equal to 65 years ( | Smoking ( |
| Female gender ( | Medication |
| Male gender ( | Use of Calcium Channel blockers ( |
| Increased BMI ( | Use of antihistamines ( |
| Comorbid illness | Use of NSAIDs ( |
| C1 inhibitor deficiency or defect ( | Use of immunosuppressants ( |
| History of allergic rhinitis ( | Use of diuretic ( |
| Seasonal allergies ( | Use of systemic corticosteroids ( |
| DM increased risk ( | Higher ACEI doses ( |
| Hypertension ( | Use of statins ( |
| Rheumatoid Arthritis ( | Use of anti-diabetic drugs ( |
| COPD ( | Other |
| History of drug induced rash ( | Trauma ( |
| CKD ( | Recent hospitalisation ( |
| Hyperlipidaemia ( | Pollen ( |
| Autoimmune disease ( | Spring season ( |
| Rheumatoid arthritis ( | |
| Known drug allergy ( | |
| Solid organ transplant ( | |
| Malignancy ( | |
| Anaemia ( | |
| Atopic dermatitis ( | |
| Other factors | |
| Highest rate of AE-ACEI within 30 days of starting ACEI ( | |
| Recent reinitiation of ACEI ( | |
| Unilateral angioedema ( | |
| Absence of urticaria or itch ( | |
| Angioedema of the lips ( | |
| Polypharmacy ( | |
| No history of other ACEI use ( | |
| ACEI cough ( |
| Variable | All, | ACEI angioedema cases, | Controls, | |
|---|---|---|---|---|
| Age, years med (IQR) | 58 (47;67) | 57 (47;68) | 59 (46;67) | 0.7 |
| Female, n(%) | 390 (57.5) | 132 (62.0) | 258 (55.4) | 0.092 |
| Ancestry from genotype, n(%), | ||||
| White | 29 (5.2) | 1 (0.6) | 28 (6.9) |
|
| Admixed | 332 (59) | 72 (47) | 260 (64) | |
| Black | 200 (36) | 81 (53) | 119 (29) | |
| Genotype not available | 118 (17.4) | 59 (27.6) | 59 (12.6) | |
| Location of recruitment | ||||
| Out patient department | 425 (62.6) | 122 (57.3) | 304 (65.2) | |
| Emergency room | 221 (32.5) | 81 (38) | 140 (30) | |
| General inpatient | 31 (4.6) | 8 (3.8) | 23 (4.9) | |
| High care or intensive care unit | 2 (0.3) | 2 (0.9) | 0 (0) | |
| Comorbidities | ||||
| Hypertension | 662 (97.5) | 210 (98.6) | 452 (97) | 0.20 |
| Hypercholesterolemia | 325 (47.9) | 83 (39) | 242 (51.9) | |
| Diabetes | 237 (34.9) | 67 (31.5) | 170 (36.5) | 0.202 |
| Atopy | 195 (28.7) | 69 (32.3) | 126 (27.6) | 0.201 |
| Cardiac disease | 128 (18.9) | 27 (12.2) | 101 (21.9) | |
| Cardiac failure | 119 (17.5) | 20 (9.4) | 99 (21.2) | |
| HIV | 89 (13.2) | 36 (16.9) | 53 (11.4) | |
| Vascular disease | 53 (8) | 15 (7) | 38 (8.2) | 0.615 |
| Chronic kidney disease | 51 (7.5) | 10 (4.7) | 41 (8.8) | 0.060 |
| Prevalence of previously reported risk factors for AE-ACEI, n(%) | ||||
| Fitz Patrick V-VI skin tone | 254 (38.3) | 108 (50.7) | 146 (31.3) | |
| Over 65 years old | 219 (32.3) | 63 (29.6) | 156 (33.5) | 0.313 |
| Allergic rhinitis | 117 (17.2) | 37 (17.4) | 80 (17.2) | 0.948 |
| On immunosuppression | 34 (5) | 8 (3.8) | 26 (5.6) | 0.312 |
| NSAID use | 162 (23.9) | 43 (20) | 119 (26) | 0.129 |
| Diuretic use | 465 (68) | 154 (72.0) | 311 (67.0) | 0.148 |
| Statin use | 355 (52.3) | 88 (41.0) | 267 (57.0) | |
| Calcium channel blocker use | 367 (54.1) | 135 (63) | 232 (50.0) | |
| Oral steroids | 7 (1.1) | 4 (1.9) | 3 (0.6) | 0.089 |
| Oral antihistamines | 68 (10.6) | 19 (8.9) | 49 (10.5) | 0.900 |
| >3 medications (polypharmacy) | 565 (83.2) | 181 (85.0) | 384 (82.4) | 0.405 |
| Increased stress | 47 (22.1) | |||
| Acute illness | 20 (9.4) | |||
| New chronic illness | 18 (8.5) | |||
| Use of over the counter medications | 16 (17.0) | |||
| Characteristic | Unadjusted | Adjusted | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI OR | aOR | 95% CI aOR | |||
| Age | 1.00 | 0.99–1.01 | 0.70 | 1.01 | 1.01–1 | 0.11 |
| Male | 0.75 | 0.54–1.05 | 0.092 | 0.95 | 0.62–1.45 | 0.8 |
| Admixed ancestry | 7.75 | 1.61–139 | 0.046 | 6.16 | 1.22–112 | 0.081 |
| Black ancestry | 19.10 | 3.94–343 | 0.004 | 15.30 | 2.94–283 | |
| Atopy | 1.23 | 0.87–1.75 | 0.2 | 1.44 | 0.92–2.25 | 0.11 |
| HIV | 1.60 | 1.01–2.52 | 0.045 | 1.08 | 0.58–1.98 | 0.8 |
| Hypertension | 2.17 | 0.70–9.48 | 0.20 | 0.3 | 0.05–1.87 | 0.2 |
| Elevated cholesterol | 0.60 | 0.43–0.83 | 0.002 | 1.44 | 0.78–2.70 | 0.20 |
| Cardiac Failure | 0.39 | 0.23–0.63 | <0.001 | 0.43 | 0.22–0.82 | |
| Chronic Kidney Disease | 0.51 | 0.24–1.00 | 0.064 | 0.24 | 0.05–0.72 | |
| Immunosuppressive drug use | 0.66 | 0.28–1.42 | 0.3 | 0.94 | 0.29–2.62 | >0.90 |
| NSAID use | 0.74 | 0.49–1.09 | 0.13 | 1.23 | 0.69–2.15 | 0.50 |
| Statin use | 0.52 | 0.38–0.73 | <0.001 | 0.36 | 0.19–0.65 | |
| Calcium channel blocker use | 1.75 | 1.25–2.44 | 0.001 | 1.77 | 1.17–2.72 | |
| Hospitalised | 1.39 | 0.99–1.93 | 0.053 | 1.66 | 1.07–2.58 | |
- —South African Medical Research Council10.13039/501100001322
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoagulation, Bradykinin, Polyphosphates, and Angioedema · Renin-Angiotensin System Studies · Blood Coagulation and Thrombosis Mechanisms
Introduction
Angiotensin converting enzyme inhibitors (ACEI) are a class of antihypertension medications that inhibit the Angiotensin Converting Enzyme (ACE; also known as kinase II). ACE is responsible for the conversion of angiotensin I to angiotensin II, as well as degradation of the vasoactive peptide bradykinin. ACEI are one of the most widely used medications globally as a result of their affordability, and many large studies have demonstrated their efficacy in the treatment of hypertension (1), cardiac failure (2, 3), ischemic heart disease (4), and chronic renal disease (5). ACEI also show improved efficacy, when compared to angiotensin receptor blockers (ARBs), in preventing hypertension related cardiovascular events, and all-cause mortality (6). Baptiste et al. found that when comparing ACEI to ARBs in hypertensive patients that in the Black African cohort ARB use was associated with a higher risk of cardiovascular related death when compared to ACEI [HR 1.2 (95% CI: 1.02–1.4)]. The two major adverse drug reactions with ACEI are cough and angioedema.
Angioedema is defined as localised swelling in subcutaneous and submucosal tissues. The frequency of AE-ACEI varies from 0.2% to 1% (7), but ubiquitous use of these medications means that AE-ACEI is the most common single cause of angioedema globally, including in South Africa (8–11). AE-ACEI most commonly affects the head and neck (12–14), with mortality rates reported as high as 11%, and intubation rates at 22% internationally (9, 12, 15). Several studies have investigated epidemiological and clinical risk factors for AE-ACEI (see Table 1) with consistent identified risk factors including: African American ancestry (with a 3–5 times increased AE-ACEI angioedema frequency) (10, 13, 16–18, 20, 23, 26, 40), female gender (17, 20, 21), older age (12, 16, 20–22), use of immunosuppression (25, 29, 30), and seasonal allergies (16, 21, 36). Additional identified risk factors (with some conflicting findings) include a variety of concomitant medications (18, 20–22, 25, 30, 41, 42), current smoking status (16, 23–25), and obesity (16, 22). The recent initiation of ACEI and first 30 days of treatment with ACEI have previously been identified as the highest risk period for AE-ACEI (17, 18, 26, 29, 37–39). Most of these epidemiological studies of AE-ACEI are from High Income Countries (HICs) and predominantly European populations, despite the reported increased risk in African Americans. Thus, the aim of this study was to examine the clinical profile and assess risk factors for AE-ACEI in an African setting.
Methods
This is a case control study comparing patients who tolerate ACEI vs. patients who have developed AE-ACEI. We aim to describe this cohort of patients and identify significant risk factors for AE-ACEI in this community. AE-ACEI cases were defined as participants who developed angioedema while on an ACEI, with no history of angioedema while not using an ACEI. ACEI tolerant controls were defined as participants who had safely tolerated an ACEI for at least two years, with no history of angioedema. In this study, AE-ACEI cases were identified both prospectively (through referral) and retrospectively (through folder review). Cases and matched controls were recruited from seven sites: District 6 Clinic, Victoria Wynberg Hospital, Mitchell's Plain District Hospital, Heideveld Emergency Centre, Green Point Clinic, The University of Cape Town Lung Institute Allergy and Immunology Clinic, and Groote Schuur Hospital (GSH) (allergy division, emergency unit, hypertension clinic, and general medical wards). All the above facilities are primary or secondary level centers that refer to GSH and the demographics of this cohort match the demographics of the Western Cape Province (see Supplement for more information about each facility, a detailed description of recruitment at each site as well as consort diagrams, Supplementary Figures 1, 2). The Western Cape Provincial Health Data Centre (PHDC) team assisted with accessing HECTIS admission data (43). All cases and controls were interviewed in person, and all data was assessed by an Allergist/Allergy Medical Officer. Information regarding angioedema history, medical history, and demographics was collected. This study is part of the Angioedema Biomarkers in Africa project, which has been approved by the University of Cape Town Human Research Ethics Committee (HREC 057/2020).
We acknowledge that neither self-reported race nor Fitpatrick skin tone accurately captures genetic ancestry. Therefore, we have decided to group patients based on our available genetic ancestry data into White ancestry, Admixed ancestry, and Black ancestry based on location and grouping in the Principle Component Analysis plot (Supplementary Figure 3) from our previous genome wide association study in this cohort. We did not have genotype data for 118/679 (17.4%) of patients.
Proportions and frequencies were used to describe categorical variables. Normally distributed variables, tested using the Shapiro Wilk test of normality, were described using mean and standard deviation or else median and interquartile range was used. The mean difference test in continuous variables that were normally distributed between groups was done using the analysis of variance (ANOVA) or else the Kruskal Wallis test was used. Proportion difference test for all categorical variables that had at least 5 observations across all groups was done using the Chi square test of independence, or else the Fisher's exact test was applied. All statistical tests were done at 5% level of significance, and Stata 15.1 software was used for the analyses (44). Multivariable analysis was performed for this cohort with AE-ACEI as the outcome. Patients were stratified as “hospitalised” (including patients in general medical wards, intensive care or high care units, and the emergency center) or “not hospitalised” (patients from outpatient departments.). The following covariates were included: age, gender, skin tone, atopy, Human immunodeficiency virus (HIV), hypertension, elevated cholesterol, cardiac failure, and chronic kidney disease. Key selected medications included: immunosuppression, NSAIDs, Statins, and Calcium channel blockers. Cardiac disease was removed from the model as there was evidence of collinearity with cardiac failure. Multicollinearity was assessed using The Variance Inflation Factor (VIF) (Supplementary Table 2), and all results were less than 5. Adjusted odds ratios (aOR) with respective 95% confidence intervals (CI) were reported. There was minimal missing data in chosen co-variates (see Supplementary Table 6). We performed Multivariable analysis for this cohort with AE-ACEI within 30 days of initiating treatment as the outcome, but no covariates reached significance (Supplementary Table 3).
Results
A total of 237 AE-ACEI cases and 466 ACEI tolerant controls were enrolled. Between June 2021 and December 2024, 49 cases of acute AE-ACEI were referred to the GSH Allergy team, while 188 participants with a history of prior AE-ACEI were retrospectively enrolled via folder review and interview. In the AE-ACEI angioedema cases, 24 participants were excluded, as they had evidence of immediate drug hypersensitivity (urticaria n = 10; pruritis n = 13; anaphylaxis n = 1) as determined by two allergists (Supplementary Figures 1, 2). Most of our cohort were treated with the ACEI enalapril [99.7%, (699/701)]. In the ACEI tolerant controls the duration on an ACEI at the time of enrollment was median 9.5 years (IQR: 5; 15.5 years).
In the overall cohort, the median age was 58 years (IQR: 47; 67), 57.5% were female, and 94.8% (532/561) were classified as Admixed or Black ancestry (see Table 2). The cases and controls were similar in terms of age and gender, but significantly more AE-ACEI cases were classified as Black ancestry when compared to controls [53% (81/154), vs. 29%% (119/407), p < 0.001]. With regards to comorbid illness, 97.5% of patients had hypertension. HIV was more prevalent in the AE-ACEI cases [16.9% (36/213) vs. 11.4% (53/466), p = 0.043] but immunosuppressive treatment did not differ between cases and controls. Compared to cases the controls had significantly higher rates of hypercholesterolaemia [51.9% (242/466) vs. 39.0% (83/213), p = 0.001], cardiac disease [21.9% (102/466) vs. 12.2% (26/213), p = 0.006], or had previously tested positive for COVID-19 [16.3% (76/466) vs. 12.2% (26/213), p = 0.001]. Atopy was reported in 32.3% (69/213) of cases and 27.6% (126/466) of controls but the results did not reach significance (p = 0.201). The cases had significantly higher rates of asthma [42.0% (29/69) vs. 20.9% (27/129), p = 0.001], while atopic dermatitis was more common in the controls [31% (40/129) vs. 8.6% (8/69), p = 0.023]. Calcium channel blockers use was significantly greater in the cases [135/213 (63%) vs. 232/466 (50%), p < 0.001] while simvastatin use was significantly more common in the controls [267/466 (57%) vs. 88/213 (41%), p < 0.001]. In multivariable analysis Black ancestry (aOR 15.3; 95% CI 2.94–283, p = 0.01), calcium channel blocker usage (aOR 1.77; 95% CI: 1.17–2.72, p = 0.008) were significant risk factors for developing AE-ACEI (Table 3). Chronic kidney disease, cardiac failure, and statin use were protective in this model.
In our cohort the duration of ACEI treatment before developing angioedema median of 6.9 years (IQR: 2.9; 13.0 years) with 31.5% (67/213) of patients developing angioedema within 30 days of ACEI initiation. The median duration of AE-ACEI was 48 h (IQR: 24; 72 h). Multivariable analysis for developing AE-ACEI within 30 days of initiating treatment found no significant covariates (Supplementary Table 3).
All AE-ACEI cases had swelling above the shoulders (see Figure 1) with the lip [72.3% (154/213)] and tongue [50.2% (107/213)] being the most common sites of swelling. Overall, 22 (10.3%) patients developed pharyngeal angioedema (10/22 with concomitant tongue and lip swelling), with two patients requiring intubation for airway protection (one emergency orotracheal intubation, and one emergency cricothyroidotomy both after reinitiation of an ACEI in patients with known AE-ACEI). There were no angioedema related deaths. Hospitalisation was required in 82.2% (175/213) of AE-ACEI cases. Information about treatment of AE-ACEI was available for 41.8% of cases (89/213). Therapy with fresh frozen plasma was given in 11 cases (11/89, 12.4%) while 73% (65/89) were treated with antihistamines, 64% (57/89) with corticosteroids, and 12.4% (12/89) required adrenaline for airway protection. One patient received Icatibant peri-intubation after discussion with our Angioedema Hotline.
Bar graph describing distribution of AE-ACEI location in cases.
Discussion
AE-ACEI is a common and potentially life-threatening complication of ACEI use, and the global rate of acute ACEI requiring care in emergency centers is rising (45, 46). To date there are no available tests or biomarkers to predict which patients are at risk of developing AE-ACEI. Currently, clinical risk factors remain the best clues to identify at-risk groups—however, these risk factors may be population-specific with limited data from diverse African countries. This large South African cohort of AE-ACEI and drug-tolerant controls were examined for traditional and novel risk factors. AE-ACEI cases more commonly had Black genetic ancestry, a higher prevalence of HIV, and lower rates of concomitant metabolic and non-hypertensive cardiovascular diseases. Notably, the majority of AE-ACEI occurred following prolonged periods of treatment, and there was increased occurrence during the spring/summer seasons. Interestingly, we also found that all patients had angioedema of the face and neck. Despite high rates of hospitalisation there were low rates of intubation (0.9%) for airway protection, and no deaths. This is contradictory to international data where 22% (37) to 32% (13) of patients with AE-ACEI required intubation, and 11% demised (37). Unlike international groups, we did not find that older age, female gender, allergic rhinitis, or immunosuppressive therapy were associated with AE-ACEI. However, similar to international data, we found that calcium channel blockers were a significant risk factor (21, 22, 24).
In 1996, Brown et al. (18) were the first to describe an increased risk for AE-ACEI in African Americans with a relative risk of 4.5 compared to white Americans. They also found that African patients were more likely to have severe hypertensive disease as they required higher doses of ACEI, as well as having more severe AE-ACEI with higher rates of hospitalisation and intubation for airway protection. Later studies in the USA (10, 13, 16, 17, 20, 23, 41) and a systematic review (40) found that black and Hispanic patients had a significantly higher risk of AE-ACEI compared with patients with paler skin tone (41). However, other authors from the USA have found that African race were not associated with AE-ACEI (12, 19). Studies completed in Sweden, the United Kingdom, and Thailand either did not describe racial demographics (21), or had no patients with darker skin tones (24, 39) (see Supplementary Table 5 for a summary of these studies). Our data from an African Middle Income Country (MIC) setting does find a significantly higher prevalence of Black genetic ancestry in AE-ACEI cases with a high aOR of 15.3 (p = 0.01 (Table 3). This result aligns with African American data and suggests that examining African populations for genetic risk factors for AE-ACEI is warranted. We have recently published a GWAS from this cohort and we replicated findings for the single nucleotide polymorphisms (SNP) rs500766 on chromosome 10 (previously linked to AE-ACEI). We also found SNPs located close to the genes PRKCQ (protein kinase C theta), RAD51B (RAD51 Paralog B), and RIMS1 (regulating synaptic membrane exocytosis 1), which have previously been linked with drug-induced angioedema. Additionally, SNPs near the CSMD1 (CUB and sushi multiple domains 1) gene, which has been linked to ACEI cough (47), were identified. We have highlighted that further work across diverse African populations is justified, as given African genomic diversity extrapolation to all darker skinned populations would be flawed (48).
AE-ACEI can occur immediately upon drug exposure, or years into therapy, and its occurrence cannot be predicted. Some authors have found that AE-ACEI is most common within the first 30 days of starting treatment, reporting that 48.6–53.0% of AE-ACEI cases occur within that window (17, 18, 39), while others have found much lower AE-ACEI rates of 10.2% within the first month of treatment (15, 39, 41). Our cohort had a long drug latency, with only 31.1% developing AE-ACEI within the first 30 days of drug initiation, which is within range of global rates. In AE-ACEI this prolonged drug latency raises the question of whether there is an additional factor/second hit event in the late presenters which i) either effects other enzymes that metabolise bradykinin, such as neprilysin, or aminopeptidase P, ii) may represent another factor that leads to increased flux through the bradykinin pathway, potentially even at the tissue-level, or iii) represents the onset of a chronic urticaria/angioedema variant independent of AE-ACEI. A recent publication by Bocquet et al. found that, on review of reported AE-ACEI angioedema cases that almost 50% of patients were excluded, and that these patients likely had mast cell mediated angioedema rather than AE-ACEI (49).
All of our AE-ACEI cases presented with swelling above the shoulders, most commonly affecting the lips and tongue, aligning with global findings (14, 36). Previous studies have identified tongue swelling in AE-ACEI as a marker associated with poor clinical outcomes and increased likelihood of intensive care admissions (13, 15). Other forms of bradykinin mediated angioedema—such as hereditary angioedema and acquired angioedema—can affect multiple body sites, including the oropharynx, abdominal viscera, limbs, and genitalia (50). If AE-ACEI is also bradykinin mediated, one would expect it to involve a broader range of anatomical sites. The density of mast cells in tissue is higher in the face than other anatomical areas (51); so a possible explanation is that ACEI treatment is unmasking mast cell mediated angioedema (i.e., ACEI are acting as a cofactor). This is supported by recent findings of high rates of mast cell mediated angioedema in patients who developed recurrent angioedema after exposure to ACEI. Douillard et al. found that 41% of patients with a suspected ACEI/ARB angioedema still had recurrent angioedema without urticaria more than 6 months after stopping the drug, indicating a diagnosis of mast cell mediated angioedema rather than bradykinin mediated angioedema in these patients (52). These findings are important and underline the need for future investigations into the pathomechanisms of AE-ACEI, and potentially cross-talk between mast-cells and kallikrein-kinin pathways.
This study is the largest study to date describing AE-ACEI in an African MIC. Our limitations include prospective case finding, which was reliant on referrals from local sites; as well as retrospective case finding which is dependent on existing ICD10 coding and local databases. We encountered difficulties in contacting retrospective cases to schedule in-person interviews because of a highly migrant population, and incorrect or outdated contact details. Our cohort had higher rates of hypertension and dyslipidaemia than reported in South Africa (53), which likely reflects our recruitment from hospitals and local clinics, rather than the general population. However, ACEI are most commonly prescribed for hypertension, so high hypertension rates (and associated metabolic conditions) in this cohort are not an unexpected finding. The case-controlled nature of the study cannot exclude potential for unintentional selection bias; however, cases and controls were recruited from the same hospitals and drainage populations. It is also important to note that as this study is nested in the government funded state sector, almost all our cohort were using Enalapril, which is the ACEI on government tender. We did have some variables with high rates of missing data—especially with regards to treatment of AE-ACEI—as participants either did not know or could not recall the treatment that was received at the time of the event.
In summary, we have shown that Black genetic ancestry, calcium channel blocker use, and HIV co-infection are important risk factors for AE-ACEI—and that previously identified risk factors including older age, female sex, and allergic rhinitis were not risk factors in this cohort. We have also identified a long drug latency compared to international cohorts. These findings highlight the need for further epidemiological and clinical studies on AE-ACEI in diverse ethnic backgrounds and LMIC settings to provide a true global clinical understanding of AE-ACEI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Williams GH. Converting-enzyme inhibitors in the treatment of hypertension. N Engl J Med. (1988) 319(23):1517–25. 10.1056/NEJM 1988120831923053054561 · doi ↗ · pubmed ↗
- 2Swedberg K Kjekshus J, CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. (1987) 316(23):1429–35. 10.1056/NEJM 1987060431623012883575 · doi ↗ · pubmed ↗
- 3Yusuf S Pitt B Davis CE Hood WB Cohn JN. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. (1991) 325(5):293–302. 10.1056/NEJM 1991080132505012057034 · doi ↗ · pubmed ↗
- 4TAIREA Study. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. The acute infarction ramipril efficacy (AIRE) study investigators. Lancet. (1993) 342(8875):821–8. 10.1016/0140-6736(93)92693-N 8104270 · doi ↗ · pubmed ↗
- 5Lewis EJ Hunsicker LG Bain RP Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The collaborative study group. N Engl J Med. (1993) 329(20):1456–62. 10.1056/NEJM 1993111132920048413456 · doi ↗ · pubmed ↗
- 6Peresuodei TS Gill A Orji C Reghefaoui M Saavedra Palacios MS Nath TS. A comparative study of the safety and efficacy between angiotensin-converting enzyme inhibitors and angiotensin receptor blockers on the management of hypertension: a systematic review. Cureus. (2024) 16(2):e 54311. 10.7759/cureus.5431138496070 PMC 10944326 · doi ↗ · pubmed ↗
- 7Kostis JB Packer M Black HR Schmieder R Henry D Levy E. Omapatrilat and enalapril in patients with hypertension: the omapatrilat cardiovascular treatment vs. Enalapril (OCTAVE) trial. Am J Hypertens. (2004) 17(2):103–11. 10.1016/j.amjhyper.2003.09.01414751650 · doi ↗ · pubmed ↗
- 8Maurer M Magerl M. Differences and similarities in the mechanisms and clinical expression of bradykinin-mediated vs. Mast cell-mediated angioedema. Clin Rev Allergy Immunol. (2021) 61(1):40–9. 10.1007/s 12016-021-08841-w 33534062 PMC 8282544 · doi ↗ · pubmed ↗