Pathological and immune features of non-tuberculous mycobacteria and Mycobacterium tuberculosis cutaneous/mucosa infections of fifty-four biopsies
Xiao Ying Zhang, Ying Li, Jing Zhao, Fang Qi Deng, Xu Hua Tang, Jin Fu Li, Wen Ting Yang, Han Wen Jiang, Jin Hua He, Zhuo Wang

TL;DR
This study compares the skin and mucosa infections caused by non-tuberculous mycobacteria and tuberculosis to improve diagnosis and understand their immune responses.
Contribution
The study identifies distinct immune and histopathological features between NTM and MTB infections using macrophage subpopulations and immune markers.
Findings
NTM infections show more small vessel changes and higher lymphocyte counts than TB.
NTM is associated with non-necrotizing granulomas, while TB shows caseous necrotizing granulomas.
Macrophage subpopulations in NTM and TB express different markers like CD68, CD206, and CD163.
Abstract
The histopathologic changes associated with cutaneous non-tuberculous mycobacteria (NTM) infections closely resemble those seen in Mycobacterium tuberculosis (MTB) infections, often leading to confusion. This study aimed to enhance clinicopathologic diagnosis and clarify the pathogenesis of NTM and MTB infections by comparing the clinicopathologic features and immunohistochemistry. We conducted a detailed observation and comparative analysis of histomorphological features in 27 biopsies of cutaneous/mucosa NTM infections and 27 biopsies of MTB infections, focusing on macrophage distribution and the infiltration of various macrophage subpopulations. Our findings revealed that NTM disease was more prone to developing small vessel hyperplasia, dilation, congestion, and interstitial edema compared to tuberculosis (TB). Additionally, the counts of lymphocytes, plasma cells, and neutrophils…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
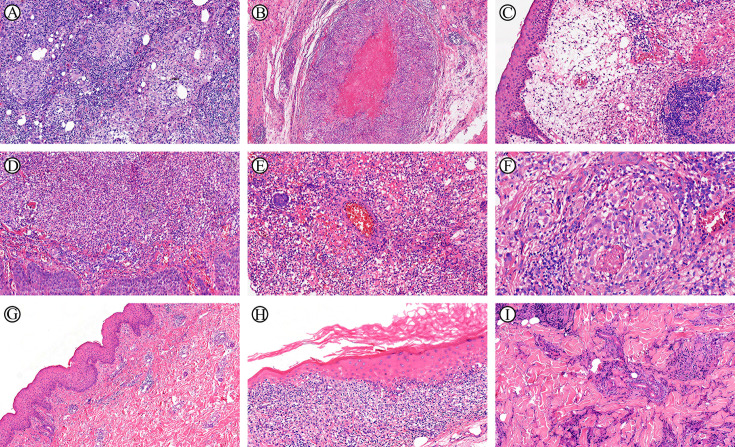 Figure 1
Figure 1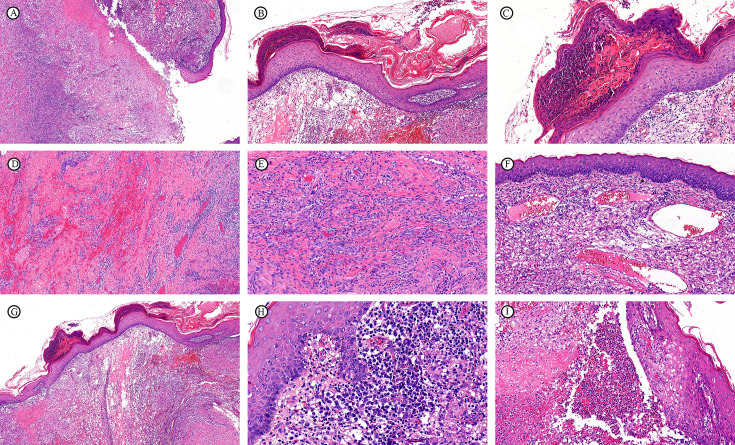 Figure 2
Figure 2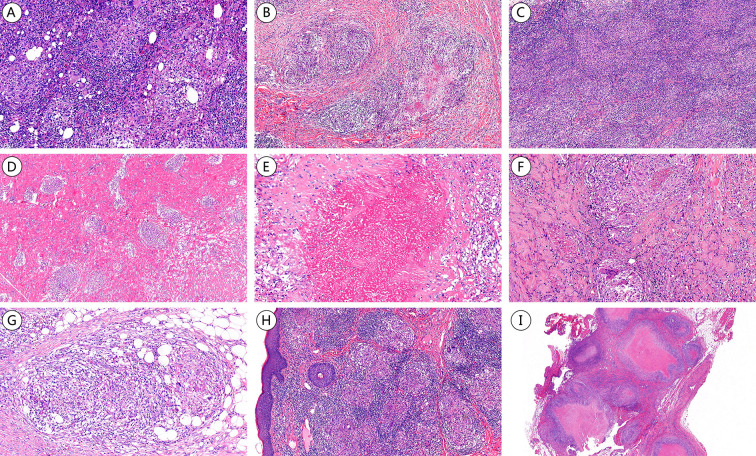 Figure 3
Figure 3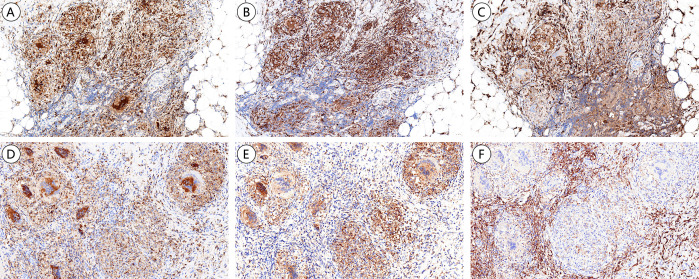 Figure 4
Figure 4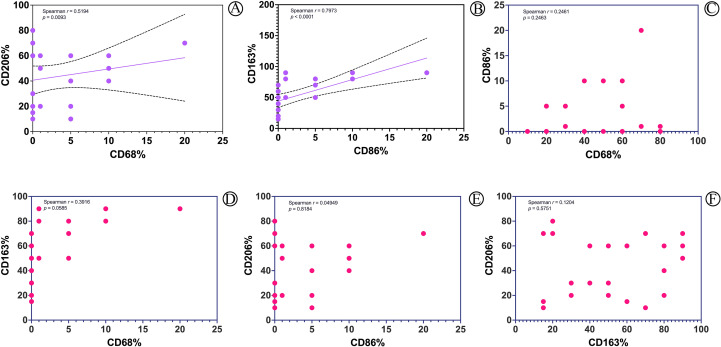 Figure 5
Figure 5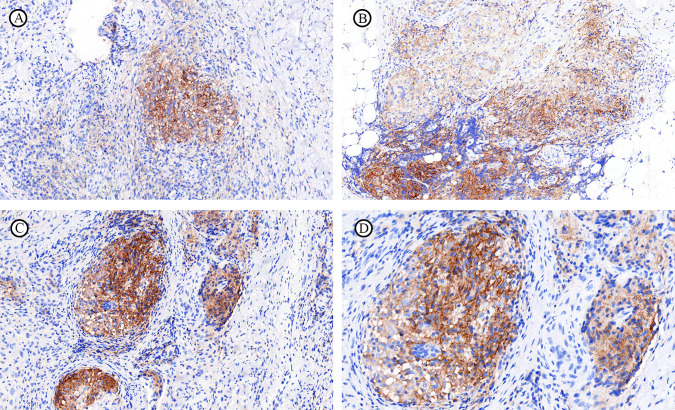 Figure 6
Figure 6| No. of biopsies | NTM subtype | Location | History of seafood exposure | Chronic diseases/tumor | Clinical diagnosis | Immunosuppressive agent |
|---|---|---|---|---|---|---|
| 1 |
| Limb | Yes | None | CNTMD | None |
| 2 |
| Limb | Yes | None | CNTMD | None |
| 3 |
| Limb | No | Diabetes | CNTMD | None |
| 4 |
| Limb | No | None | CNTMD | None |
| 5 |
| UCL | No | None | CNTMD | None |
| 6 |
| UCL | No | None | CNTMD | None |
| 7a |
| Limb | No | None | CNTMD | None |
| 8a |
| Limb | No | None | CNTMD | None |
| 9 |
| Face | No | None | CNTMD | IARAIS |
| 10 |
| Limb | No | None | CNTMD | None |
| 11 |
| Back | No | None | DNTMD | IARAIS |
| 12b |
| Face | No | None | DNTMD | IARAIS |
| 13b |
| Abdomen | No | None | DNTMD | IARAIS |
| 14b |
| Neck | No | None | DNTMD | IARAIS |
| 15 | MAC | Nasal mucosa | No | DILI | DNTMD | None |
| 16c | MAC | Limb | No | None | DNTMD | IARAIS |
| 17c | MAC | UCL | No | None | DNTMD | IARAIS |
| 18c | MAC | UCL | No | None | DNTMD | IARAIS |
| 19d | MAC | UCL | No | None | CNTMD | IARAIS |
| 20 |
| Limb | Yes | None | CNTMD | None |
| 21e |
| Back | No | Lymphoma | DNTMD | None |
| 22e |
| Abdomen | No | Lymphoma | DNTMD | None |
| 23 |
| Nasal mucosa | No | None | CNTMD | None |
| 24 |
| Limb | No | None | CNTMD | None |
| 25 |
| Face | No | None | DNTMD | IARAIS |
| 26 |
| Limb | No | Castleman Diseases | CNTMD | None |
| 27d |
| Face | No | None | CNTMD | IARAIS |
| Pathological feature | NTMD number of positive case/number of biopsies tested (percentage positive) | TB number of positive case/number of biopsies tested (percentage positive) | Adj. |
|---|---|---|---|
| Epidermal hyperplasia | 16/21(76.2%) | 10/17(58.8%) | 0.738 |
| Ulceration | 6/21(28.6%) | 6/17(35.3%) | 0.897 |
| Hyperkeratosis/Parakeratosis | 14/21(66.7%) | 9/17(52.9%) | 0.873 |
| Granulocytic exudates | 10/23(43.5%) | 6/17(35.3%) | 0.897 |
| Plasma exudates | 3/23(13.0%) | 3/17(17.7%) | 1.000 |
| Spongy edema | 5/23(21.7%) | 1/17(5.9%) | 0.647 |
| Appendage destruction | 19/27(70.4%) | 12/17(70.6%) | 1.000 |
| Hemorrhage | 14/27(51.9%) | 11/27(40.7%) | 0.879 |
| Microvessels hyperplasia | 20/27(74.1%) | 12/27(44.4%) | 0.309 |
| Microvessels dilation and congestion | 18/27(66.7%) | 9/27(33.3%) | 0.309 |
| Interstitial edema | 19/27(70.4%) | 13/27(48.2%) | 0.647 |
| Vasculitis | 0/27(0%) | 2/27(7.4%) | 0.873 |
| Immune cell | NTMD (n=27) number of positive case/number of biopsies tested (percentage positive) | TB (n=27) number of positive case/number of biopsies tested (percentage positive) | Adj. | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 Grade | 1 Grade | 2 Grade | 3 Grade | 0 Grade | 1 Grade | 2 Grade | 3 Grade | ||
| Lymphocytes | 0(0.0%) | 7(25.9%) | 14 (51.9%) | 6 (22.2%) | 0 (0.0%) | 20 (74.1%) | 7 (25.9%) | 0 (0.0%) | 0.002 |
| Plasma Cells | 1(3.7%) | 18(66.7%) | 5 (18.5%) | 3 (11.1%) | 9 (33.3%) | 16 (59.3%) | 2 (7.4%) | 0 (0.0%) | 0.013 |
| Eosinophils | 17(63.0%) | 7(25.9%) | 3 (11.1%) | 0(0.0%) | 15 (55.6%) | 12 (44.4%) | 0 (0.0%) | 0 (0.0%) | 0.154 |
| Neutrophils | 0(0.0%) | 14(51.9%) | 9 (33.3%) | 4 (14.8%) | 8 (29.6%) | 15 (55.6%) | 3 (11.1%) | 1 (3.7%) | 0.008 |
| Histiocytes | 0(0.0%) | 14(51.9%) | 8(29.6%) | 5(18.5%) | 0(0.0%) | 5(18.5%) | 20(74.1%) | 2(7.4%) | 0.009 |
| MGC | 9(33.3%) | 12(44.4%) | 5 (18.5%) | 1 (3.7%) | 3 (11.1%) | 19 (70.3%) | 3 (11.1%) | 2 (7.4%) | 0.154 |
- —National Natural Science Foundation of China 10.13039/501100001809
- —Traditional Chinese Medicine Bureau of Guangdong Province 10.13039/501100010883
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Mycology · Tuberculosis Research and Epidemiology
Introduction
1
The term non-tuberculous mycobacteria (NTM) refers to a diverse group of mycobacteria distinct from the “Mycobacterium tuberculosis complex” and “Mycobacterium leprae.” Previously, this group included terms like “atypical mycobacteria” and “atypical acid-resistant mycobacteria.” To date, more than –266 NTM species and 14 subspecies have been identified, most of which are commensal bacteria, with only a few being pathogenic to humans under certain conditions (Smith et al., 2016; Yoon et al., 2017; Santin et al., 2018; Furuuchi et al., 2019; Winthrop et al., 2020; Yazdanmanesh et al., 2024). Tuberculosis (TB), caused by Mycobacterium tuberculosis (MTB), exhibits similar histopathological changes to those seen in NTM infections, leading to potential diagnostic confusion. However, significant differences exist in clinical treatment and prognosis, making accurate pathological diagnosis crucial for guiding clinical management.
Macrophages can be broadly classified into two categories: M1 and M2, based on their inflammatory roles. Classically activated macrophages (M1) are induced by lipopolysaccharide (LPS) and interferon-γ (IFN-γ) (Dolezalova et al., 2022), playing a critical role in anti-infective responses during the early stages of the disease. Conversely, alternatively activated macrophages (M2), stimulated by IL-4 or IL-13, are significant in chronic disease progression and fibrosis. NTM and MTB can exist not only intracellularly but also extracellularly, and they can survive phagocytosis, and macrophages are essential in inhibiting and killing these pathogens. However, the distinct roles of M1 and M2 macrophages in this context remain unclear.
To investigate these differences, we conducted comprehensive histomorphological examinations of 27 biopsies of cutaneous/mucosa NTMD and 27 biopsies of TB. While both NTMD and TB were primarily present as granulomatous lesions and non-specific chronic suppurative inflammation, distinct pathomorphological differences were identified in the epidermis, dermis, and subcutaneous adipose tissue. Our analysis focused on macrophage infiltration and differences in PD-L1 (programmed death ligand 1) expression in immune cells.
Materials and methods
2
Case selection and clinicopathologic evaluation
2.1
We analyzed 27 biopsies of cutaneous/mucous NTMD and 27 biopsies of TB diagnosed between December 2, 2013 and May 17, 2023. 26 biopsies of cutaneous NTMD and 26 biopsies of TB were from the First Affiliated Hospital of Sun Yat-sen University, 1 biopsy of cutaneous NTMD and 1 biopsy of TB were from the Affiliated Panyu Central Hospital of Guangzhou Medical University. The inclusion criteria comprised cases of cutaneous/mucous NTMD and TB. The diagnosis was based on clinical presentation, imaging, pathogenesis, pathological examination, metagenomics next-generation sequencing (mNGS), and tuberculosis polymerase chain reaction (TB-PCR) testing (Sardiña et al., 2020; Epperson et al., 2024). Cutaneous/mucous tissue, cutaneous pus, blood, and bronchoalveolar lavage fluid (BALF) were collected for acid-fast bacilli (AFB) culture, mNGS, and TB-PCR testing. mNGS was used as a high-resolution reference method, mNGS plays a critical role in the identification and diagnosis of infectious diseases. However, mNGS still presents several limitations, such as FFPE contamination, detection threshold, and semiquantitative interpretation challenges (Appak et al., 2018; Huang et al., 2019; Zhou et al., 2019; Dulanto Chiang and Dekker, 2020; Qian et al., 2020). In this cohort, all 27 biopsies of NTMD were diagnosed by mNGS, among which 12 biopsies underwent AFB culture, with a positive rate of approximately 58.3% (7/12). All 27 biopsies of tuberculosis (TB) were confirmed by mNGS and TB-PCR, among which 10 biopsies underwent AFB culture, with a positive rate of approximately 60.0% (6/10).
Specimens were fixed in 4% neutral formaldehyde, routinely dehydrated, clarified, paraffin-embedded, and cut into 3 μm thick sections. These sections were stained with hematoxylin and eosin (HE) and subjected to acid-fast staining. Two dermatopathologists with subspecialty expertise conducted independent morphological analyses to assess differences between the groups.
Immunohistochemistry
2.2
Immunohistochemical staining was performed on 4 μm sections cut from formalin-fixed, paraffin-embedded tissue using an automated immunostainer. The primary monoclonal antibodies used included CD68 (1:100, mouse monoclonal, clone KP1, catalog No. ZM-0060; OriGene), CD86 (1:100, rabbit monoclonal, clone E2G8P; Cell Signaling), CD163 (RTU, mouse monoclonal, clone 10D6, catalog No. ZM-0428; OriGene), CD206 (1:1000, rabbit monoclonal, catalog No. 18704-1-AP; Proteintech), and PD-L1 (1:50, mouse monoclonal, clone 22C3, catalog No. M3653; Dako). The cells were counted manually by two individuals (X-Y Z and Z W). In cases of discrepancies between the two evaluators, the slides were re-examined and recounted to reach a consensus.
The percentage of positive macrophages was calculated for CD68, CD86, CD163, and CD206, based on the total number of macrophages. PD-L1 expression was assessed by counting PD-L1 stained cells (lymphocytes and macrophages/histiocytes) relative to the total number of live mononuclear inflammatory cells, expressed as a percentage. Membrane staining intensity was considered PD-L1 expression, including in multinucleated giant cells. In PD-L1 assessment, there is currently no standardized criteria for inflammatory lesions. Therefore, we adopted the ≥10% cut-off in immune cells based on the study by Selma Emre (Emre et al., 2023). Samples were categorized into low PD-L1(+) (less than 10% positivity) and high PD-L1(+) (10% or greater positivity) groups.
Metagenomic next-generation sequencing and analysis
2.3
When selecting body fluids or fresh tissue from the infection site for mNGS testing, strict aseptic techniques must be followed during the collection of sterile body fluid/tissue samples to avoid false positives caused by environmental mycobacterial contamination. Samples were aseptically sealed and stored at −20 °C or transported on dry ice to the molecular laboratory for mNGS detection. The samples underwent grinding and cell wall disruption procedures followed by host DNA depletion. Upon completion of pre-processing, nucleic acid extraction was performed using magnetic bead-based methods. RNA and DNA libraries constructed from patient-derived samples were sequenced on an Illumina HiSeq platform in rapid-run mode, achieving a depth of 5 to 10 million single-end reads, each 140 base pairs in length. The raw sequencing data were quality-controlled using fastp (v0.23.2), which included adapter trimming, low-quality read filtering, low-complexity sequence removal, and elimination of excessively short reads. A human reference database was constructed based on GRCh38.p13 and the NCBI nt database to identify and remove human-derived sequences through alignment with bowtie2 (v2.3.5.1). A pathogen database was built using the NCBI RefSeq database (v20221231), FDA-ARGOS v1.0, the Genome Taxonomy Database release 206, and the NCBI GenBank database (v20221231). Non-human sequences were aligned to the pathogen database using the Burrows-Wheeler Aligner (BWA, v0.7.17-r1198-dirty). Contaminating sequences were filtered using a laboratory background database, followed by taxonomic classification and statistical analysis (in-house script) to obtain species-specific read counts, relative abundance, and genome coverage. All detected read counts were normalized to 20 M reads. For specific pathogens such as NTM and MTB, the detection of one unique species-specific read was considered positive (Naccache et al., 2014; Schlaberg et al., 2017; Han et al., 2022).
Polymerase chain reaction
2.4
Paraffin-embedded tissues were sectioned at 5 μm thickness, and DNA was extracted using the Paraffin-Embedded Tissue Genomic DNA Extraction Kit (Qiagen). The concentration and purity of extracted DNA were assessed by UV spectrophotometry. Subsequently, samples underwent an MTB assay according to the instructions of the Mycobacterium tuberculosis DNA fluorescence diagnostic kit (PCR-fluorescence probing, Sansure Biotech Inc.). Positive and negative controls were established to ensure the accuracy and reliability of results (Choi et al., 2012; Lim et al., 2019; Sawatpanich et al., 2022).
Statistical analyses
2.5
Statistical analysis was performed using SPSS 27.0 software. Categorical variables were presented as frequencies and percentages. The Fisher’s exact test was used to compare pathological features, immune cell infiltration, granuloma types, and PD-L1 expression on immune cells. P-values were adjusted for multiple testing using the Benjamini-Hochberg (BH) method, with a significance threshold set at P < 0.05. The correlations among the positive rates of macrophage markers (CD68, CD86, CD163, and CD206) were analyzed as follows. The Shapiro-Wilk test (prioritized for sample sizes n ≤ 50) was used to assess normality. Variables with p > 0.05 were considered normally distributed, and Pearson correlation coefficients were calculated. For variables failing to meet the normality criterion (p ≤ 0.05), nonparametric Spearman correlation was employed. Correlation strength was quantified using R-values ranging from –1 to 1, where values closer to ±1 denote a stronger linear association between variables. A p-value less than 0.05 was considered statistically significant.
Results
3
Clinical findings
3.1
A total of 27 biopsies of NTMD were analyzed, with cutaneous/mucosal biopsy specimens obtained from each case (Table 1). The biopsies included 8 of M. marinum, 6 of M. abscessus, 5 of the M. avium-intracellulare complex (MAC), 3 of M. haemophilum, 3 of M. avium, 1 of M. colombiense, and 1 of M. mantenii. Specimens were collected from various sites: 11 from the limbs, 4 from the face, 2 from the back, 2 from the abdomen, 1 from the neck, 5 from unspecified cutaneous locations, and 2 from the nasal mucosa.
The 27 biopsies represented 20 patients with an average age range of 41–72 years (mean age 57.9, median age 59). Most patients were middle-aged or elderly, with a male-to-female ratio of 1:1. Five patients had multiple biopsies from different sites either concurrently or at different times. One patient had successive infections with two NTM species: initially with M. avium-intracellulare complex in 2020, which was clinically resolved, followed by M. mantenii in 2022.
Among the 20 patients, 6 had disseminated NTMD, all of whom had compromised or deficient immune function, including 4 with adult anti-IFN-γ autoantibody-related immunodeficiency syndrome, one with a history of lymphoma, and one with drug-induced liver damage. Among the 14 biopsies of NTM cutaneous infections, 2 had adult anti-IFN-γ autoantibody-associated immunodeficiency syndrome, and one had diabetes. All 6 patients with anti-IFN-γ syndrome received prednisone for anti-inflammatory treatment, and pathological biopsies were performed prior to the initiation of therapy. The NTMD lesions were primarily painless papules, nodules, or plaques, some merging into larger lesions that exhibited bleeding, crusting, and scarring in chronic cases. A few patients had co-infections with human herpesvirus type 4, human herpesvirus type 5, fine cyclic virus, Pseudomonas aeruginosa, and Candida albicans.
For tuberculosis (TB), 27 cutaneous/mucosal biopsy specimens were obtained from 24 patients, with ages ranging from 8 to 83 years (mean age 40.8, median age 36). This group displayed a wide age distribution, from children to the elderly, also with a male-to-female ratio of 1:1. Three patients underwent cutaneous biopsies from different sites simultaneously. The biopsies from patients with cutaneous manifestations of tuberculosis were collected from the limbs (12), neck (4), chest (2), buttocks (2) and face (1), as well as from other sites including facial cutaneous, the vocal cords, the floor of the mouth, nasal mucosa, and the inner canthus of the eye. The TB cutaneous lesions typically appeared as plaques or nodules, dark red in color, and were often accompanied by desquamation, vesiculobullous eruptions, oozing, ulceration, and crusting.
Pathological morphological analysis of NTMD and TB
3.2
A comparative analysis of the pathomorphological characteristics of the epidermis, dermis, and subcutaneous adipose tissue was conducted (Supplemental Digital Content Supplementary Figure S1, which demonstrates gross pathological morphological features of NTMD and TB), focusing on subtle features (Figures 1, 2). Epidermal characteristics included hyperplasia, ulceration, parakeratosis/hyperkeratosis, granulocytic exudates, plasma exudates, and spongy edema. Dermal and subcutaneous features included interstitial edema, hemorrhage, microvessels hyperplasia, microvessels dilation and congestion, vasculitis, necrosis, and destruction of appendages. Four NTMD biopsies and eight TB biopsies exhibited loss of the epidermis due to ulceration or crusting, while two NTMD biopsies and two TB biopsies from nasal mucosa. Consequently, fewer biopsies were available for evaluation of epidermal-related features. A comparison of the features revealed that NTMD exhibited more microvessels hyperplasia, dilation, congestion, and interstitial edema than TB, although these differences did not reach statistical significance (Table 2). Pseudoepitheliomatous hyperplasia was observed in NTMD (3/27, 11.1%) and TB (2/27, 7.4%), with no significant difference. Epidermal hyperplasia and ulceration were present in both NTMD and TB biopsies, as were parakeratosis/hyperkeratosis, granulocytic exudation, plasma exudation, spongiotic edema, hemorrhage, vasculitis, and destruction of appendages, with no significant differences noted.
NTMD pathomorphological characterization of diverse bacterial strains (H&E staining). (A) M. marinum, organized granulomas (300-500 μm). (B) M. marinum, granulomas with central fibrinous necrosis. (C) M. marinum, interstitial edema. (D) M. abscessus, aggregation of neutrophils and microabscess. (E) M. abscessus, intravascular neutrophilic infiltration. (F) M. abscessus, histiocytes containing faintly basophilic granules and filamentous cellular debris. (G) MAC, sparse inflammatory cell infiltration. (H) M.haemophilum, interface dermatitis. (I) M. avium, prominent, coarse collagen proliferation.
Pathological morphological features of TB (H&E staining). (A) Cutaneous ulcers. (B) Hyperkeratosis and parakeratosis of the epidermis with serous exudate. (C) Munro microabscesses. (D) Interstitial hemorrhage. (E) Proliferation of microvessels. (F) Dilation and congestion of microvessels. (G) Moderate interstitial edema. (H) Patchy infiltration of plasma cells. (I) Microabscess.
NTMD pathomorphological characterization of diverse bacterial strains
3.3
A comparison of the pathomorphological features of NTMD from seven different strains revealed distinct findings (Figure 1, Supplemental Digital Content Supplementary Table S2, which demonstrates NTMD pathomorphological characterization of diverse bacterial strains): (i) M. marinum exhibited two distinct histopathological patterns: The first was characterized by well-formed granulomas (300 -500 μm) composed of abundant epithelioid cells, often with central fibrinous necrosis. The second pattern featured marked interstitial edema, hemorrhage, and loosely distributed epithelioid cells without distinct nodular formation, accompanied by peripheral granulation tissue proliferation. (ii) M. abscessus infection consistently demonstrated neutrophilic infiltration. In severe cases, aggregates of neutrophils within newly formed blood vessels were observed. A distinctive feature was the presence of foamy histiocytes with abundant pale cytoplasm, these foamy histiocytes exhibit the distinctive feature of containing faintly basophilic granules and filamentous cellular debris within their cytoplasm. (iii) MAC infection typically demonstrate relatively sparse inflammatory cell infiltration. Histopathological examination reveals only mild neutrophilic infiltration. (iv) A distinctive histopathological feature of M.haemophilum infection is the presence of interface dermatitis. (v) M. avium infection is characterized by prominent, coarse collagen proliferation, resulting in characteristic keloid-like fibrosis. (vi) M. colombiense demonstrated focal interstitial edema, loosely arranged epithelioid cells, hemorrhage, granulation tissue proliferation, and granular necrosis. (vii) M.mantenii presented with small clusters of epithelioid cells (100 μm), diffuse neutrophilic infiltration without distinct abscess formation, and minimal intravascular neutrophil aggregation.
Immune cell infiltration in NTMD and TB
3.4
Both NTMD and TB primarily present with granulomatous lesions and nonspecific chronic suppurative inflammation. Immune cell types present include lymphocytes, plasma cells, eosinophils, neutrophils, histiocytes, and multinucleated giant cells. Immune cell infiltration was graded on a scale of 0 to 3, where grade 0 indicates absence, grade 1 denotes focal or scattered infiltration, grade 2 signifies multifocal aggregates and grade 3 indicates small patchy or diffuse infiltration. The histopathological grading of neutrophilic infiltration is categorized as: grade 1 indicates neutrophils are sparsely distributed with low cellular density, grade 2 indicates moderate neutrophil density with formation of small neutrophil foci, grade 3 indicates dense, confluent neutrophilic infiltration with microabscess or abscess formation. A comparative analysis revealed significant differences in the infiltration of lymphocytes, plasma cells, neutrophils, and histiocytes between NTMD and TB, with no significant differences in eosinophils or multinucleated giant cell distribution (Table 3). The number of lymphocytes, plasma cells, and neutrophils was significantly higher in NTMD compared to TB. Neutrophil infiltration was observed in all NTMD biopsies, mostly in small focal distributions (grade 1, 14/27, 51.85%). A few neutrophilic microabscesses (grade 3) were seen in 4 biopsies (4/27, 14.8%), while neutrophils were absent in 29.63% of TB biopsies. Only one case of TB exhibited neutrophilic microabscesses (grade 3). In addition to forming granulomas as epithelioid cells, histiocytes in NTM biopsies could also be seen as foamy histiocytes scattered or patchily distributed in the dermis and subcutaneous tissue (excluding the ulcerated granulation tissue), predominantly in focal distributions (grade 1, 14/27, 51.85%). In TB biopsies, histiocytes were mainly involved in granuloma formation as epithelioid cells, with only a few biopsies (5/27, 18.52%) showing scattered or patchily distributed foamy histiocytes (grade 1) in the stroma (excluding ulcerated granulation tissue).
Granuloma formation in NTMD and TB
3.5
Granulomatous lesions can be classified as necrotizing or non-necrotizing, based on necrosis presence. Necrotizing granulomas are further categorized into caseous, coagulative, and pyogenic necrosis. NTMD presented with granulomas in 19 of 27 biopsies (70.4%), while TB exhibited granulomas in 26 of 27 biopsies (96.3%), indicating a significantly higher frequency in TB(Supplemental Digital Content Supplementary Table S1, which demonstrates comparison of granuloma types between NTMD and TB). Both NTMD and TB can have non-necrotizing or necrotizing granulomas; however, NTMD predominantly exhibited non-necrotizing granulomas (11/27, 40.7%) (Figures 3A–G), whereas TB predominantly showed caseous necrotizing granulomas (12/27, 44.4%) (Figures 3H, I), with NTMD presenting caseous necrotizing granulomas in 14.8% (4/27). Statistically significant differences were found in both the proportion and classification of granulomas between NTMD and TB.
Compares the granuloma morphologies in NTMD and TB (H&E staining). (A) M. marinum, multiple small non-necrotizing granulomas. (B) M. abscessus, necrotizing and non-necrotizing granulomas. (C) MAC, multiple non-necrotizing granulomas in the nasopharynx (case 15). (D) M. haemophilum, multiple non-necrotizing granulomas. (E) M. haemophilum, caseous necrotizing granulomas with thorough necrosis, complete disappearance of cellular outlines and structures, appearing as homogeneous eosinophilic granular material. (F) M. avium, necrotizing and non-necrotizing granulomas. (G) M. colombiense, non-necrotizing granulomas. (H) M. tuberculosis, multiple non-necrotizing granulomas. (I) M. tuberculosis, caseous necrotizing granulomas.
Analysis of macrophage subsets in NTMD and TB
3.6
CD68 is a pan-macrophage marker, M1-type macrophages is marked by the surface marker CD86, while M2-type macrophages are characterized by CD163 and CD206. Macrophages were found distributed in the interstitium, present as scattered histiocytes and granuloma epithelioid macrophages. The mean positivity of macrophages for CD68, CD86, CD163, and CD206 in NTMD was 42.5%, 3.0%, 55.4%, and 43.3%, respectively. In TB, the positivity rates were 41.7%, 2.7%, 44.2%, and 39.0%. Both NTMD and TB exhibited high expression of CD68, CD163, and CD206, with CD163 being the most prominently expressed marker. CD86 was either negative or weakly positive (less than 5% positivity).
In NTMD and TB, CD68 and CD206 were primarily expressed by granuloma epithelioid macrophages, while CD163 was expressed by interstitial scattered macrophages (Figure 4). A positive correlation was noted between CD68 and CD206 positivity, as well as between CD86 and CD163 in NTMD, reaching statistical significance (Figure 5). No significant correlations were found in TB macrophages (Supplemental Digital Content Supplementary Figure S2, which demonstrates statistical analysis of the correlation between the positive rates of CD68, CD86, CD163, and CD206 in macrophages in TB).
Immunohistochemical expression of different macrophage subsets in NTMD and TB. (A–C) M. avium. (A) CD68 highlights expression primarily in granuloma epithelioid macrophage. (B) CD206 expression mainly in granuloma epithelioid macrophage. (C) CD163 expression predominantly in interstitial scattered macrophages. (D–F) MTB, (D) CD68 highlights expression primarily in granuloma epithelioid macrophage. (E) CD206 expression mainly in granuloma epithelioid macrophage. (F) CD163 expression is mainly in interstitial scattered macrophages.
Statistical analysis of the correlation between the positive rates of CD68, CD86, CD163, and CD206 in macrophages in NTMD. (A) Significant correlation between CD68 and CD206. (B) Significant correlation between CD86 and CD163. (C–F) No statistical significance correlations between CD68 and CD86, CD68 and CD163, CD86 and CD206, CD163 and CD206.
Analysis of PD-L1 expression of immune cells in NTMD and TB
3.7
In both NTMD and TB, PD-L1 was expressed by granuloma epithelial cells, lymphocytes, and multinucleated giant cells. Granuloma epithelial cells predominantly expressed PD-L1, whereas lymphocytes and multinucleated giant cells showed low or absent PD-L1 expression (Figure 6). In NTMD, mononuclear inflammatory cells exhibited a PD-L1 positivity rate of 0% to 40%, with a mean positivity of 6.4%, which was higher in biopsies of M. avium and M. marinum. In TB, PD-L1 positivity ranged from 0% to 60% in mononuclear inflammatory cells, with a mean positivity of 14.3%. A higher percentage of mononuclear inflammatory cells in TB (45.8%) demonstrated high PD-L1 expression (≥10%) compared to NTMD (25%), though no significant difference was noted between the two groups (Supplemental Digital Content Supplementary Table S3, which demonstrates PD-L1 expression of immune cells in NTMD and TB).
Immunohistochemical PD-L1 expression in NTMD and TB. (A) M. marinum, granuloma epithelioid macrophage positive for PD-L1. (B) M. avium, granuloma epithelioid macrophage and mononuclear inflammatory cells positive for PD-L1. (C, D) MTB, granuloma epithelioid macrophage positive for PD-L1.
Discussion
4
The species identified in 27 biopsies of cutaneous NTMD included M. marinum, M. abscessus, MAC, M. haemophilum, M. avium, M. colombiense, and M. mantenii, with M. marinum, M. abscessus, and MAC being the most commonly identified Mycobacterium species. Notably, local abscesses of cutaneous and soft tissue are mainly attributed to M. abscessus, typically occurring at sites of needle puncture wounds, open injuries, or fractures (Fowler and Mahlen, 2014; Philips et al., 2019), while infections from M. marinum and M. haemophilum are linked to contact with seafood (Hsueh et al., 2019; Mei et al., 2019). Disseminated NTMD is primarily observed in immunocompromised individuals, particularly those with HIV or other forms of immunodeficiency. Symptoms include persistent or intermittent fever, weight loss, night sweats, and gastrointestinal issues (Nithirungruang et al., 2024; Park et al., 2024). In our cohort, M. abscessus, M. haemophilum, and MAC were implicated in systemic disseminated NTMD, with 6 of 20 patients being immunocompromised.
The histopathological features of cutaneous NTMD are under-reported in literature (Heid-Picard et al., 2024; Yao et al., 2024). While NTM shares similarities with MTB in bacterial composition and antigens, they are generally less virulent, leading to a milder tissue response and less severe lesions (Nguyen et al., 2024). Main pathological features in NTMD include granulomatous lesions and non-specific chronic suppurative inflammation. The pathological changes generally include: Exudative reactions dominated by lymphocytes, histiocytes, and neutrophils; Proliferative reactions consisting of granulomas formed by macrophages and Langerhans giant cells, sometimes with caseous or coagulative necrosis; Sclerotic reactions involving the regression of inflammatory cells, granuloma atrophy, and collagen fiber proliferation (Nguyen et al., 2024).
NTM species are diverse, and the histopathological changes in various types of infections are not entirely consistent: (i) M. marinum infection demonstrated biphasic histologic manifestations, type I (granuloma-predominant) organized epithelioid granulomas with central fibrinoid necrosis, and type II (edema-predominant) a diffuse edematous pattern exhibiting hemorrhagic stroma without discrete granuloma formation. These distinct histopathological patterns likely reflect the host immune response to infection, mirroring the immune spectrum seen in tuberculosis. When host immunity is relatively robust and bacterial burden is low, the predominant pathological manifestation is small, well-formed granulomas. Conversely, in immunocompromised states with high mycobacterial load and enhanced pathogenicity, the pathology shifts toward marked tissue edema with scattered epithelioid cells. Notably, both patterns may coexist within the same lesion, with one predominating and potential interconversion between them. Case 5 exhibited both pathological patterns simultaneously. (ii) M. abscessus infection reveals neutrophil-dominated inflammation, Bayer-Garner (Bayer-Garner et al., 2005) suggests that M. abscessus exploits neutrophil-rich settings to promote its survival. the foamy histiocytes characterized by their voluminous pale cytoplasm containing distinctive intracytoplasmic inclusions of faintly basophilic granules and filamentous degenerative debris. This unique feature, representing intracellular phagocytosed bacterial and degenerated cellular debris, serves as a diagnostic hallmark for M. abscessus. (iii) MAC characteristically shows diminished inflammatory cell infiltration compared to other NTM infections. This observation may suggest that MAC exhibits relatively weaker pathogenicity and elicits a milder host inflammatory response. (iv) M.haemophilum infection is characterized by interface dermatitis, a diagnostic morphological feature that demonstrates remarkable specificity when differentiating from other NTM species. Busam (Busam et al., 1999) reveal that infection by M. haemophilum can present with nongranulomatous or pauci-granulomatous reactions without necrosis is of note, one biopsy showed an interface dermatitis. (v) M. avium infection demonstrates distinctive stromal changes featuring thickened, hyalinized collagen bundles that progress to form pathognomonic keloid-type fibrotic lesions.
Macrophages are the most important cell type in the innate immune response against both NTM and MTB, playing a crucial role throughout the infection process, including establishment, progression, and dissemination. Macrophages can be classified into classically activated M1 type (CAM) and alternatively activated M2 type (AAM) (Lee and Sacks, 2024). M1 macrophages are mainly involved in inflammatory responses and mediating tissue damage, with common surface marker CD86. M2 macrophages can downregulate immune responses, suppress inflammation, and promote tissue repair and remodeling (Zhang et al., 2024), with common surface markers including CD163 and CD206. Additionally, macrophages can regulate their own polarization through autocrine and paracrine signaling, allowing the conversion between M1 and M2 types and utilizing this plasticity to balance the immune microenvironment (Jiang et al., 2024; Luo et al., 2024; Salmaninejad et al., 2024). In our study, both NTMD and TB granulomas highly express CD68 and CD206 (M2 type macrophages), and the scattered macrophages highly express CD163 (M2 type macrophages), indicating involvement in chronic inflammation. The location of CD163 and CD206 expressing macrophages differs: CD163 expressing macrophages are mainly found in non-granuloma regions, while CD206 expressing macrophages are predominantly in the granulomas. There is no significant correlation between their positivity rates. The differing localization of CD163 and CD206 expressing macrophages suggests that these M2 macrophage subsets belong to different subpopulations with distinct functional roles. CD206+ macrophages may be involved in the intracellular growth of the pathogen, while CD163+ macrophages may be involved in immune response modulation. Both NTM and TB macrophages show almost no expression of CD86, with only a few biopsies showing focal weak positivity, possibly due to the lower sensitivity of the CD86 antibody.
Correlation analysis of positivity rates for CD68, CD86, CD163, and CD206 reveals a significant correlation between CD68 and CD206 in NTMD, primarily expressed in granulomas. Although CD86 is expressed at low levels in non-granuloma region macrophages, this study revealed a significant correlation between CD86 and CD163. No statistical significance is found in TB, suggesting that in NTMD, CD68+CD206+ and CD86+CD163+ may represent more independent macrophage subpopulations that warrant further to exploring their potential roles in the pathogenesis of NTMD. NTM and MTB are successful intracellular pathogens that are mainly harbored in macrophages of the host. Although macrophages have several antimicrobial mechanisms to eliminate the intracellular bacteria, NTM and MTB can survive and multiply within them by adjusting and adapting to host immune responses (Mi et al., 2017). PE/PPE family proteins are primarily found in pathogenic mycobacteria species and they are usually expressed during infection and secreted or exposed to the cell surface. All these factors imply that PE/PPE proteins play a critical role in mycobacterial pathogenicity (Fishbein et al., 2015). A crucial factor in MTB’s virulence is the ESX-5 secretion system, which plays an essential role in the transport of PE/PPE proteins, cell wall integrity, and full virulence of MTB (Bottai et al., 2012; Ehtram et al., 2025). The ESX-5 secretion system and PE/PPE proteins collectively facilitate immune evasion and promote intracellular persistence within macrophages.
PD-1 is an inhibitory receptor predominantly expressed on T lymphocytes, which plays a critical role in regulating autoimmunity and self-tolerance. PD-1 is a transmembrane protein expressed on the cell membrane of T cells, B cells, and other immune cells, as well as on tumor cells. PD-L1 immunohistochemistry is a simple and effective method for predicting the efficacy of PD-L1 inhibitors. This technique involves assessing the expression levels of PD-L1 on the surface of tumor cells (TC) or immune cells (IC) to estimate the potential effectiveness of PD-L1 inhibitors. Selma Emre (Emre et al., 2023) investigated the expression of PD-1/PD-L molecules in the lesioned skins of psoriasis patients. the PD-1 and PD-L1 expressions were significantly higher in immune cells than that in the skin samples of the healthy controls. In our experiments, we compared PD-L1 expression in NTMD and TB biopsies by assessing the positivity rate in immune cells. Granuloma epithelioid macrophages, lymphocytes, and multinucleated giant cells can express PD-L1, primarily in granuloma epithelioid macrophages. Non-necrotizing granulomas and necrotizing granulomas both expressed PD-L1, but non-necrotizing granulomas showed stronger expression. 70.8% of NTMD immune cells had a PD-L1 positive rate greater than 1%, with an average positive rate of 6.4%, and higher positive rates were observed in M. avium and M. marinum. 87.5% of TB immune cells had a PD-L1 positive rate greater than 1%, with an average positive rate of 14.3%. 25% of NTMD immune cells showed high PD-L1 expression (≥10%), and 45.8% of TB immune cells showed high PD-L1 expression. Although there was no significant difference between the two groups, the expression levels still reflected the characteristic that the immune cells’ response in TB is somewhat stronger than in NTMD. NTMD complicated by anti-IFN-γ autoantibody-associated immunodeficiency syndrome immune cells showed low or absent PD-L1 expression. Immunosuppressed patients demonstrated reduced PD-L1 expression on immune cells, although the relationship between PD-L1 expression and immunosuppression remains unclear.
Conclusion
5
This study highlights the distinct histopathological features of NTMD compared to TB, NTMD shows higher prevalence of small vessel changes (hyperplasia/dilation/congestion), interstitial edema, and elevated counts of lymphocytes, plasma cells, and neutrophils. The histopathological features of cutaneous NTM infections show distinct patterns: M. marinum demonstrates marked interstitial edema, M. abscessus exhibits prominent neutrophilic infiltration, M. avium infection is characterized by prominent, coarse collagen proliferation, and M. haemophilum presents interface dermatitis. NTMD is characterized by non-necrotizing granulomas, while TB features necrotizing granulomas. The granulomas within NTMD predominantly express CD68 and CD206, contrasting with the CD163 expression found in non-granulomatous areas, indicating distinct subpopulations with different roles.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1AppakÖTürkel S.Esen N.Özkütük A. A. (2018). Comparison of polymerase chain reaction-restriction enzyme analysis method and DNA sequence analysis results in the identification of non-tuberculous mycobacteria. Acta Microbiol. Immunol. Hung. 65, 515–527. doi: 10.1556/030.65.2018.027, PMID: 30010392 · doi ↗ · pubmed ↗
- 2Bayer-Garner I. B.Cox M. D.Scott M. A.Smoller B. R. (2005). Mycobacteria other than Mycobacterium tuberculosis are not present in erythema induratum/nodular vasculitis: a case series and literature review of the clinical and histologic findings. J. Cutan Pathol. 32, 220–226. doi: 10.1111/j.0303-6987.2005.00296.x, PMID: 15701084 · doi ↗ · pubmed ↗
- 3Bottai D.Di Luca M.Majlessi L.Frigui W.Simeone R.Sayes F.. (2012). Disruption of the ESX-5 system of Mycobacterium tuberculosis causes loss of PPE protein secretion, reduction of cell wall integrity and strong attenuation. Mol. Microbiol. 83, 1195–1209. doi: 10.1111/j.1365-2958.2012.08001.x, PMID: 22340629 · doi ↗ · pubmed ↗
- 4Busam K. J.Kiehn T. E.Salob S. P.Myskowski P. L. (1999). Histologic reactions to cutaneous infections by Mycobacterium haemophilum. Am. J. Surg. Pathol. 23, 1379–1385. doi: 10.1097/00000478-199911000-00008, PMID: 10555006 · doi ↗ · pubmed ↗
- 5Choi Y. J.Kim H. J.Shin H. B.Nam H. S.Lee S. H.Park J. S.. (2012). Evaluation of peptide nucleic acid probe-based real-time PCR for detection of Mycobacterium tuberculosis complex and nontuberculous mycobacteria in respiratory specimens. Ann. Lab. Med. 32, 257–263. doi: 10.3343/alm.2012.32.4.257, PMID: 22779066 PMC 3384806 · doi ↗ · pubmed ↗
- 6Dolezalova K.Strachan T.Matej R.Ricna D.Bloomfield M. (2022). Manifestations of cutaneous mycobacterial infections in patients with inborn errors of IL-12/IL-23-IFNγ immunity. Eur. J. Dermatol. 32, 495–504. doi: 10.1684/ejd.2022.4281, PMID: 36069176 PMC 9465665 · doi ↗ · pubmed ↗
- 7Dulanto Chiang A.Dekker J. P. (2020). From the pipeline to the bedside: advances and challenges in clinical metagenomics. J. Infect. Dis. 221, S 331–Ss 40. doi: 10.1093/infdis/jiz 151, PMID: 31538184 PMC 7325616 · doi ↗ · pubmed ↗
- 8Ehtram A.Shariq M.Quadir N.Jamal S.Pichipalli M.Zarin S.. (2025). Deciphering the functional roles of PE 18 and PPE 26 proteins in modulating Mycobacterium tuberculosis pathogenesis and immune response. Front. Immunol. 16. doi: 10.3389/fimmu.2025.1517822, PMID: 39949767 PMC 11821933 · doi ↗ · pubmed ↗