A Case of Bladder Perforation With Rectal Impalement Injury
Tatsuma Juichi, Atsushi Fujikawa

TL;DR
A rare case of combined rectal impalement and bladder perforation is reported, highlighting the importance of considering bladder injury in similar trauma cases.
Contribution
This case report adds to the limited literature on combined rectal impalement and bladder perforation injuries.
Findings
A 50-year-old man with rectal impalement and bladder perforation was successfully managed with colostomy and transurethral intervention.
Extraperitoneal bladder perforation can be treated with transurethral coagulation and catheterization without major voiding or defecation dysfunction.
Gross hematuria in rectal impalement injuries should prompt suspicion of concomitant bladder perforation.
Abstract
Combined rectal impalement (RI) and bladder perforation (BP) is an extremely rare injury pattern, with limited case reports and no established consensus on their diagnosis and management. A 50‐year‐old man sustained a perianal impalement injury caused by a metal rod at a construction site. He presented with perianal pain and gross hematuria (GH). Imaging revealed RI and extraperitoneal BP. A colostomy was performed on the same day as the injury, and transurethral coagulation of the bladder (TUC) was performed on the 6th day, during which a bladder mucosal defect was identified. Postoperatively, the GH reduced, and no persistent voiding or defecation dysfunction was observed. In patients with RI and GH, concomitant BP should be suspected. Although colostomy is almost always required for rectal injury, extraperitoneal BP can be cured with transurethral intervention and catheterization.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
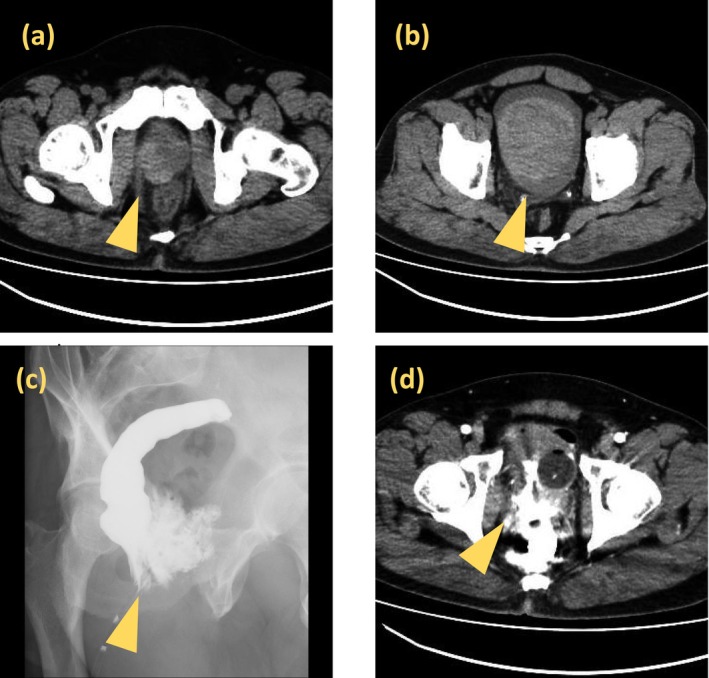 FIGURE 1
FIGURE 1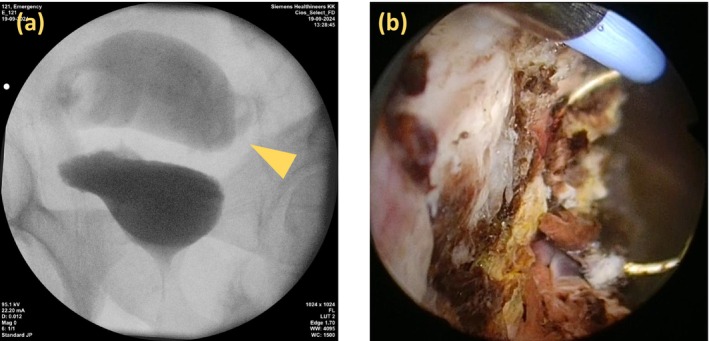 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrological Disorders and Treatments · Ureteral procedures and complications · Urinary and Genital Oncology Studies
Summary
- Simultaneous rectal impalement and bladder perforation is extremely rare.
- Gross hematuria with confirmed rectal injury should raise suspicion of bladder involvement.
- Transurethral surgery and urethral catheterization were effective for extraperitoneal bladder injury.
AbbreviationsBPbladder perforationCEcontrast enemaCTcomputed tomographyeGFRestimated glomerular filtration rateRIrectal impalementTUCtransurethral coagulation of bladderUCurethral catheter
Introduction
1
The combination of rectal impalement (RI) and bladder perforation (BP) was first described over 50 years prior [1]. Despite this, reported cases remain rare [2]. Therefore, continued accumulation of case reports and individualized, case‐by‐case clinical approaches are essential. Here, we present a rare case of combined RI and BP that was successfully treated using a multidisciplinary approach.
Case Report
2
A 50‐year‐old man with a history of cerebral hemorrhage in his 20s and residual right hemiparesis, although ambulatory without assistive devices, experienced trauma at a construction site. He fell backward onto an 8‐cm fixed metal rod protruding from the floor, which penetrated his perianal region. He managed to stand and detach from the rod, which remained embedded in the floor, but continued to experience lower abdominal and perineal pain, along with gross hematuria (GH). He presented to the emergency department approximately 2 h post‐injury.
Physical examination revealed a 2‐cm depressed perianal wound at the 11 o'clock position without active bleeding. Continuous venous bleeding from the external urethral meatus and a strong sensation of urinary retention were observed. Laboratory tests revealed mild anemia (Hb 11.4 g/dL) and elevated levels of inflammatory markers. Computed tomography (CT) showed a 4‐cm hematoma between the right anterior rectal wall and right dorsolateral prostate (Figure 1a) and a 10‐cm hematoma in the bladder (Figure 1b). Fat stranding was also observed around the rectum, particularly on the right side. No foreign bodies or free air were detected. Contrast enema (CE) revealed extravasation outside the rectum without communication with the bladder or urethra (Figure 1c). Post‐CE CT showed contrast accumulation in the rectum, perirectal space, bladder, and perivesical area, indicating combined RI and BP (Figure 1d); however, no leakage into the peritoneal cavity was observed.
(a) Non‐contrast CT showing a high‐density area (approximately 4 cm) between the right anterior wall of the rectum and the right dorsolateral prostate, suggestive of hematoma. (b) CT revealing a high‐density area (approximately 10 cm) within the bladder, also indicative of hematoma. (c) CE demonstrating extravasation of contrast medium outside the rectal lumen without bladder visualization. (d) Post‐enema CT showing high‐density contrast accumulation around the rectum, prostate, bladder, and perivesical space, raising suspicion of combined rectal and bladder injury without evidence of intraperitoneal leakage.
A urethral catheter (UC) was then inserted. The GH was mild but persistent despite saline irrigation, raising the suspicion of BP.
Emergency management prioritized the rectal injury, and a diverting colostomy was performed on the same day. During surgery, 150 mL of indigo carmine‐dyed saline was instilled into the bladder; no peritoneal leakage was observed. After the diverting colostomy, the GH gradually reduced, but did not fully resolve. On hospital day 6, transurethral surgery was performed with the patient under general anesthesia. During the procedure, simultaneous retrograde urethrocystography demonstrated contrast leakage outside the bladder with suspected visualization of the sigmoid colon or rectum (Figure 2a). Endoscopy revealed no urethral damage; however, a 2‐cm hematoma was found on the right bladder wall lateral to the right ureteral orifice. After removal, a mucosal defect with exposed fat was observed (Figure 2b), which was determined to be the BP. Coagulation achieved hemostasis, and no other bladder injuries were identified. A urethral catheter was re‐inserted postoperatively. Following the procedure, the GH was nearly resolved.
(a) Retrograde urethrocystography showing extravasation of the contrast medium outside the bladder with suspected opacification of the sigmoid colon or rectum. (b) Endoscopic image revealing a mucosal defect on the right lateral bladder wall with exposed perivesical fat, following removal of a 2‐cm hematoma. This site was identified as the source of the hematuria.
One month later, CE revealed no rectal leakage. The patient continued to undergo outpatient follow‐ups with the UC in place. No further GH or urinary leakage was observed. Three months postoperatively, cystoscopic evaluation demonstrated a mildly ulcerative lesion at the previous site of the BP; however, the perforation itself was confirmed to be fully closed. Simultaneous contrast imaging revealed no evidence of contrast medium leakage, and the UC was subsequently removed. Colostomy closure was completed 6 months post‐injury. A follow‐up cystoscopy at 7 months revealed scarring at the injury site; however, the lesion had reduced in size. The patient had no voiding dysfunction or recurrence of GH.
Discussion
3
RI injuries are typically caused by penetrating trauma from foreign objects entering directly or via the perineum and may lead to intraperitoneal or extraperitoneal rupture of the rectum and other organs, most commonly within the genitourinary tract. Although isolated RI or BP have been frequently reported, secondary BP following RI is extremely rare. Benjelloun et al. compiled 14 such cases [2], and Harada et al. subsequently reported an additional case [3]. Among the 15 cases referenced above, 13 were male, with a median age of 34 years (range: 9–57 years), indicating a predominance of younger men.
GH is the most frequent symptom of BP, occurring in up to 95% of the cases [4]. Because rectal injury can be relatively easily diagnosed through digital rectal examination and CE, the presence of GH in a patient with a confirmed rectal injury, such as in the present case, should prompt a strong suspicion of concomitant BP.
The European Association of Urology recommends the use of CT cystography to obtain rapid diagnostic information, particularly when there is a possibility of concomitant abdominal trauma [5]. In the present case, CT was performed after CE on the day of the injury, and a diverting colostomy was performed based on the diagnosis of rectal injury. The diagnosis of BP was later confirmed using TUC combined with cystography. Additionally, indigo carmine was instilled intraoperatively into the bladder to rule out intraperitoneal perforations. Although prioritizing CT cystography is reasonable in cases of isolated BP, in cases such as the present case where multiple organ injuries are involved, the diagnostic and therapeutic priorities must be carefully considered on a case‐by‐case basis.
In cases of combined rectal and bladder perforating trauma, surgical management typically involves diverting colostomies for rectal injury, and treatment outcomes are generally favorable [2, 3]. Because the most feared complication in similar cases is peritonitis due to gastrointestinal perforation, thorough evaluation of gastrointestinal lesions is essential in managing combined RI and BP. In this case, gastrointestinal surgical intervention performed on the day of injury was the greatest success factor in the treatment strategy. This prompt intervention likely contributed to the favorable clinical outcome.
When managing bladder injury, treatment planning depends on the type of injury, making it essential to distinguish between intraperitoneal and extraperitoneal BP. Intraperitoneal BP usually requires immediate surgical repair, whereas extraperitoneal BP is often managed conservatively with urethral catheterization for several weeks and has a good prognosis [6]. Extraperitoneal BP with RI is typically managed using urethral catheterization and diverting colostomy [2].
Conclusion
4
Simultaneous injuries to the rectum and bladder are rare. However, this case underscores the importance of considering concurrent bladder injury in patients presenting with RI and GH. Accurate diagnosis requires a dual approach: CE for rectal evaluation and cystography for bladder assessment. Although diverting colostomy is almost always necessary, the management of BP depends on whether the perforation is intraperitoneal or extraperitoneal. In cases involving extraperitoneal bladder injury, such as the present one, TUC for hematuria control combined with urethral catheterization has been shown to yield favorable treatment outcomes.
Consent
The patient provided informed consent for publication of this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1P. A. Johnson , “RI With Perforation of the Bladder,” British Medical Journal 2 (1971): 748–749.5090764 10.1136/bmj.2.5764.748PMC 1796378 · doi ↗ · pubmed ↗
- 2E. B. Benjelloun , Y. Ahallal , K. Khatala , et al., “RI With Bladder Perforation: A Review From a Single Institution,” Urology Annals 5 (2013): 249–254.24311904 10.4103/0974-7796.120298 PMC 3835982 · doi ↗ · pubmed ↗
- 3J. Harada , K. Takehara , and J. Watanabe , “Bladder Perforation With RI Injury: Usefulness of Exploratory Laparoscopy for Excluding Intraperitoneal Perforation,” Urology Case Reports 37 (2021): 101622.33732622 10.1016/j.eucr.2021.101622 PMC 7944034 · doi ↗ · pubmed ↗
- 4A. R. Mundy and D. E. Andrich , “Pelvic Fracture‐Related Injuries of the Bladder Neck and Prostate: Their Nature, Cause and Management,” BJU International 105 (2010): 1302–1308.19874306 10.1111/j.1464-410X.2009.08970.x · doi ↗ · pubmed ↗
- 5Y. Mahat , J. Y. Leong , and P. H. Chung , “A Contemporary Review of Adult Bladder Trauma,” Journal of Injury & Violence Research 11 (2019): 101–106.30979861 10.5249/jivr.v 11i 2.1069 PMC 6646823 · doi ↗ · pubmed ↗
- 6B. Phillips , S. Holzmer , L. Turco , et al., “Trauma to the Bladder and Ureter: A Review of Diagnosis, Management, and Prognosis,” European Journal of Trauma and Emergency Surgery 43 (2017): 763–773.28730297 10.1007/s 00068-017-0817-3 · doi ↗ · pubmed ↗