Morbidity and risk factors of COVID‐19 in people with HIV‐1 in Europe: A combined observational cohort and nested case–control study
Georg M. N. Behrens, Lambert Assoumou, Stephane De Wit, Rona MacDonald, Nathalie de Castro, Casper Rokx, Holly Middleditch, Margaret Johnson, Jose Luis Casado, Jose Ramon Arribas, Jose‐Ramon Blanco, Carl Fletcher, Caroline Eteve‐Pitsaer, Aliou Baldé, Anton Pozniak

TL;DR
This study finds that people with HIV who get COVID-19 have higher rates of certain comorbidities and longer hospital stays compared to those without HIV.
Contribution
The study identifies specific risk factors for severe outcomes in people with HIV and COVID-19 using a large observational and case–control design.
Findings
PLWH with COVID-19 had significantly higher rates of chronic kidney disease, COPD, and other comorbidities compared to HIV-uninfected patients.
Higher BMI, uncontrolled HIV viral load, and CDC stage B were significant risk factors for COVID-19 in PLWH.
PLWH with COVID-19 had longer hospital and ICU stays but similar critical care admission or death rates as HIV-uninfected patients.
Abstract
To study the COVID‐19 disease course in people living with HIV (PLWH) based on meaningful case numbers, information about comorbidities, antiretroviral and COVID‐19 treatment and HIV disease‐related variables. Multi‐centre, observational, retrospective study of people living with HIV with COVID‐19 matched to HIV‐uninfected individuals with COVID‐19 (HUC) and a case–control study of people living with HIV with COVID‐19 matched to COVID‐19 negative people living with HIV. Kaplan–Meier estimates and Cox proportional‐hazards models stratified on each matched pair were used for COVID‐19 outcomes, and conditional logistic regression models were used to identify risk factors for COVID‐19 infection. Five hundred people living with HIV and COVID‐19, 1106 HUC and 992 people living with HIV without COVID‐19 were included. Rates for chronic kidney disease, peripheral vascular disease, dementia,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
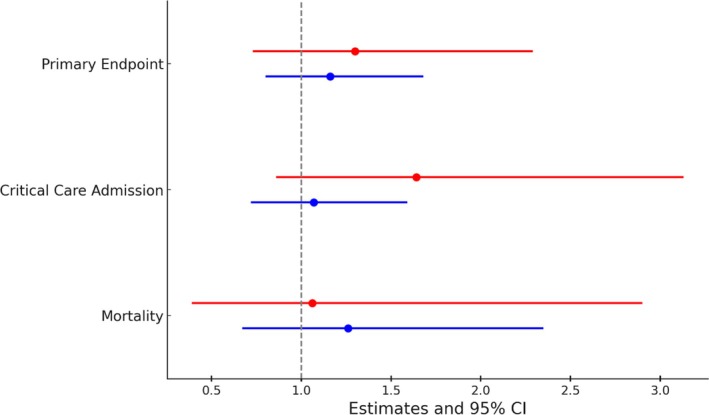 FIGURE 1
FIGURE 1| Characteristics | Participants |
| |
|---|---|---|---|
| PLWH with COVID‐19, | HUC with COVID‐19, | ||
| Age (years) | |||
|
| 486 | 1106 | |
| Median (IQR) | 51 (43–58) | 51 (43–58) | |
| [Range] | [21–89] | [21–88] | |
| Mean (SD) | 51 (11.2) | 51 (11.1) | |
|
| |||
| <60 years | 378 (77.8) | 878 (79.4) | |
| ≥60 years | 108 (22.2) | 228 (20.6) | |
| Gender, | |||
| Female | 171 (35.2) | 409 (37.0) | |
| Male | 315 (64.8) | 697 (63.0) | |
| Ethnicity, |
| ||
|
| 344 | 344 | |
| White Caucasian | 150 (43.6) | 148 (43.0) | |
| White mixed | 19 (5.5) | 24 (7.0) | |
| Asian | 4 (1.2) | 4 (1.2) | |
| Black | 105 (30.5) | 86 (25.0) | |
| Other | 8 (2.3) | 4 (1.2) | |
| Not stated | 58 (16.9) | 78 (22.7) | |
| Month of COVID‐19 diagnosis | |||
| Median (IQR) | 10/2020 (04/2020–12/2020) | 10/2020 (04/2020–12/2020) | |
| [Range] | [01/2020–03/2021] | [01/2020–03/2021] | |
| COVID‐19 diagnosis location, | |||
| Inpatient | 176 (36.2) | 176 (15.9) | |
| Outpatient (ambulatory) | 310 (63.8) | 930 (84.1) | |
| Body weight (kg) | 0.272 | ||
|
| 365 | 779 | |
| Median (IQR) | 80 (70–91) | 80 (68–92) | |
| [Range] | [38–200] | [10–184] | |
| Mean (SD) | 82 (18.0) | 81 (19.1) | |
| BMI (kg/m2) |
| ||
|
| 305 | 581 | |
| Median (IQR) | 27.0 (24.2–31.2) | 28.0 (24.6–31.5) | |
| [Range] | [14.8–69.2] | [14.7–61.3] | |
| Mean (SD) | 28.1 (6.4) | 28.7 (6.2) | |
|
| 0.112 | ||
| <30 kg/m2 | 212 (69.5) | 376 (64.7) | |
| ≥30 kg/m2 | 93 (30.5) | 205 (35.3) | |
| Comorbidities, | PLWH with COVID‐19, | PLWH without COVID‐19, |
| PLWH with COVID‐19, | HUC with COVID‐19, |
|
|---|---|---|---|---|---|---|
| Myocardial infarction | 16/500 (3.2) | 34/992 (3.4) | 0.835 | 15/395 (3.8) | 17/634 (2.7) | 0.537 |
| Congestive heart failure | 13/500 (2.6) | 20/992 (2.0) | 0.455 | 12/395 (3.0) | 21/634 (3.3) | 0.544 |
| Peripheral vascular disease | 28/500 (5.6) | 42/992 (4.2) | 0.212 | 24/320 (7.5) | 9/344 (2.6) |
|
| Stroke or transient ischaemic attack | 19/500 (3.8) | 25/992 (2.5) | 0.203 | 14/395 (3.5) | 24/634 (3.8) | 0.670 |
| Dementia | 16/500 (3.2) | 19/992 (1.9) | 0.129 | 14/320 (4.4) | 6/344 (1.7) |
|
| COPD | 36/500 (7.2) | 43/992 (4.3) |
| 31/395 (7.9) | 35/634 (5.5) | 0.143 |
| History of pneumonia | 83/500 (16.6) | 146/992 (14.7) | 0.339 | 70/395 (17.7) | 46/634 (7.3) |
|
| Connective tissue disease | 21/500 (4.2) | 25/992 (2.5) | 0.957 | 17/395 (4.3) | 144/634 (22.7) |
|
| Peptic ulcer disease | 21/500 (4.2) | 35/992 (3.5) | 0.461 | 16/395 (4.1) | 30/634 (4.7) | 0.959 |
| Liver disease | 69/500 (13.8) | 141/992 (14.2) | 0.843 | 54/395 (13.7) | 54/634 (8.5) |
|
| Diabetes | 59/500 (11.8) | 97/992 (9.8) | 0.226 | 50/395 (12.7) | 131/634 (20.7) |
|
| Hemiplegia | 2/500 (0.4) | 3/992 (0.3) | 0.753 | 2/320 (0.6) | 0/344 (0.0) | 0.987 |
| Paralysis of arm(s) or leg(s) | 3/500 (0.6) | 3/992 (0.3) | 0.396 | 3/395 (0.8) | 6/634 (1.0) | 0.533 |
| Chronic kidney disease | 38/500 (7.6) | 32/992 (3.2) |
| 36/395 (9.1) | 14/634 (2.2) |
|
| Current or history of cancer | 46/500 (9.2) | 99/992 (10.0) | 0.620 | 42/395 (10.6) | 79/634 (12.5) | 0.162 |
| Leukaemia | 1/500 (0.2) | 3/992 (0.3) | 0.726 | 1/395 (0.3) | 3/634 (0.5) | 0.504 |
| Lymphoma | 12/500 (2.4) | 30/992 (3.0) | 0.514 | 10/395 (2.5) | 10/634 (1.6) | 0.485 |
| PLWH with COVID‐19, | HUC and COVID‐19, | Crude measure of association (95% CI) | Adjusted measure of association (95% CI) | |
|---|---|---|---|---|
| Number of composite primary endpoint (critical care admission, palliative discharge, death) events | 66 | 67 | ||
| Kaplan–Meier estimate of primary endpoint—% (95% CI) | 13.6 (10.8–17.0) | 6.1 (4.8–7.6) | 1.16 (0.80–1.68) | 1.30 (0.73–2.29) |
| Number of critical care admission | 55 | 58 | ||
| Kaplan–Meier estimate of critical care admission—% (95% CI) | 11.4 (8.9–14.6) | 5.3 (4.1–6.8) | 1.07 (0.72–1.59) | 1.64 (0.86–3.13) |
| Number of palliative discharge | 1 | 0 | ||
| Kaplan–Meier estimate of palliative discharge—% (95% CI) | 0.2 (0.1–1.5) | 0.0 (0.0–0.3) | n.a. | n.a. |
| Mortality: number of deaths | 24 | 23 | ||
| Kaplan–Meier estimate of deaths—% (95% CI) | 4.9 (3.3–7.3) | 2.1 (1.4–3.1) | 1.26 (0.67–2.35) | 1.06 (0.39–2.90) |
| Characteristic | Participants |
| |
|---|---|---|---|
| PLWH and COVID‐19, | PLWH, no COVID‐19, | ||
| Age (years) | 0.971 | ||
|
| 500 | 992 | |
| Median (IQR) | 52 (44–59) | 53 (44–59) | |
| [Range] | [21–89] | [21–89] | |
| Mean (SD) | 52 (11.3) | 52 (11.2) | |
|
| 0.452 | ||
| <60 years | 388 (77.6) | 778 (78.4) | |
| ≥60 years | 112 (22.4) | 214 (21.6) | |
| Gender, | |||
| Female | 176 (35.2) | 348 (35.1) | |
| Male | 324 (64.8) | 644 (64.9) | |
| Ethnicity, | 0.260 | ||
| White Caucasian | 226 (45.2) | 464 (46.8) | |
| White mixed | 37 (7.4) | 49 (4.9) | |
| Asian | 4 (0.8) | 7 (0.7) | |
| Black | 163 (32.6) | 329 (33.2) | |
| Other | 12 (2.4) | 23 (2.3) | |
| Not stated | 58 (11.6) | 120 (12.1) | |
| Body weight (kg) |
| ||
|
| 479 | 943 | |
| Median (IQR) | 80 (70–90) | 78 (68–88) | |
| [Range] | [38–200] | [40–179] | |
| Mean (SD) | 82 (17.7) | 79 (16.1) | |
| BMI (kg/m2) |
| ||
|
| 428 | 847 | |
| Median (IQR) | 27.1 (24.3–31.3) | 26.1 (23.2–29.7) | |
| Mean (SD) | 28.1 (6.0) | 26.8 (5.4) | |
|
|
| ||
| <30 kg/m2 | 286 (66.8) | 649 (76.6) | |
| ≥30 kg/m2 | 142 (33.2) | 198 (23.4) | |
| Time since HIV diagnosis (years) |
| ||
|
| 492 | 977 | |
| Median (IQR) | 17.1 (10.7–24.5) | 18.3 (11.8–25.4) | |
| Mean (SD) | 17.8 (9.5) | 18.7 (9.3) | |
| CD4 cell nadir (cells/mm3) | 0.303 | ||
|
| 468 | 926 | |
| Median (IQR) | 224 (80–364) | 230 (110–364) | |
| Mean (SD) | 257 (213.1) | 263 (202.8) | |
| CD4 cell count (cells/mm3) | 0.204 | ||
|
| 489 | 971 | |
| Median (IQR) | 631 (417–827) | 632 (446–845) | |
| Mean (SD) | 654 (332.9) | 669 (321.9) | |
| CD4% | 0.118 | ||
|
| 483 | 956 | |
| Median (IQR) | 32.9 (24.9–40.0) | 33.3 (25.6–40.0) | |
| Mean (SD) | 32.0 (12.0) | 32.8 (11.3) | |
| CD4/CD8 ratio | 0.817 | ||
|
| 430 | 850 | |
| Median (IQR) | 0.86 (0.6–1.29) | 0.90 (0.57–1.24) | |
| Mean (SD) | 1.36 (5.8) | 1.20 (4.0) | |
| HIV viral load (copies/mL) |
| ||
|
| 492 | 976 | |
| Median (IQR) | 20 (20–40) | 20 (20–36) | |
| Mean (SD) | 15 773 (235,013.9) | 5531 (83,204) | |
|
| |||
| <50 | 423 (86.0) | 878 (90.0) | |
| ≥50 | 69 (14.0) | 98 (10.0) | |
| CDC disease stage, | 0.063 | ||
|
| 481 | 953 | |
| A | 100 (20.8) | 244 (25.6) | |
| B | 225 (46.8) | 413 (43.3) | |
| C | 156 (32.4) | 296 (31.1) | |
| AIDS, | 0.378 | ||
|
| 500 | 992 | |
| Yes | 96 (19.2) | 174 (17.5) | |
| Current ART, | 0.999 | ||
|
| 493 | 977 | |
| BIC + FTC + TAF | 73 (14.8) | 146 (14.9) | |
| DTG + 3TC + ABC | 67 (13.6) | 96 (9.8) | |
| DTG + 3TC | 62 (12.6) | 131 (13.4) | |
| DRVc + FTC + TAF | 31 (6.3) | 67 (6.9) | |
| RPV + FTC + TAF | 26 (5.3) | 32 (3.3) | |
| FTC + TDF | 21 (4.3) | 55 (5.6) | |
| DTG | 20 (4.1) | 28 (2.9) | |
| 3TC + ABC | 18 (3.6) | 39 (4.0) | |
| RPV + FTC + TDF | 17 (3.5) | 34 (3.5) | |
| EFV + FTC + TDF | 14 (2.8) | 45 (4.6) | |
| EVGc + FTC + TAF | 13 (2.6) | 31 (3.2) | |
| DTG + RPV | 12 (2.4) | 31 (3.2) | |
| Other | 119 (24.1) | 242 (24.8) | |
| 0.0596 | |||
| TDF/TAF‐based regimen | 230 (46.7) | 505 (51.7) | |
| Other regimen | 263 (53.3) | 472 (48.3) | |
| Characteristic | Participants | Conditional logistical regression model | ||||
|---|---|---|---|---|---|---|
| Univariable analysis | Multivariable analysis | |||||
| PLWH with COVID‐19, | PLWH without COVID‐19, | OR (95% CI) |
| OR (95% CI) |
| |
| Age (years) | 0.451 | |||||
| <60 | 388 (77.6) | 778 (78.4) | 1 | |||
| ≥60 | 112 (22.4) | 214 (21.6) | 1.31 (0.65–2.61) | |||
| Gender, | ||||||
| Female | 176 (35.2) | 348 (35.1) | ||||
| Male | 324 (64.8) | 644 (64.9) | ||||
| Ethnicity, | ||||||
| White Caucasian | 226 (45.2) | 464 (46.8) | 1 | 0.260 | ||
| White mixed | 37 (7.4) | 49 (4.9) | 2.41 (1.01–5.75) | |||
| Asian | 4 (0.8) | 7 (0.7) | 1.31 (011–15.4) | |||
| Black | 163 (32.6) | 329 (33.2) | 1.07 (0.28–4.11) | |||
| Other | 12 (2.4) | 23 (2.3) | 1.17 (0.15–9.43) | |||
| Not stated | 58 (11.6) | 120 (12.1) | 0.65 (0.11–3.67) | |||
| Body weight (kg), median (IQR) |
| |||||
|
80 (70–91) |
77 (68–88) | 1.74 (1.34–2.25) | ||||
| BMI (kg/m2) |
|
| ||||
| <30 kg/m2 | 336 (67.1) | 756 (76.2) | 1 | 1 | ||
| ≥30 kg/m2 | 164 (32.9) | 236 (23.8) | 1.68 (1.29–2.19) | 1.73 (1.32–2.26) | ||
| Comorbidities, | ||||||
| Myocardial infarction (heart attack) | 16 (3.2) | 34 (3.4) | 0.94 (0.5–1.75) | 0.835 | ||
| Congestive heart failure | 13 (2.6) | 20 (2.0) | 1.31 (0.65–2.67) | 0.455 | ||
| Peripheral vascular disease | 28 (5.6) | 42 (4.2) | 1.41 (0.82–2.40) | 0.212 | ||
| Cerebrovascular accident (stroke) or transient ischaemic attack | 19 (3.8) | 25 (2.5) | 1.51 (0.80–2.85) | 0.203 | ||
| Dementia | 16 (3.2) | 19 (1.9) | 1.71 (0.86–3.41) | 0.129 | 1.65 (0.80–3.39) | 0.178 |
| Chronic obstructive pulmonary disease | 36 (7.2) | 43 (4.3) | 1.93 (1.16–3.22) |
| 1.83 (1.07–3.11) |
|
| History of pneumonia | 83 (16.6) | 146 (14.7) | 1.16 (0.85–1.58) | 0.339 | ||
| Connective tissue disease | 21 (4.2) | 25 (2.5) | 1.69 (0.91–3.13) | 0.957 | ||
| Peptic ulcer disease | 21 (4.2) | 35 (3.5) | 1.26 (0.68–2.31) | 0.461 | ||
| Liver disease | 69 (13.8) | 141 (14.2) | 0.97 (0.69–1.35) | 0.843 | ||
| Diabetes | 59 (11.8) | 97 (9.8) | 1.25 (0.87–1.79) | 0.226 | ||
| Hemiplegia | 2 (0.4) | 3 (0.3) | 1.33 (0.22–7.98) | 0.753 | ||
| Paralysis of arm(s) or leg(s) | 3 (0.6) | 3 (0.3) | 2.00 (0.40–9.91) | 0.396 | ||
| Chronic kidney disease | 38 (7.6) | 32 (3.2) | 2.71 (1.61–4.57) |
| 2.19 (1.28–3.74) |
|
| Current or history of cancer | 46 (9.2) | 99 (10.0) | 0.91 (0.61–1.34) | 0.620 | ||
| Leukaemia | 1 (0.2) | 3 (0.3) | 0.67 (0.07–6.41) | 0.726 | ||
| Lymphoma | 12 (2.4) | 30 (3.0) | 0.80 (0.41–1.56) | 0.514 | ||
| Time since HIV diagnosis | ||||||
| Per 10 unit for the model | 17.1 (10.7–24.6) | 18.3 (11.8–25.3) | 0.85 (0.74–0.99) |
| 0.86 (0.74–1.00) | 0.057 |
| CD4 cell nadir | ||||||
| Per 100 unit for the model | 224 (81–364) | 226 (107–360) | 0.98 (0.93–1.04) | 0.458 | ||
| CD4 cell count | ||||||
| Per 100 unit for the model | 630 (414–827) | 630 (443–840) | 0.99 (0.95–1.02) | 0.453 | ||
| CD4% | ||||||
| Per 100 unit for the model | 32.9 (25.0–40.0) | 33.1 (25.0–40.0) | 0.95 (0.86–1.05) | 0.296 | ||
| CD4/CD8 ratio | 0.86 (0.52–1.31) | 0.89 (0.54–1.28) | 1.00 (0.98–1.02) | 0.734 | ||
| HIV viral load (copies/mL) |
|
| ||||
| <50 | 427 (85.4) | 888 (89.5) | 1 | 1 | ||
| ≥50 | 73 (14.6) | 104 (10.5) | 1.67 (1.13–2.45) | 1.52 (1.01–2.29) | ||
| CDC disease stage, | 0.051 |
| ||||
| A | 104 (20.8) | 248 (25.0) | 1 | 1 | ||
| B | 236 (47.2) | 430 (43.3) | 1.49 (1.08–2.06) | 1.51 (1.09–2.10) | ||
| C | 160 (32.0) | 314 (31.7) | 1.29 (0.93–1.78) | 1.21 (0.87–1.70) | ||
| AIDS, | 0.378 | |||||
|
| 500 | 992 | ||||
| Yes | 96 (19.2) | 174 (17.5) | 1.15 (0.85–1.55) | |||
| Current ART, | 0.0887 | 0.1358 | ||||
| TDF/TAF‐based regimen | 237 (47.3) | 514 (51.8) | 1 | 1 | ||
| Other regimen | 263 (52.7) | 478 (48.2) | 1.21 (0.97–1.50) | 1.19 (0.95–1.49) | ||
- —Gilead Sciences10.13039/100005564
- —NEAT‐ID
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · Long-Term Effects of COVID-19 · COVID-19 and healthcare impacts
INTRODUCTION
The COVID‐19 pandemic was a public health emergency of international concern with mortality rates of 2%–4% and the highest death risk in elderly male patients and those with comorbidities including arterial hypertension, cardiovascular disease, chronic lung disease, obesity and diabetes. Preliminary data reported the disease course of COVID‐19 in specific patient groups with immunosuppression or people living with HIV [1, 2, 3, 4] and some suggested that people living with HIV may have some degree of protection due to their antiretroviral therapy (ART) compounds [5, 6, 7, 8]. Irrespective of their ART, people living with HIV with comorbidities were expected to have risk factors for poorer COVID‐19 outcomes, since cardiovascular and chronic lung disease are more common in this population and almost half of people living with HIV in Europe are older than 50 years. Also, incomplete immune reconstitution may put them at risk for severe COVID‐19.
Case series of people living with HIV with COVID‐19 from China, Spain, Germany, Italy and the United States [3, 9, 10, 11, 12, 13, 14, 15, 16] showed no clear evidence for a higher SARS‐CoV‐2 infection rate or different disease course in people with and without HIV. Of note, most case series of people living with HIV reported a younger age in their study population than in HIV‐negative hospitalized COVID‐19 patients, but comparable rates of comorbidities.
Among the larger studies, a retrospective cohort of electronic medical record data in the United States found that people living with HIV and more advanced HIV disease (greater immunosuppression and HIV viraemia) were at higher risk for severe COVID‐19 outcomes [17]. An analysis, in which outcomes in COVID‐19 positive people living with HIV were compared with a propensity‐matched cohort of patients without HIV, found that the crude COVID‐19 mortality was higher in people living with HIV. However, propensity‐matched analyses revealed no difference in outcomes, showing that higher mortality is driven by a higher burden of comorbidities [18]. A cohort study from the United Kingdom reported a potential increase in the risk of mortality among people living with HIV under 60 years of age once hospitalized with COVID‐19. Mortality was higher among people living with HIV after adjusting for age (adjusted hazard ratio 1.47, 95% confidence interval [CI], 1.01–2.14; p = 0.05), and the association persisted after adjusting for the other variables and when restricting the analysis to people aged <60 years. However, the study provided no data around the risk of developing severe COVID‐19 or hospitalization among this cohort of 112 people living with HIV and no data on viral load or CD4 count [19]. A retrospective study from Spain with 749 people living with HIV and COVID‐19 found that SARS‐CoV‐2 diagnosis was more common among migrants, men who have sex with men and those with four or more chronic comorbidities. Age above 75 years, non‐Spanish origin and neuropsychiatric, autoimmune disease, respiratory disease and metabolic disease chronic comorbidities were associated with an increased risk of severe outcomes [20]. An analysis of risk factors for COVID‐19 deaths in the Western Cape described that after adjusting for other risk factors, HIV increased a COVID‐19 patient's death risk by a factor of 2.14 (95% CI, 1.70–2.70) [21].
A meta‐analysis [22] concluded that people living with HIV and HIV‐negative individuals showed comparable rates and intensity of COVID‐19. ART users exhibited immunological health comparable to immunocompetent people, demonstrating the essential role of antiretroviral therapy in reducing the severity and mortality of people living with HIV with COVID‐19. Another narrative review [23] reported that out of 57 studies assessing risk factors and clinical outcomes in HIV patients co‐infected with COVID‐19, 39 of the studies indicated several comorbidities being associated with severe outcomes in HIV and COVID‐19, whilst 20 studies reported no difference in clinical outcomes.
To date, many studies assessing the risk factors for COVID‐19 and clinical outcomes in people living with HIV were restricted by the number of cases (mostly 100–200 people living with HIV and COVID‐19), were solely created from medical record databases or included only hospitalized patients, were deficient in completeness of data on comorbidities and biomedical data, frequently lacked information on antiretroviral or COVID‐19 treatment, failed to include HIV disease‐related parameters and had clear limitations when comparing people living with HIV without COVID‐19 as control groups. To overcome these limitations, we performed an observational, retrospective study with 500 people living with HIV and COVID‐19 recruited from multiple European sites and two control groups with 2098 patients to simultaneously evaluate the severity of COVID‐19 in people living with HIV as compared to control COVID‐19 cases without HIV as well as to describe risk factors for COVID‐19 within the group of people living with HIV.
MATERIALS AND METHODS
The HIV COVID‐19 Co‐Infection (HIV CoCo) Study is an observational, retrospective combined exposure/non‐exposure and case–control study. The study population consisted of adult people living with HIV with and without COVID‐19 disease followed up at 21 study sites in five countries (UK, Spain, France, Belgium and the Netherlands) for routine clinical care. In addition, data from adult HIV‐uninfected COVID‐19 patients were used as controls. People living with HIV and COVID‐19 were identified from sites in the NEAT ID network after launching a dashboard in March 2020, in which 50 European sites registered to provide basic information about the number of people living with HIV with COVID‐19 and disease outcomes (https://www.NEAT-ID.org/). Ambulatory HUC were identified from COVID‐19 outpatients from THIN® France (The Health Improvement Network), a European clinical database network of Electronic Health Records extracts. These extracts are transmitted in compliance with current regulations, including General Data Protection Regulation (GDPR) by a network of voluntary physicians (general practitioners and specialists, https://www.the‐health‐improvement‐network.com). Hospitalized HUC were identified from NEAT ID network sites.
Cases (people living with HIV and COVID‐19) were at least 18 years of age with documented HIV‐1 infection and confirmed COVID‐19 by documented, or patient‐reported, positive result on polymerase chein reaction (PCR) testing of a nasopharyngeal or respiratory sample, before 1 April 2021 when COVID‐19 vaccination became available. HUC were at least 18 years of age without documented HIV‐1 infection but confirmed COVID‐19 by documented, or patient‐reported, positive result on PCR testing of a nasopharyngeal or respiratory sample, before 1 April 2021. The second control group (people living with HIV without COVID‐19) included individuals at least 18 years of age with documented HIV‐1 infection and no COVID‐19.
For comparing people living with HIV with COVID‐19 versus HUC, we performed a 1:1 and 1:3 matching according to the following criteria: age (±5 years), sex, ethnicity (where available), month of COVID‐19 diagnosis (±2 months) and diagnosis as inpatient or outpatient. Inpatients with COVID‐19 diagnosis were matched 1:1; ambulatory patients with COVID‐19 were matched at 1:3. For comparing people living with HIV and COVID‐19 versus people living with HIV without COVID‐19, individuals were matched at 1:2 for similar risk of acquiring COVID‐19 according to the following criteria: age (±5 years), sex, ethnicity (where available).
Data collection
For all patients, we collected age, sex, ethnicity (where available), comorbidities (including myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular accident or transient ischaemic attack, dementia, chronic obstructive pulmonary disease [COPD], history of pneumonia, connective tissue disease, peptic ulcer disease, liver disease, diabetes, hemiplegia, paralysis of arm[s] or leg[s], chronic kidney disease [CKD], current or history of cancer, leukaemia, lymphoma, AIDS [where applicable]), body mass index (BMI), Charlson Comorbidity Index (CCI) and age‐adjusted CCI (ACCI). For people living with HIV, the following additional data were collected: date of HIV diagnosis, current antiretroviral therapy, Centers for Disease Control and Prevention (CDC) disease stage, CD4 T lymphocyte nadir, last (≤6 months) CD4 T cell count (including CD4 T cell percentage and CD4/CD8 ratio) and last HIV‐RNA before COVID‐19 diagnosis, or most recent (≤6 months). For patients with COVID‐19, the following additional information was collected, if available: date of positive PCR test result (documented or patient‐reported), COVID‐19 diagnosis inpatient or outpatient, all‐cause mortality in hospital or palliative discharge, or mortality at 6 weeks after diagnosis of COVID‐19 or at discharge from hospital, hospitalization for COVID‐19 and length of hospitalization, critical care admission (high dependency unit or intensive care unit) for COVID‐19 and length of stay in critical care, length of invasive ventilation (number of ventilator‐free days), length of extracorporeal membrane oxygenation (ECMO), need for kidney replacement therapy, laboratory markers and blood cell counts at COVID‐19 diagnosis (e.g., Alanine‐aminotransferase, Aspartate‐aminotransferase (AST), serum creatinine, calcium, glucose and HbA1c levels, C‐reactive protein [CRP], D‐dimer and lactate dehydrogenase) and drug treatment for COVID‐19. Real‐world retrospective data from people living with HIV and from hospitalized HUC were transcribed into the eCRF system from source data at each clinical site. Data from ambulatory HUC were obtained from THIN® France, a network of longitudinal databases covering over 35 million electronic health records.
Outcomes
The primary outcomes of our study were (1) the proportion of participants with a severe form of COVID‐19 infection (critical care admission [high dependency unit or intensive care unit], or palliative discharge when discharged from hospital, or mortality within the 6 weeks after diagnosis of COVID‐19) in people living with HIV in comparison to HUC, and (2) identifying risk factors (e.g., CD4 T cell nadir, current CD4 T cell count, comorbidities) for COVID‐19 infection within the group of people living with HIV.
Statistical analysis
For the sample size calculation and statistical analysis, please see Supplementary material.
RESULTS
Objective 1: Outcomes of COVID‐19 in people living with HIV in comparison to HIV‐uninfected COVID‐19 controls
In total, we included 500 people living with HIV and COVID‐19, 1106 HUC with COVID‐19 and 992 people living with HIV without COVID‐19. Fourteen inpatient people living with HIV with COVID‐19 had no control. The key baseline demographics and clinical characteristics are listed in Table 1, which also contains information about other matching criteria.
The 486 people living with HIV with COVID‐19 had a median age of 51 years (interquartile range, IQR 15); 108 (22.2%) were ≥60 years, 315 (64.8%) were male, 150/344 (43.6%) were white Caucasians and their median BMI was 27.0 kg/m^2^ (IQR 24.2–31.2).
People living with HIV and COVID‐19 compared to HUC had higher rates of CKD (9.1 vs. 2.2%, p < 0.001), peripheral vascular disease (7.5% vs. 2.6%, p = 0.006), dementia (4.4% vs. 1.7%, p = 0.039), history of pneumonia (17.7% vs. 7.3%, p < 0.001) and liver disease (13.7% vs. 8.5%, p = 0.003), and lower rates of connective tissue disease (4.3% vs. 22.7%, p < 0.001) and diabetes (12.7% vs. 20.7%, p < 0.001, Table 2).
People living with HIV and COVID‐19 had significantly lower median values for red blood cell counts (p = 0.002), lactate dehydrogenase (p = 0.038) and AST (p = 0.009) but their median values for mean corpuscular volume (MCV, p < 0.001), mean corpuscular haemoglobin (MCH, p < 0.001), lymphocyte counts (p < 0.001), serum creatinine (p = 0.020) and total cholesterol (p = 0.041) were higher (Table S1). People living with HIV and COVID‐19 were more often treated with hydroxychloroquine (49.2% vs. 38.0%, p = 0.007), but less often with glucocorticoids (29.4% vs. 48.6%, p = 0.002), anti‐IL 6 inhibitors (6.4% vs. 15.5%, p = 0.010) or other experimental treatments (16.5% vs. 30.3%, p = 0.008, Table S2).
Results for the composite primary endpoint and secondary endpoints are listed in Table 3 and depicted in Figure 1. The absolute Kaplan–Meier estimate of the primary endpoint was 13.6% in people living with HIV and COVID‐19 and 6.1% in HUC and COVID‐19, with an adjusted HR (aHR) of 1.30 (95% CI, 0.73–2.29). The same applies to the risk of mortality 6 weeks after COVID‐19 (aHR 1.06; 95% CI, 0.39–2.90) and admission to critical care (aHR 1.64; 95% CI, 0.86–3.13). Only one people living with HIV with COVID‐19 received palliative discharge, and none in the HUC and COVID‐19 group. The adjusted sub‐distribution HR (sHR) for cumulative incidence for discharge from the hospital was 0.63; 95% CI, 0.48–0.84, and cumulative incidence for discharge from ICU was 0.06; 95% CI, 0.01–0.34. This means that the median length of hospital and ICU stay was longer in people living with HIV and COVID‐19 than in HUC. Interestingly, the age‐adjusted CCI was significantly higher in people living with HIV and COVID‐19 than in HUC (adjusted mean difference 1.62; 95% CI, 1.14–2.22), as were differences in mean MCV (4.30; 95% CI, 2.77–5.85) and mean MCH (1.55; 95% CI, 1.09–2.01). The need for kidney replacement therapy had an adjusted odds ratio (aOR) of 1.81; 95% CI, 0.54–6.02 (Table S3).
Primary and secondary outcomes of people living with HIV with COVID‐19 versus COVID‐19. Depicted are the crude (blue) and adjusted measures (red) of association (95% confidence interval [CI]) for the composite primary endpoint (critical care admission, palliative discharge, death), critical care admission and mortality. For adjusted factors, see Table 3.
In summary, rates of CKD, peripheral vascular disease, dementia, history of pneumonia and liver disease were between 0.6‐ and 3.1‐fold higher in people living with HIV and COVID‐19, whilst rates for diabetes and connective tissue disease were 0.6‐fold and 4.2‐fold lower compared to HUC. In line with this, people living with HIV and COVID‐19 had a higher median AACI, and their relative risk for severe COVID‐19 disease outcome increased by 30%.
Objective 2: Risk factors for severe COVID‐19 outcomes within the group of people living with HIV
The baseline demographics and clinical characteristics of people living with HIV with COVID‐19 versus people living with HIV without COVID‐19 are listed in Table 4. Compared to people living with HIV and no COVID‐19, the median age, sex and ethnicity (where available) were matching criteria and thus similar. Compared to people living with HIV and no COVID‐19, the median BMI in people living with HIV with COVID‐19 was significantly higher (27.1 kg/m^2^ [IQR 7] vs. 26.1 kg/m^2^ [IQR 6.5], p < 0.001), and people living with HIV with COVID‐19 had more comorbidities (Table 2). COPD (7.2% vs. 4.3%, p = 0.012) and CKD (7.6% vs. 3.2%, p < 0.001) were 1.67‐fold and 2.37‐fold different. People living with HIV and COVID‐19 had a shorter median time since HIV diagnosis (17.1 years [IQR 13.3] vs. 18.3 years [IQR 13.6], p = 0.005).
Whilst CD4 T cell counts, CD4/CD8 T cell ratio, HIV CDC disease stage and compositions of antiretroviral therapy regimens were not different between the groups, the proportion of people living with HIV and COVID‐19 with detectable HIV‐RNA was significantly higher (14% vs. 10%, p = 0.008).
Using a multivariable analysis, we identified the following significant risk factors for COVID‐19 in people living with HIV: CKD (aOR 2.19; 95% CI, 1.28–3.74, p = 0.004), COPD (aOR 1.83; 95% CI, 1.07–3.11, p = 0.027), BMI ≥30 kg/m^2^ (aOR 1.73; 95% CI, 1.32–2.26, p < 0.001), CDC stage B versus A (aOR 1.51; 95% CI, 1.09–2.10, p = 0.042) and HIV‐RNA above 50 copies/mL (aOR 1.52; 95% CI, 1.01–2.29 [p = 0.045]) (Table 5).
DISCUSSION
Our study revealed that people living with HIV and COVID‐19 have higher rates of several comorbidities, including CKD, as compared to HUC, but a well‐controlled HIV infection was not identified as an independent risk factor for severe COVID‐19 outcomes (critical care admission, palliative care discharge, death); although associations with a longer length of hospital and ICU stay were found. In their 2023 systematic review, Hanson et al. conclude that, according to the literature, morbidity and mortality associated with SARS‐CoV‐2 infection in people living with HIV is complex and that there is no clear consensus thus far [24]. Whilst two systematic reviews and eight individual studies found an increased rate of mortality, hospitalizations and/or severe COVID‐19 outcomes in people living with HIV co‐infected with SARS‐CoV‐2, the other five systematic reviews and six individual studies concluded people living with HIV were not at an increased risk compared to patients without HIV [24]. In a more recent systematic review [22] published in 2024 and evaluating the severity and outcome of COVID‐19 in people living with HIV with COVID‐19 and COVID‐19 controls, the authors concluded that people living with HIV and HIV‐negative individuals showed comparable rates and intensity of COVID‐19. In view of these open questions, our results add important novel evidence based on a solid study design to address this relevant question.
In our study, CKD and multi‐morbidity also stand out as significant risk factors for COVID‐19 in people living with HIV compared to people living with HIV with no COVID‐19. Interestingly, instead of CD4 T cell counts or CD4/CD8 T cell ratio, which are routine immunological surrogate markers for HIV disease stage and immune function, we identified CDC disease stage and detectable HIV‐RNA as risk factors for COVID‐19 infection [25]. The influence of comorbidities on COVID‐19 outcomes has been recognized since the earliest days of the pandemic. Understanding the impact of comorbidity in COVID‐19 facilitates prioritization for interventions (preventive measures, vaccination and early treatment) and it may deepen understanding of the underlying biology of the disease [26]. In the ISARIC4C study [27] more than three‐quarters of hospitalized patients with COVID‐19 had at least one comorbidity, and patients with cardiac disease, pulmonary disease, CKD, obesity, cancer, chronic neurological disorders, dementia and/or liver disease had an increased risk of in‐hospital mortality. Among more than 1700 participants in the UK Biobank with severe SARS‐CoV‐2 infection, about 25% had multi‐morbidity, defined from a list of 12 comorbidities [28]. The combination of stroke and hypertension was most prevalent, and the combination of CKD and diabetes was associated with the highest risk of severe COVID‐19 (OR 4.93; 95% CI, 3.36–7.22). In a UK cohort study [29] using primary‐care data, 15 comorbidity groupings were evaluated together with BMI. The most common comorbidity was hypertension (34.3%), followed by asthma (15.9%) and diabetes (9.9%). However, in age‐ and sex‐adjusted regression models, all comorbidity groups were associated with increased risk of death from COVID‐19; the greatest risk was found in organ‐transplant recipients (HR 6.00; 95% CI, 4.73–7.61) and in those with CKD (HR 3.48 [3.23–3.75]). Interestingly, the magnitude of association was greater in analyses restricted to the earlier pandemic period [26]. We also found some interesting differences in the treatment regimens against COVID‐19 between people living with HIV and HUC since the former received glucocorticoids and anti‐IL 6 inhibitors less often but hydroxychloroquine more often. We can only speculate whether the known HIV status led to more hesitation to treat COVID‐19 in people living with HIV with further immunosuppressive medication.
Depending on the study design and samples size, there are conflicting reports on risk‐factors for COVID‐19 and disease outcomes in people living with HIV. In line with our study, higher rates of comorbidities in people living with HIV and COVID‐19 as compared to matched controls were reported by others [11], and these included COPD, cirrhosis and a history of cancer diagnosis. People living with HIV and uninfected controls had similar COVID‐19 severity on admission as measured by oxygen supplementation requirements but comparable COVID‐19 disease outcomes. A review [23] of 30 studies reported risk factors associated with severity of diseases (e.g., older age, higher BMI, male sex, ethnicity, obesity, smoking, CKD, diabetes, cardiovascular disease, lung cancer, African American, high viral load, low CD4 T cell count, discontinued ART usage and some ART regimens), but very few of these risk factors were confirmed in other studies. Also, 20 studies indicated that clinical presentations among the people living with HIV and COVID‐19 were the same as the general population therefore there was low risk of disease severity [23]. Whilst our study confirms that comorbidities are more prevalent in people living with HIV with COVID‐19 in general (e.g., higher BMI, peripheral vascular disease, dementia, history of pneumonia and liver disease), we provide additional evidence for higher BMI, COPD and HIV disease stage as risk factors for COVID‐19 infection in people living with HIV. In this regard, our study presents for the first time high‐level evidence for CKD being a particular risk factor in people living with HIV, since this condition was significantly more prevalent in people living with HIV with COVID‐19 compared to both control groups. In addition, people living with HIV and COVID‐19 showed a trend to more kidney replacement therapy. Whilst CKD and dialysis are important risk factors for severe COVID‐19 in general [29], especially when combined with other morbidities [29], and COVID‐19 leads to short and long term kidney [30] damage, thus far only a small study indicated chronic kidney dysfunction as potential risk factor in people living with HIV [31]. In contrast, we were surprised to see that the rate of diabetes in people living with HIV and COVID‐19 was significantly lower as compared to COVID‐19 patients without HIV. Whilst an association between diabetes and life‐threatening disease in hospitalized people with COVID‐19 has been described [27] since early in the pandemic, type 2 diabetes often co‐occurs with obesity and cardiovascular disease and is more prevalent in older individuals. Today there seems to be more evidence that type 2 diabetes itself is not causally associated with adverse outcomes in COVID‐19, in contrast to the closely related trait of obesity [32, 33]. Finally, by comparing people living with HIV and COVID‐19 and HUC, we are also evaluating people with and without HIV, independently of COVID‐19 status and this could lead to confounders. Data on the prevalence of conditions such as CKD in cohorts of people living with HIV and seronegative controls matched for age, sex and ethnicity are very limited. The COCOMO Study, for example, provides evidence for a higher prevalence of CKD in people living with HIV, but no increased rates of type 2 diabetes [34]. Therefore, the identification of CKD in our cohort could partially reflect a higher underlying prevalence of CKD in people living with HIV. The same may apply to conditions such as prior pneumonia or liver disease. In contrast, cardiovascular disease (CVD)—which is known to be more prevalent in people living with HIV and a risk factor for severe COVID‐19—did not emerge as a significant risk factor in our analysis. Conversely, type 2 diabetes, another known risk factor for severe COVID‐19, was significantly less common among people living with HIV.
When we started our study, several comorbidities were already described as general risk factors for COVID‐19 and disease courses, which encouraged us to collect many comorbidities for our analysis. The question arises, whether the higher prevalence we found for some conditions in people living with HIV and COVID‐19 is interrelated to the higher pre‐existing comorbidities in people living with HIV in general or associated with COVID‐19 disease? Arguments for the former scenario come from a study analysing the hospital admissions [35]. The authors observed the greatest comorbidity disparities between HIV‐positive and HIV‐negative admissions for mild liver disease (prevalence ratio [PR], 4.9; 95% CI, 4.8–5.1), moderate or severe liver disease (PR, 2.2; 95% CI, 2.0–2.4) and chronic pulmonary disease (PR, 1.8; 95% CI, 1.8–1.8) and these conditions are two among others that we found more often in people living with HIV and COVID‐19. Yet, people living with HIV and COVID‐19 had higher rates of the above‐mentioned comorbidities despite the most likely above‐normal comorbidity rates in the COVID‐19 controls. It is also important to consider that the significant association of a very broad range of comorbidities with hospitalization and death is consistent across not only studies of COVID‐19, but also a range of other respiratory and systemic illnesses. This, together with the strong, consistent signal that multi‐morbidity is the biggest risk factor for severe COVID‐19, suggests that the impact of these comorbidities is not specific to COVID‐19, or even to respiratory disease [26].
We would like to highlight some unique qualities in our study design, which we consider advantageous as compared to previous reports about HIV and COVID‐19. First, the large multi‐centre design (21 sites and five countries) ensured representative data collection of abundant case numbers (people living with HIV and COVID‐19) with matched people living with HIV controls recruited from the same sites and regions. This enabled us to integrate the distinct control group of people living with HIV without COVID‐19. Second, we included important information on HIV disease stage including current CD4 T cell count, HIV‐RNA and antiretroviral therapy. Third, we were able to control for age, sex and ethnicity as known risk factors for the COVID‐19 disease course. We also matched for the time of COVID‐19 diagnosis to contain variability due to, for example, constraints in health care services during the early phase of the pandemic and matched for place of COVID‐19 diagnosis (inpatient/ambulatory), which otherwise could have had an important influence on the primary and secondary outcome measures. Fourth, we measured 17 different comorbidities, most of which have known impact on either SARS‐CoV‐2 infection and/or COVID‐19 disease course and included the CCI as an established score to estimate mortality risk in people with multi‐morbidity. Fifth, when defining inclusion criteria and our composite primary endpoint, we deliberately avoided hospitalization as a component. Associations reported between comorbidities and outcomes in studies of populations of hospitalized patients with COVID‐19 could be biased owing to the criteria for entry into the study (that is, requirement for hospitalization) being causally associated with both the comorbidity [36] and the outcome. Studies undertaken in populations that are not restricted to hospitalized individuals are less likely to report associations affected by this bias [26]. Caution is also needed when severity is defined by health‐service use or intervention (that is, hospitalization [37], critical care admission or respiratory support), as the presence of a comorbidity (e.g., HIV infection) might influence clinical decision making, either lowering or increasing the threshold for hospitalization or provision of organ support. It is possible that the extreme capacity strain in many areas during the early peak of the COVID‐19 pandemic may have augmented this effect with relevance to people with known HIV status [26]. To strengthen in‐hospital related severe COVID‐19 disease outcomes, we captured important secondary outcomes including number of ventilator‐free days, length of extracorporeal membrane oxygenation (ECMO) and need for kidney replacement therapy.
Our study also has some limitations. We did not assess COVID‐19 related parameters like baseline SARS‐CoV‐2 viral load, which can have an impact on the COVID‐19 disease course and most people living with HIV had good immune function with median CD4 T cell counts above 600 cells per mL [38]. We do not have complete biomedical data for all individuals, and we were unable to assess, for example, socioeconomic factors, which together with ethnicity and environment influence the likelihood of infection and subsequent outcomes [26]. Whilst several sites from European countries participated in this study, we are not fully representative of the entire European region. One could consider the fact that our study period is restricted to the time before the start of widespread COVID‐19 vaccination as a limitation. However, since vaccinations and hybrid immunity significantly influenced the COVID‐19 disease course, we expected that the impact of, for example, number of COVID‐19 vaccinations, various vaccine schedules and infections with different SARS‐CoV‐2 variants would have been important confounders and difficult to control for [39]. Thus, we can only make conclusions about the initial phase of the corona pandemic when SARS‐CoV‐2 hit people living with HIV with a naïve immune system for the infection. When comparing people living with HIV who have and have not had COVID‐19, it is important to consider that those who seek testing and report infection may differ in baseline characteristics from those who do not, potentially introducing bias. Also, self‐reporting is unreliable and might influence the results. We believe that recruiting people living with HIV as controls from the same sites or outpatient clinics where the people living with HIV and COVID‐19 cases were diagnosed and treated was the most practical way to reduce confounding effects related to variations in pandemic waves, healthcare systems, testing strategies or sociodemographic factors.
In summary, based on improved evidence, our study did not identify a well‐controlled HIV infection as a significant risk factor for severe COVID‐19 overall, but we found associations with a longer length of hospital and ICU stay. We confirmed several risk factors for COVID‐19 in people living with HIV, among which our study identified CKD and multi‐morbidity of particular relevance.
AUTHOR CONTRIBUTIONS
Study design: Georg M. N. Behrens, Anton Pozniak and Lambert Assoumou. Data collection and curation: Stephane De Wit, Rona MacDonald, Nathalie de Castro, Casper Rokx, Holly Middleditch, Margaret Johnson, Jose Luis Casado, Jose Ramon Arribas, Jose‐Ramon Blanco, Caroline Eteve‐Pitsaer, Carl Fletcher. Data analysis: Aliou Baldé and Lambert Assoumou. Data interpretation: Lambert Assoumou, Georg M. N. Behrens, Anton Pozniak and Esteban Martinez. Writing: Georg M. N. Behrens, Anton Pozniak and Esteban Martinez with comments from all authors. Georg M.N. Behrens and Lambert Assoumou have directly accessed and verified the underlying data reported in the manuscript.
FUNDING INFORMATION
This work was supported by an investigator‐sponsored research grant (ISR) from Gilead (IN‐DE‐983‐6076) and the NEAT ID Foundation.
CONFLICT OF INTEREST STATEMENT
Georg M. N. Behrens has received honoraria for lectures and advisory boards from Gilead, ViiV Healthcare, MSD, Janssen, Novartis, EUROIMMUN, Moderna and Pfizer. He received funding for research from Novartis to his institution unrelated to this work. Esteban Martinez has received honoraria for lectures or advisory boards from Gilead, Janssen, MSD and ViiV, and his institution has received research grants from MSD and ViiV. Anton Pozniak has received honoraria for lectures and advisory boards from Gilead, ViiV Healthcare and MSD. Casper Rokx declares honoraria for advisory boards and a research grant for investigator‐initiated studies from Gilead and ViiV Healthcare paid to his institution. All other authors declare no conflicts of interest.
ETHICS STATEMENT
The NAET ID HIV CoCo Study (NCT05481216) and the analysis conducted for this article were approved by the relevant ethics committees in the United Kingdom, Spain, Belgium and the Netherlands.
Supporting information
Data S1. Supporting information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blanco JL , Ambrosioni J , Garcia F , et al. COVID‐19 in patients with HIV: clinical case series. Lancet HIV. 2020;7(5):e 314‐e 316.32304642 10.1016/S 2352-3018(20)30111-9PMC 7159872 · doi ↗ · pubmed ↗
- 2Harter G , Spinner CD , Roider J , et al. COVID‐19 in people living with human immunodeficiency virus: a case series of 33 patients. Infection. 2020;48(5):681‐686.32394344 10.1007/s 15010-020-01438-z PMC 7211976 · doi ↗ · pubmed ↗
- 3Karmen‐Tuohy S , Carlucci PM , Zervou FN , et al. Outcomes among HIV‐positive patients hospitalized with COVID‐19. J Acquir Immune Defic Syndr. 2020;85(1):6‐10.32568770 10.1097/QAI.0000000000002423 PMC 7446982 · doi ↗ · pubmed ↗
- 4Zhao J , Liao X , Wang H , et al. Early virus clearance and delayed antibody response in a case of coronavirus disease 2019 (COVID‐19) with a history of coinfection with human immunodeficiency virus type 1 and hepatitis C virus. Clin Infect Dis. 2020;71(16):2233‐2235.32270178 10.1093/cid/ciaa 408PMC 7184426 · doi ↗ · pubmed ↗
- 5Nutho B , Mahalapbutr P , Hengphasatporn K , et al. Why are lopinavir and ritonavir effective against the newly emerged coronavirus 2019? Atomistic insights into the inhibitory mechanisms. Biochemistry. 2020;59(18):1769‐1779.32293875 10.1021/acs.biochem.0c 00160 · doi ↗ · pubmed ↗
- 6Del Amo J , Polo R , Moreno S , et al. Incidence and severity of COVID‐19 in HIV‐positive persons receiving antiretroviral therapy: a cohort study. Ann Intern Med. 2020;173(7):536‐541.32589451 10.7326/M 20-3689 PMC 7394316 · doi ↗ · pubmed ↗
- 7Martinez MA . Compounds with therapeutic potential against novel respiratory 2019 coronavirus. Antimicrob Agents Chemother. 2020;64(5):e 00399‐20.32152082 10.1128/AAC.00399-20PMC 7179632 · doi ↗ · pubmed ↗
- 8Ford N , Vitoria M , Rangaraj A , Norris SL , Calmy A , Doherty M . Systematic review of the efficacy and safety of antiretroviral drugs against SARS, MERS or COVID‐19: initial assessment. J Int AIDS Soc. 2020;23(4):e 25489.32293807 10.1002/jia 2.25489 PMC 7158851 · doi ↗ · pubmed ↗