Bilateral Cerebellar Hemispheric Ischemia in Cryptococcal Meningitis
Abdul Safi, John L Liu, Mittal Prajapati, Ram Narayan

TL;DR
A rare case of cerebellar ischemia in a patient with cryptococcal meningitis is described, highlighting vasculitis as a possible cause.
Contribution
This case report adds to the understanding of rare neurological complications in cryptococcal meningitis.
Findings
MRI revealed multiple small infarcts in the cerebellar hemisphere during treatment for cryptococcal meningitis.
Symptoms such as ataxia and facial droop were linked to bilateral cerebellar involvement.
Neurological improvement occurred after initiating treatment for suspected cryptococcal vasculitis.
Abstract
Bilateral cerebellar hemispheric ischemia is a rare complication of cryptococcal meningitis that may lead to significant neurologic morbidity. We present the case of a 70-year-old male with asplenia who developed progressive headaches, confusion, and fever. Neurological exam and brain MRI were unremarkable. Cerebrospinal fluid (CSF) showed lymphocytic pleocytosis with elevated protein and low glucose levels. CSF polymerase chain reaction (PCR) consisted of Cryptococcus neoformans, and the patient was started on induction therapy. On day 12, the patient reported altered mental status with worsening confusion and dizziness. MRI revealed multiple small infarcts of the posterolateral left cerebellar hemisphere. Transthoracic echocardiogram (TTE) and computed tomography angiography (CTA) of the head and neck were normal. By weeks 3 and 4, new symptoms developed, including ataxia, left-sided…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
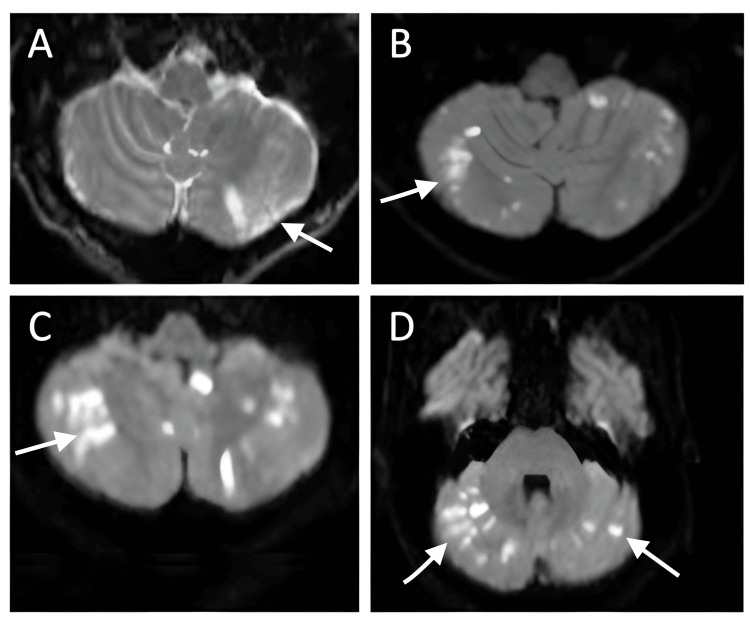 Figure 1
Figure 1| Parameter | Patient value | Reference/normal range |
| CSF opening pressure | 10 cm H2O | 6–20 cm H2O |
| CSF appearance | Clear, colorless | Clear, colorless |
| CSF WBC count | 54 /µL (60% lymphocytes) | <5 /µL |
| CSF glucose | <10 mg/dL | 40–70 mg/dL (≈2/3 serum) |
| CSF protein | 204 mg/dL | 15–45 mg/dL |
| CSF cryptococcal antigen | Positive, titer 1:2560 | Negative |
| CSF culture | Cryptococcus neoformans isolated | No growth |
| CSF Gram stain | Many polymorphonuclear leukocytes | No PMNs/organisms |
| BioFire ME panel | Positive for Cryptococcus neoformans | Negative |
| HIV Ag/Ab | Negative | Negative |
| West Nile virus serology (prior admission) | IgG positive/IgM negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Antifungal resistance and susceptibility · Nail Diseases and Treatments
Introduction
Cryptococcus neoformans is an encapsulated yeast that can cause life-threatening meningoencephalitis, most often in immunocompromised patients such as those with HIV/AIDS, organ transplants, or hematologic malignancies. In non-HIV, non-transplant patients, predisposing conditions include chronic immune dysfunction, such as asplenia, cirrhosis, or long-standing comorbidities [1,2]. Standard presenting features include headache, fever, and altered mental status [3]. Cerebrovascular complications occur in approximately 4-13% of patients and are usually due to infectious vasculopathy involving small- or medium-sized arteries [4]. These infarcts most often affect the basal ganglia, thalamus, and cerebellum and are associated with a poor prognosis [4].
Standard management consists of an induction phase with amphotericin B plus flucytosine, followed by consolidation therapy with fluconazole [5]. However, treatment may be complicated by immune reconstitution inflammatory syndrome (IRIS), characterized by paradoxical clinical worsening despite effective antifungal therapy, due to an exaggerated inflammatory response during immune recovery [6]. In selected cases with severe inflammatory complications, corticosteroids may be used. Corticosteroids are potent anti-inflammatory drugs that can help reduce the inflammation associated with IRIS, potentially improving patient outcomes. However, their use remains controversial due to potential side effects, including hyperglycemia, secondary infections, gastrointestinal bleeding, osteoporosis, mood or psychiatric changes, and delayed wound healing. Further research is needed to establish their efficacy in this context [7].
Case presentation
A 70-year-old male with a history of childhood splenectomy and chronic portal vein thrombosis presented with three months of progressively worsening daily headaches, waxing and waning confusion, decreased appetite, and low-grade fevers. His past medical history also included atrial fibrillation without anticoagulation and hyperlipidemia. He denied alcohol and tobacco use.
At the onset of these symptoms three months earlier, he was hospitalized with daily fevers and severe headaches. He was found to have a small, punctate infarct in the right middle cerebral artery (MCA) cortical branch territory. The lesion measured approximately 3-4 mm on MRI and was clinically silent; he had no hemiparesis, aphasia, or visual field deficits at that time. His atrial fibrillation was considered a potential embolic source; however, given the tiny infarct size, lack of recurrent episodes, and concurrent systemic infection, the etiology was felt more likely to be inflammatory or cryptogenic. He was not started on anticoagulation due to a low CHA_2_DS_2_-VASc score and perceived low risk of recurrence. He was discharged oriented and without residual neurological deficits. He also tested positive for West Nile Virus (positive IgG/negative IgM), consistent with chronic infection. At discharge, he was oriented and without significant cognitive or motor deficits.
On admission, he was febrile, tachycardic, and hypertensive, but alert and oriented without focal deficits. CT of the head and cervical spine was unremarkable. Still, brain MRI demonstrated a small, focal right MCA cortical branch infarct (Figure 1A), consistent with a subacute lesion and without associated neurological deficits. Lumbar puncture showed transparent CSF with an opening pressure of 10 cm H_2_O, lymphocytic pleocytosis (54 WBC/mL, 60% lymphocytes), glucose <10 mg/dL, and protein 204 mg/dL. BioFire FilmArray (BioFire Diagnostics, Salt Lake City, UT, USA) meningitis panel was positive for *Cryptococcus neoformans *(titer 1:2560) and confirmed by CSF culture. Gram stain showed many polymorphonuclear leukocytes. Other infectious work-up, including HIV, was negative. He began induction therapy with liposomal amphotericin B and flucytosine. Lab values are indicated in Table 1.
Axial diffusion weighted MRI scans in a 70-year-old male patient following the diagnosis of cryptococcal meningitis from initial presentation showing infarcts in the posterolateral cerebellar hemisphere (A). More numerous diffusion positive infarcts involving both cerebellar hemispheres are seen at 2 weeks (B), 3 weeks (C,D)
By day 12, he developed worsening confusion and dizziness. MRI revealed multiple small infarcts in the posterolateral left cerebellar hemisphere with leptomeningeal enhancement (Figure 1B). Echocardiography, CT angiogram of the brain and neck, and venous duplex studies excluded cardiac or vascular embolic sources.
After a gradual improvement in mental status and resolution of fevers, with stable vital signs and no new neurological deficits, he was discharged on day 19 to begin consolidation with fluconazole (800 mg daily for eight weeks). Thirty-six hours later, he was readmitted with new nausea, ataxia, left facial droop, diplopia, fatigue, diaphoresis, and dysphagia. He had sustained multiple falls due to an imbalance. Neurologic exam showed the patient was alert and oriented to person, place, and time. Cranial nerve exam showed left lower motor neuron facial weakness consistent with Bell’s palsy (CN VII), impaired abduction of the left eye suggestive of left CN VI palsy (correlating with pontine involvement), and absent gag reflex indicating involvement of CN IX/X. Pupils were equal, round, and reactive to light; no ptosis was noted. Extraocular movements were otherwise intact. Speech was mildly dysarthric. Motor strength was 5/5 in all extremities with no pronator drift. Sensation was intact to light touch and pinprick. Cerebellar testing revealed dysmetria on finger-to-nose on the left and a wide-based, ataxic gait with positive Romberg sign. Deep tendon reflexes were symmetric. The neck was supple but exhibited mild nuchal rigidity. MRI revealed new bilateral cerebellar infarcts and a right hippocampal infarct (not shown) (Figure 1C). Given the patient’s new neurologic deficits (ataxia, left facial droop, diplopia, and dysphagia), a repeat MRI was obtained shortly after the prior scan, which demonstrated increased diffusion-positive infarcts involving both cerebellar hemispheres (Figure 1D).
He was started on prednisone (10 mg daily, later increased to 60 mg with taper) for suspected IRIS-related vasculopathy. Trimethoprim-sulfamethoxazole (TMP-SMX) was added for Pneumocystis prophylaxis. Follow-up MRI showed improvement in cerebellar signal changes. His admission to rehabilitation for impaired mobility and speech was a turning point. Over the following four weeks, his cognition and mobility improved significantly, instilling hope for his eventual discharge home.
Discussion
This patient developed multifocal ischemic infarcts during treatment for cryptococcal meningitis, likely secondary to infectious vasculopathy. While cerebral infarctions are an uncommon complication, they are well described and may result from fungal invasion, vasculitis, or thrombotic occlusion [2]. In this case, involvement of both cerebellar hemispheres and the hippocampus was less common than the typical basal ganglia or thalamic distribution [2].
Negative vascular imaging and echocardiography, along with the infarct pattern, suggested an inflammatory rather than embolic mechanism. Continued progression despite antifungal therapy raised concern for IRIS, previously described in both HIV-positive and HIV-negative patients [3].
Adjunctive corticosteroids
In cryptococcal meningitis, corticosteroids are usually avoided early but may be indicated for: (1) new or worsening neurologic deficits with progression on imaging despite antifungal therapy; (2) evidence of IRIS or post-infectious inflammatory response syndrome (PIIRS) with negative cultures; or (3) severe CNS inflammation with mass effect or intracranial hypertension. Guidelines recommend prednisone-equivalent 0.5-1.0 mg/kg/day for two to six weeks with taper [1,4].
Host factors and risk
The patient's asplenia reflects chronic immune dysfunction, impairing opsonization and increasing fungal burden. Chronic portal vein thrombosis, while not a known risk factor, may have compounded ischemic risk in the setting of vasculitis. Other comorbidities such as cirrhosis, malignancy, or prior glucocorticoid exposure are associated with worse outcomes [1,4].
Long-term outcomes
Stroke complicating cryptococcal meningitis is linked with poor prognosis. In HIV-negative cohorts, infarctions increase the odds of poor outcomes more than twelvefold [5]. Survivors frequently suffer cognitive impairment, cranial neuropathies, or motor deficits, with 20-70% disability at follow-up [6]. Functional recovery may peak at 1 month but improve slowly with structured rehabilitation [6].
This patient improved after corticosteroid escalation, supporting a role for steroids in select cases. TMP-SMX was used to mitigate infection risk during prolonged immunosuppression.
Conclusions
Vasculopathic complications in cryptococcal meningitis are rare but may cause recurrent infarctions and disability. In patients with neurologic deterioration despite antifungal therapy and negative CSF cultures, IRIS or post-infectious inflammatory response syndrome (PIIRS) should be considered. A time-limited corticosteroid course can be practical in carefully selected cases. Early recognition, repeat imaging, and multidisciplinary management are critical to optimizing outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the Infectious Diseases Society of America Clin Infect Dis Perfect JR Dismukes WE Dromer F 2913225020102004748010.1086/649858 PMC 5826644 · doi ↗ · pubmed ↗
- 2Cryptococcosis in apparently immunocompetent patients QJM Lui G Lee N Ip M 1431519920061650498910.1093/qjmed/hcl 014 · doi ↗ · pubmed ↗
- 3Predictors of mortality and differences in clinical features among patients with Cryptococcosis according to immune status P Lo S One Brizendine KD Baddley JW Pappas PG 08201310.1371/journal.pone.0060431 PMC 360859223555970 · doi ↗ · pubmed ↗
- 4Cerebrovascular injury in cryptococcal meningitis Int J Stroke Mishra AK Arvind VH Muliyil D 57651320182842187810.1177/1747493017706240 · doi ↗ · pubmed ↗
- 5Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDSAIDS Park BJ Wannemuehler KA Marston BJ Govender N Pappas PG Chiller TM 5255302320091918267610.1097/QAD.0b 013e 328322 ffac · doi ↗ · pubmed ↗
- 6Cryptococcal immune reconstitution inflammatory syndrome in HIV-1-infected individuals: proposed clinical case definitions Lancet Infect Dis Haddow LJ Colebunders R Meintjes G 7918021020102102999310.1016/S 1473-3099(10)70170-5PMC 3026057 · doi ↗ · pubmed ↗
- 7Detrimental outcomes of unmasking cryptococcal meningitis with recent ART initiation Open Forum Infect Dis Rhein J Hullsiek KH Evans EE 05201810.1093/ofid/ofy 122PMC 608005230094292 · doi ↗ · pubmed ↗