Our First Experience in Using Anatomically Fitted Mesh Implant (Hertra™) During Lichtenstein Repair: A Case Report
Mekhaeel Shehata Fakhry Mekhaeel, Andrey Vitalevitch Protasov, Sameh M Salem, Olga Igorevna Mazurova, Abdelrahman Gomaa Zaky Aly Elshliby

TL;DR
The paper reports a successful hernia repair using a pre-shaped mesh implant, highlighting its benefits in a patient with multiple health conditions.
Contribution
Demonstrates the practical application of anatomically fitted mesh in Lichtenstein repair with a real patient case.
Findings
Anatomically fitted mesh implant was successfully used in Lichtenstein repair.
Procedure achieved concise surgical time and manageable postoperative complications.
Abstract
This article's main goal is to highlight the successful use of a pre-shaped, anatomically fitted mesh implant in Lichtenstein repair. We treated a 65-year-old male patient who experienced a left-sided hernial protrusion for six years, taking into account his concomitant comorbidities: secondary controlled hypertension, chronic superficial gastritis, and lumbar osteochondrosis with an old scar of appendectomy. Lichtenstein repair using a pre-shaped anatomically fitted polypropylene mesh implant with single-suture fixation was the chosen strategy for repair, achieving a concise surgical time along with initial and delayed onset of postoperative complications. Our objectives during the management of hernia were the use of anatomically fitted mesh implants, seamless fixation, and access to the advantages of anterior hernia repair. Here, we discuss the patient's condition, including medical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
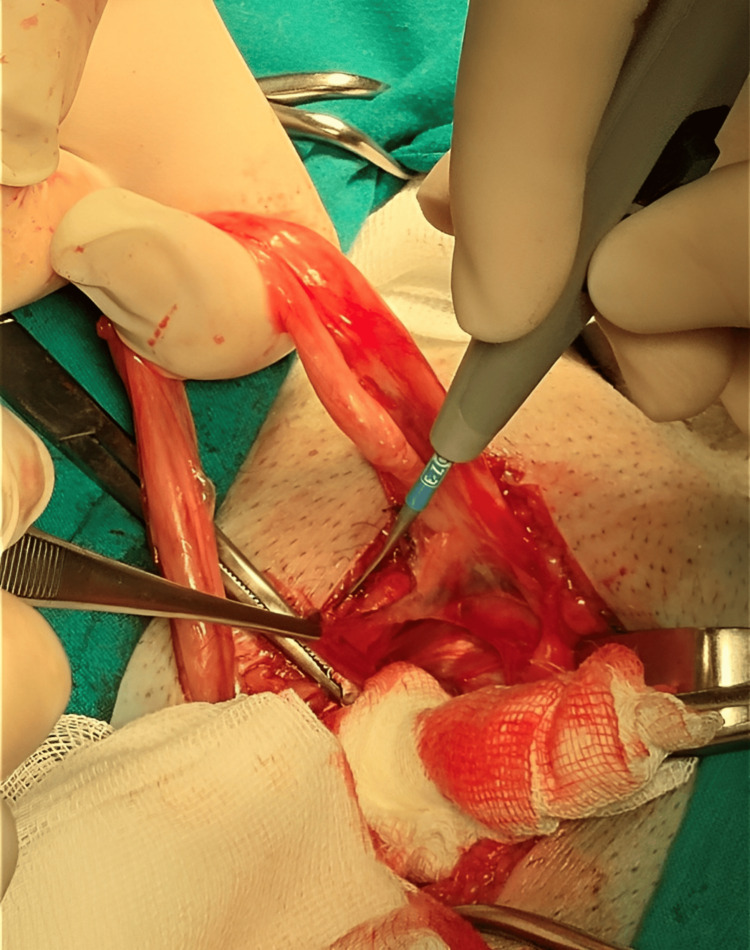 Figure 1
Figure 1 Figure 2
Figure 2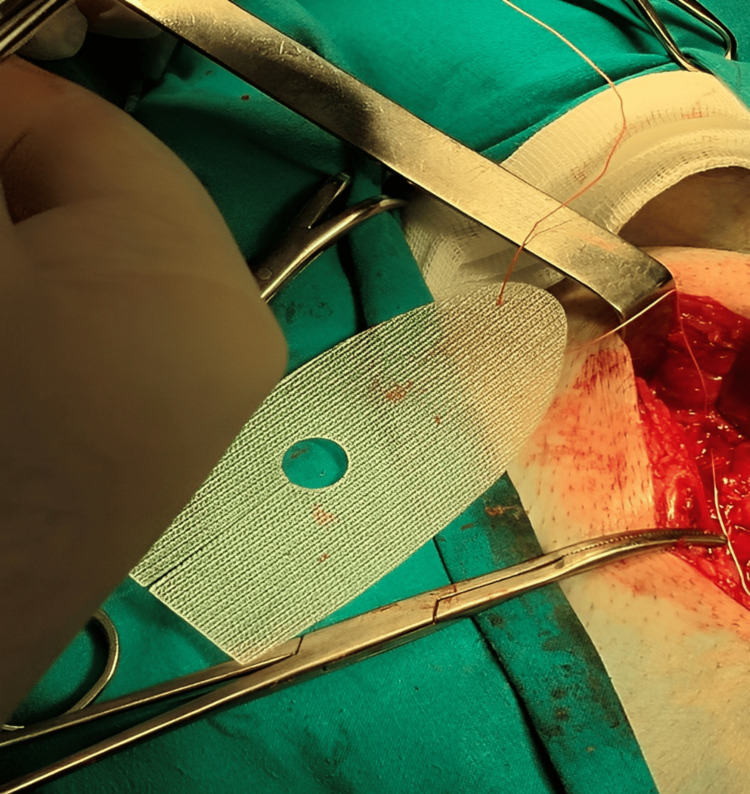 Figure 3
Figure 3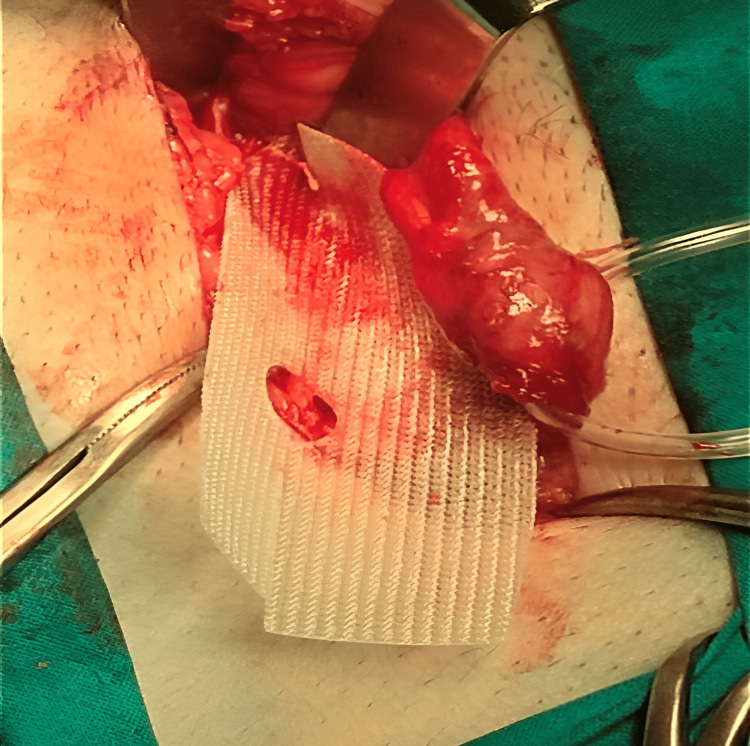 Figure 4
Figure 4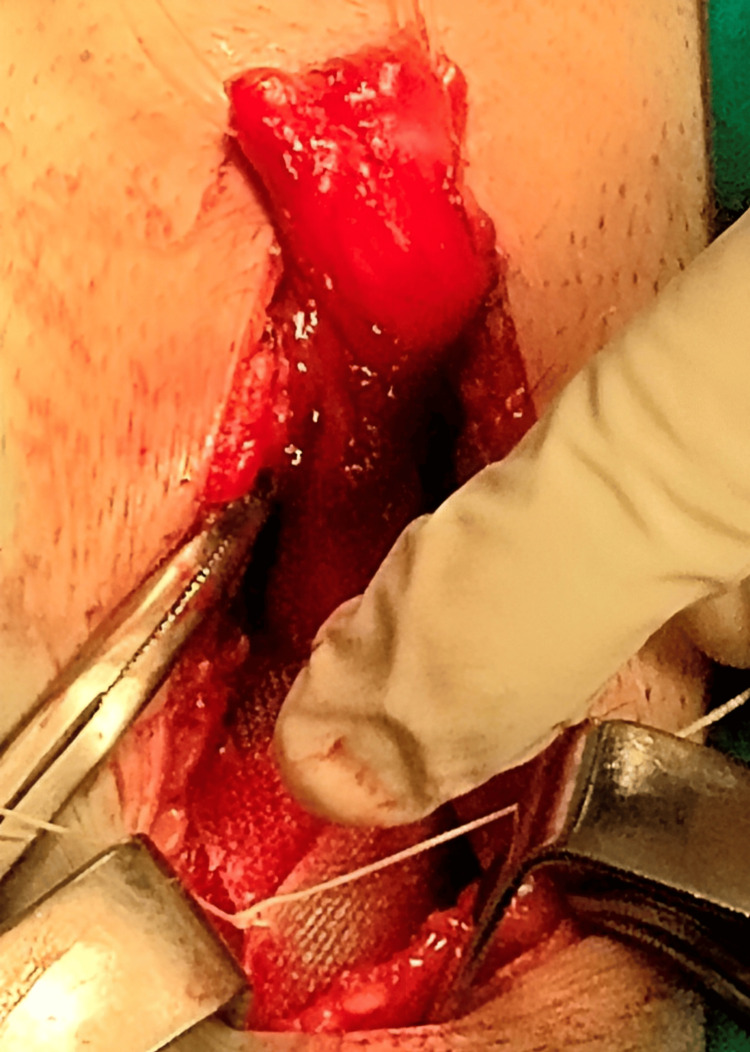 Figure 5
Figure 5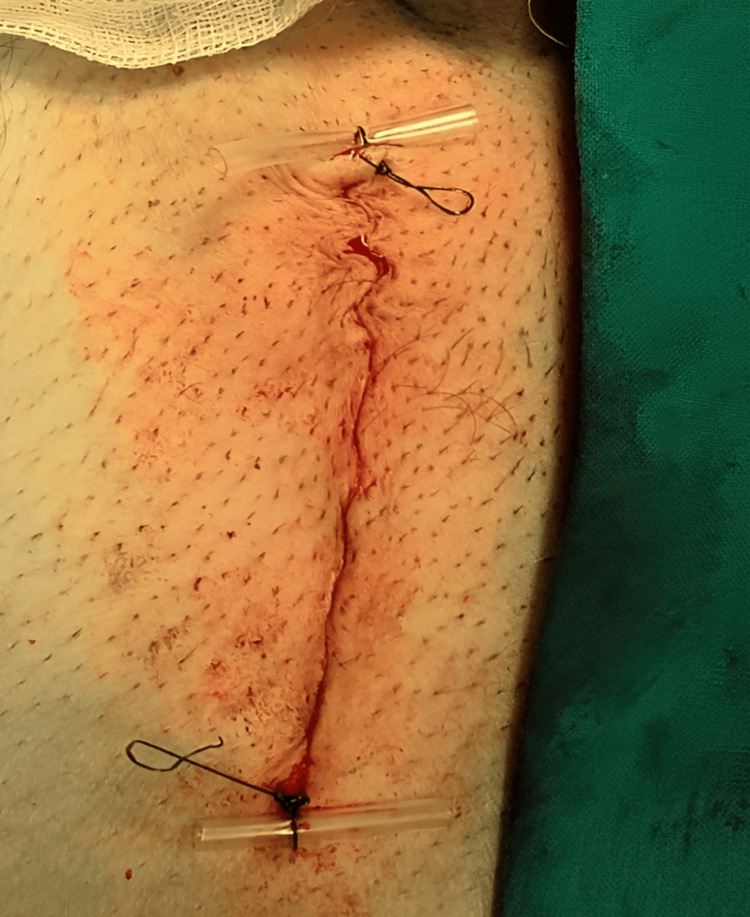 Figure 6
Figure 6| Complete Blood Count (CBC) | Patient’s value | Normal values |
| Red Blood Cell (RBC) Count | 4.9x109/mm3 | 4.2 to 6.9x109/mm3 |
| Hemoglobin (Hb) | 160 g/L | 130 to 180 g/L in males 120 to 160 g/L in females |
| Hematocrit (Hct) | 49% | 45% to 62% in males 37% to 48% in females |
| Mean Corpuscular Volume (MCV) | 85 micromillimeter | 80 to 100 micromillimeter |
| Mean Corpuscular Hemoglobin (MCH) | 30 pg/cell | 27 to 32 pg/cell |
| Mean Corpuscular Hemoglobin Concentration (MCHC) | 33% | 32% to 36% |
| White Blood Cell (WBC) Count | 6x109/mm3 | 4.3 to 11 x 109/mm3 |
| WBC differential | ||
| Neutrophils | 7x103/mm3 | 1.8 to 7.8x103/mm3 |
| Lymphocytes | 3.5x103/mm3 | 0.7 to 4.5x103/mm3 |
| Monocytes | 0.5x103/mm3 | 0.1 to 1.0 x 103/mm3 |
| Eosinophils | 0.1 x103/mm3 | 0 to 0.4 x103/mm3 |
| Basophils | 0 | 0 to 0.2 x 103/mm3 |
| Platelet Count | 256x109/mm3 | 150 to 400 x 109/mm3 |
| Reticulocytes | 0.049x109/mm3 | 1% of total RBC count |
| Coagulation Profile | Patient’s value | Normal values |
| Platelet Count | 256 x109/L | 150 to 400 x109/L |
| Prothrombin Time (PT) | 15 s | 11 to 24 s |
| International Normalized Ratio (INR) | 0.9 | 0.9 to 1.2 |
| Activated Partial Thromboplastin Time (aPTT) | 25 s | 22 to 35 s |
| Hepatic function tests | Patient’s value | Normal values |
| PT/INR | 1 | 0.9 to 1.2 |
| Serum Albumin | 4.0 g/dL | 3.5 to 5.0 g/dL |
| Serum Bilirubin (total) | 0.5 mg/dL | 0.1 to 1.0 mg/dL |
| Serum Bilirubin (direct) | 0.3 mg/dL | 0 to 0.3 mg/dL |
| Alanine aminotransferase (ALT) | 11 U/L | 8 to 20 U/L |
| Aspartate aminotransferase (AST) | 8 U/L | 8 to 20 U/L |
| Alkaline phosphatase (ALP) | 73 U/L | 35 to 100 U/L |
| Gamma-glutamyl transferase (GGT) | 3 U/L | 0 to 30 U/L |
| Renal function tests | Patient’s value | Normal values |
| Blood urea nitrogen (BUN) | 15 mg/dL | 7-20 mg/dL |
| Serum creatinine | 0.6 mg/dL | 0.6-1.2 mg/dL |
| Estimated Glomerular Filtration Rate | 100 mL/min/1.73 m2 | >90 mL/min/1.73 m2 |
| Albumin to creatinine ratio (ACR) | 20 mg/g | <30 mg/g |
| Serology for HBV, HCV | Patient’s value | Normal values |
| HBsAg | Negative | Negative |
| Anti-HBc | Negative | Negative |
| Anti-HBs | Negative | Negative |
| Serology for HIV | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnatomy and Medical Technology · Hernia repair and management · Surgical Sutures and Adhesives
Introduction
The average cost of a hernioplasty procedure in the United States is approximately 12,500, and that the global incidence of hernias has been steadily increasing over the past 30 years, approaching 33 million cases annually [[1](#REF1)]. The global market for hernia repair is expected to reach 6.3 billion in a few years [2]. Given the increasing incidence of hernia and cost of hernia repair, we aimed to improve the results of the gold standard technique of anterior hernia repair by Lichtenstein technique [3].
Polypropylene (PP), the most widely used material for the fabrication of surgical meshes [4], is a non-absorbable, electrostatically neutral, highly hygroscopic, non-polar material with high tensile strength, available as monolayers or multi-layers, coated or uncoated, and in heavy or light forms [5]. The manufacturing technique significantly influences the mesh properties. Traditional knitting creates meshes with mobile joint points, which can lead to high, localized stress concentrations at suture fixation sites, potentially contributing to tissue trauma and post-operative pain. In contrast, advanced techniques like fuse deposition modeling (FDM) 3D printing allow for the creation of pre-formed, anatomically fitted meshes with a more uniform structure [6]. Although this may result in a different tensile profile compared to some knitted meshes, it enables a design that distributes mechanical load more effectively across the implant and tissue interface. This reduces shear forces and pressure on the inguinal nerves, thereby mitigating a major cause of chronic pain. The anatomic design also facilitates quicker and easier implantation, reducing operative time [7].
The use of pre-shaped surgical meshes is preferable to non-pre-shaped fixed sutures due to reduced surgical time, lower post-operative seroma and hematoma formation and urinary retention and, even more importantly, reduced recurrence rates [8,9]. Various hypotheses link the pathogenesis of early post-operative inguinal pain not only to surgical causes but also to tissue trauma from surgical site preparation, mesh inflammatory reactions and mesh fixation, which may explain the less-induced post-operative pain caused by the use of self-adhesive meshes in contrast to the suture.
A significant consideration is cost-effectiveness. While anatomically fitted, pre-formed meshes command a higher initial price than conventional flat polypropylene meshes, analyses show that they provide a superior long-term economic benefit [10,11]. The key drivers of this advantage are: (1) intraoperative efficiency: the pre-formed design eliminates the need for extensive trimming and minimizes the number of sutures required for fixation, significantly reducing operative time and associated costs and (2) reduced complication burden: by promoting better biomechanical integration and reducing nerve entrapment and inflammatory response, these meshes lead to substantially lower the rates of chronic pain, seroma formation, and recurrence. The avoidance of diagnosing and managing these complications results in major cost savings for the healthcare system post-discharge [10,11].
Case presentation
A 65-year-old male patient was admitted to the outpatient clinic of the clinical hospital No. 85 of the Federal Medico-Biological Agency (FMBA) in Moscow, Russian Federation, complaining of a hernia-bearing disease, gradually increasing in size, in the left groin area for six years. No signs of obstruction or any other hernial complications were reported by the patient. During history taking, the patient clarified that he has a secondary controlled hypertension and his targeted blood pressure level was less than 130/80 mmHg, chronic superficial gastritis, lumbar osteochondrosis, and appendectomy performed by open approach more than 40 years ago. There was no history of allergy.
The patient was alert, comfortable in bed with a level of consciousness on the Glasgow scale of 15/15. The skin had a normal appearance, without pathological rashes and cyanosis. No edema was detected. Visible mucous membranes were pink without pathological rashes. Lymph nodes were neither palpable nor enlarged. An assessment of the musculoskeletal system showed a normal musculature without pathological changes. The patient's height was 170 cm and body weight 80 kg, resulting in a body mass index (BMI) of 27.7 kg/m^2^.
A physical assessment was made. On reviewing the respiratory system, it was found that the shape of the chest was normal and it participates in breathing evenly. Palpation was painless and the percussive sound was pulmonary upon lung auscultation. Respiration was performed evenly throughout the thoracic cavity. Without any wheezing, breathing through the nose was free. Auscultation of the cardiac tones was clear and rhythmic. Abnormal noises were not detected.
The palpation of abdominal organs showed that the liver was along the edge of the costal margins, painless, and not palpable. The gallbladder and spleen were not palpable. Symptoms of peritoneal irritation were not determined. The assessment of the nature of the stools and the frequency of defecation showed that the stool was normal, without pathological inclusions, and passed one to two times a day. No pathological changes were detected in the genitourinary system. Kidneys were not palpable and painless. An assessment of the nature of urination showed that it was free and painless. On assessing vital body signs, body temperature was 36.6°C, heart rate 74 beats/min, blood pressure 125/85 mmHg and respiratory rate 17/min. On local examination, the hernial protrusion was found in the left inguinal region, freely adjustable into the abdominal cavity, painless with normal covering skin. The outer inguinal ring was up to 2.5 cm.
The results of investigations are presented. The complete blood count results are shown in Table 1, the coagulation profile is presented in Table 2, hepato-renal function tests as displayed in Tables 3, 4, and serology for hepatitis B virus (HBV), hepatitis C virus (HCV) and human immunodeficiency virus (HIV) is shown in Table 5.
Abdomino-pelvic ultrasonographic examination revealed a left inguinal herniation with a hernia sac dimensions of 8x7 cm and width of the outer inguinal ring up to 2.5 cm. The content of hernia was peritoneum. There were no enlarged abdominopelvic organs and no specific abdominal lymphadenopathy. Ascites were not present. ECG was normal. Arterial oxygen saturation was 99% and glomerular filtration rate (GFR) was 53.056. After maintaining controlled blood pressure and obtaining a written informed consent for the operation, the patient was planned for an elective inguinal hernioplasty by Liechtenstein using Hertra™ (Herniamesh, Turin, Italy) mesh implant with spinal anesthesia.
Cleaning of the inguinal region was performed for two minutes, followed by a 4-cm incision along the inguinal ligament following Langer’s line. For averting postoperative pain, edema, and ecchymosis, abdominal retractors were applied for the prevention of over-retraction. Layer-by-layer dissection was achieved successfully, avoiding injury to the ilioinguinal, iliohypogastric, and genital branch of the genitofemoral nerves through their identification. The ilioinguinal nerve was preserved by careful dissection of the external oblique aponeurosis starting from the external ring along its fibers. Furthermore, local anesthetic was infiltrated around the ilioinguinal nerve and the surgical field lateral to the external oblique aponeurosis to provide pre-emptive analgesia. Herniotomy with high dissection of the hernia sac and complete reduction of the hernial contents back into the abdominal cavity was done as shown in Figure 1. The spermatic cord and the hernia sac were encircled using a Penrose for preserving the genital branch of the genitofemoral nerve as seen in Figure 2.
Dissection of the hernial sac.
Encircling the spermatic cord using a Penrose.
A semirigid pre-shaped left-sided polypropylene monofilamentous Hertra™ 2 mesh implant, measuring 4.5x10 cm with an eccentric eye and with an anatomically fitted position for the passage of the spermatic cord, was used for repair as seen in Figure 3. No fixation was needed except for a single suture at the pubic tubercle using Dexon zero suture as shown in Figure 4.
Hertra™ 2 mesh implant.
Single-suture fixation to the pubic tubercle.
The tails of the pre-splitted mesh encircled the spermatic cord and the internal inguinal ring, followed by securing both ends by a single nonabsorbable suture as seen in Figure 5. The external oblique aponeurosis was reapproximated using absorbable sutures. The wound was closed layer by layer till skin, which was closed by subcuticular suture with upper and lower markers for easier identification of the ends during removal as seen in Figure 6.
Securing the mesh tails using a single nonabsorbable suture at the level of the internal inguinal nerve.
Skin closure with upper and lower markers.
The operative time was approximately 30 minutes. During the postoperative period, acute postoperative pain decreased gradually. The surgical dressings were done once daily for a week. During the short-term follow-up, the patient showed no complications, no chronic postoperative pain, no foreign body sensation, and no seroma. There was no recurrence. The follow-up for the first two years was without any complications nor recurrence.
Discussion
Lichtenstein was performed using semi-rigid polypropylene monofilament mesh Hertra™ 2 (Hertra™1 and Hertra™ 2 are pre-adapted for masculine inguinal canal), while Hertra™ 2A is pre-adapted for feminine inguinal canal geometry with acentric opening with average pore size of 741 microns (min. 389 microns, max. 1083 microns), density of 177 g/m^2^ and sterilized by ethylene oxide [12]. This strategy improved the patient’s surgical output in our experience.
The biologic response to hernia prostheses has a major influence on the operative results and patient’s compliance as well, affecting the compatibility between both the inguinal canal and implanted mesh geometries; flat conventional hernia meshes, fixated with sutures or tacks, induce a poor-quality fibrotic ingrowth, resulting in mesh shrinkage. Furthermore, uncontrolled development of a scar plate can impair movement and may incorporate the ilioinguinal, iliohypogastric, and genital branch of the genitofemoral nerves, resulting in postoperative neuralgia [13]. On the contrary, preformed meshes possess a dynamic responsive behavior as they are designed to adapt the geometry of the inguinal canal; during inguinal movements, preformed meshes induce enhanced biological response with ingrowth of newly formed connective tissue, muscle fibers, and nerves, supporting the contextual development of newly formed arteries and veins, thus inducing the healing process as well [14].
Finally, our patient gained all the above-mentioned benefits, reduced operative time, and absence of complications during both postoperative hospital stays and short-term follow-up periods. Moreover, the patient is following up in the outpatient clinic every six months on a five-year schedule.
Conclusions
This initial experience with the Hertra™ anatomically contoured, three-dimensional mesh in a Lichtenstein hernioplasty demonstrated notable procedural efficiency and excellent short-term outcomes. The key observation was the mesh's pre-formed design, which facilitated a swift and intuitive implantation process, negating the need for intraoperative trimming and minimizing suture fixation to a single point at the pubic tubercle. This contributed to an operative time of approximately 30 minutes.
In this single case, the patient's postoperative course was unremarkable, with no observed complications such as seroma, chronic pain, or recurrence at the two-year follow-up. These outcomes are consistent with the proposed advantages of such devices, which aim to reduce technical variability, promote physiological force distribution, and minimize nerve irritation.
While these preliminary results are promising, they represent a proof-of-concept from a single instance. The higher initial cost of a pre-formed mesh may be offset by potential gains in operating room efficiency and a reduced complication burden; however, this requires formal health-economic analysis. Therefore, based on this favorable initial experience, we conclude that the Hertra™ mesh is a viable and promising option for open inguinal hernia repair. We strongly recommend and intend to pursue further comparative studies with long-term follow-up to objectively evaluate its advantages over conventional flat meshes in terms of chronic pain, patient satisfaction, and overall cost-effectiveness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1AI-based evaluation of polypropylene and polyester meshes in Lichtenstein hernia repair Archiv Euromedica Mekhaeel M Kazem R Protasov A Salem S Al Tekreeti WK Mohareb A 2152025 https://journal-archiveuromedica.eu/archiv-euromedica-02-2025/8-AI-Based-Evaluation-of-Polypropylene-and-Polyester-Meshes-in-Lichtenstein-Hernia-Repair.html
- 2Prosthetic meshes for hernia repair: state of art, classification, biomaterials, antimicrobial approaches, and fabrication methods J Biomed Mater Res A Serrano-ArocaÁ Pous-Serrano S 2695271910920213402170510.1002/jbm.a.37238 · doi ↗ · pubmed ↗
- 3Lichtenstein technique for inguinal hernia repair: ten recommendations to optimize surgical outcomes Hernia Messias BA Nicastro RG Mocchetti ER Waisberg J Roll S Junior MA 146714762820243890035510.1007/s 10029-024-03094-w PMC 11297121 · doi ↗ · pubmed ↗
- 4A review of recent developments of polypropylene surgical mesh for hernia repair Open Nano Saha T Wang X Padhye R Houshyar S 10004672022 https://www.sciencedirect.com/science/article/pii/S 2352952022000093?via%3Dihub
- 5Development of mesh implants materials through history regarding their characteristics. Review study International Journal of Medical Reviews and Case Reports Mekhaeel MD Salem SM Protasov AV 41082024
- 6The choice of the optimal mesh implant for hernioplasty operations depending on the properties of mesh implants RUDN Journal of Medicine Protasov A Mekhaeel M Salem S 499507282024 https://journals.rudn.ru/medicine/article/view/42013
- 73D Printed vs. commercial polypropylene surgical meshes: a comparative analysis of tensile strength 2021 International Conference on e-Health and Bioengineering (EHB), Iasi, Romania Galvan-Chacon V Patrocinio D Duarte-Leon M Pagador JB Margallo FM 142021 https://ieeexplore.ieee.org/document/9657708
- 8Comparison of three-dimensional mesh (3D mesh) without fixation versus polypropylene mesh with fixation in patients of inguinal hernia undergoing totally extraperitoneal repair Laparoscopic Endoscopic Surgical Science Omarov N Huseynov E Özocak AB 5056312024