Idiopathic Recurrent Serositis: A Multispecialty Challenge Resolved With Colchicine
Shivashankari Dakshinamoorthy, Renuka Renuka, Irfan Tariq, Deepak Albana

TL;DR
A rare condition causing recurring inflammation of body membranes was successfully treated with colchicine after extensive diagnostic workup failed to find other causes.
Contribution
Demonstrates successful use of colchicine for idiopathic recurrent serositis after multidisciplinary investigation ruled out other causes.
Findings
Colchicine provided durable remission of recurrent serositis symptoms in a patient with no identifiable underlying cause.
Multidisciplinary evaluation including imaging and biopsies failed to identify malignancy, infection, or autoimmune disease.
Treatment with colchicine and NSAIDs led to resolution of pleural and peritoneal effusions and sustained remission.
Abstract
Idiopathic recurrent serositis (IRS) is a rare and diagnostically challenging condition characterised by recurrent inflammation of serous membranes, occurring without any identifiable infection, malignancy, or autoimmune cause. We present the case of a 32-year-old female who was initially admitted with dyspnoea and a right pleural effusion. Pleural fluid analysis revealed an exudate with negative microbiology, cytology, and tuberculosis testing, and she was treated empirically with antibiotics. Over the following months, the patient developed recurrent symptoms, including progressive abdominal distension due to gross ascites and a small pericardial effusion. An extensive multidisciplinary evaluation involving infectious disease, gynecology, respiratory medicine, and rheumatology yielded no definitive findings. Cross-sectional imaging and positron emission tomography (PET) excluded…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
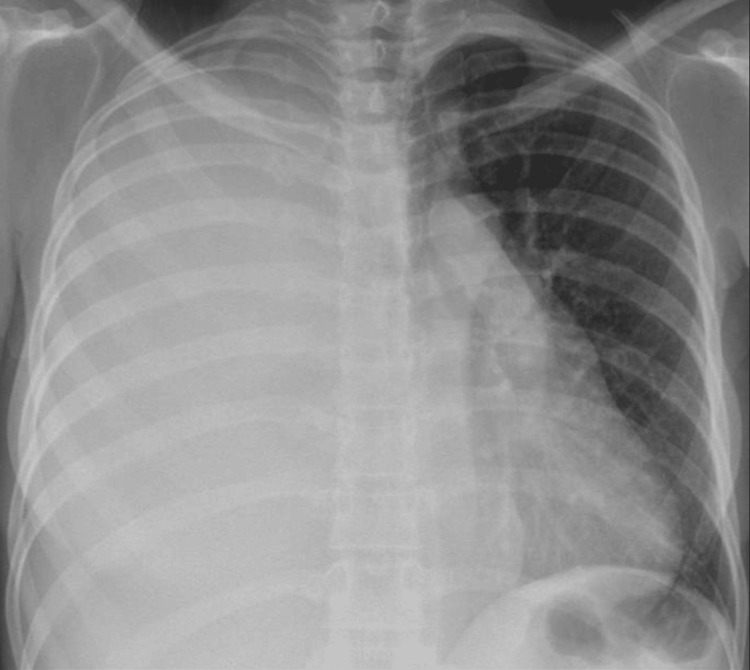 Figure 1
Figure 1 Figure 2
Figure 2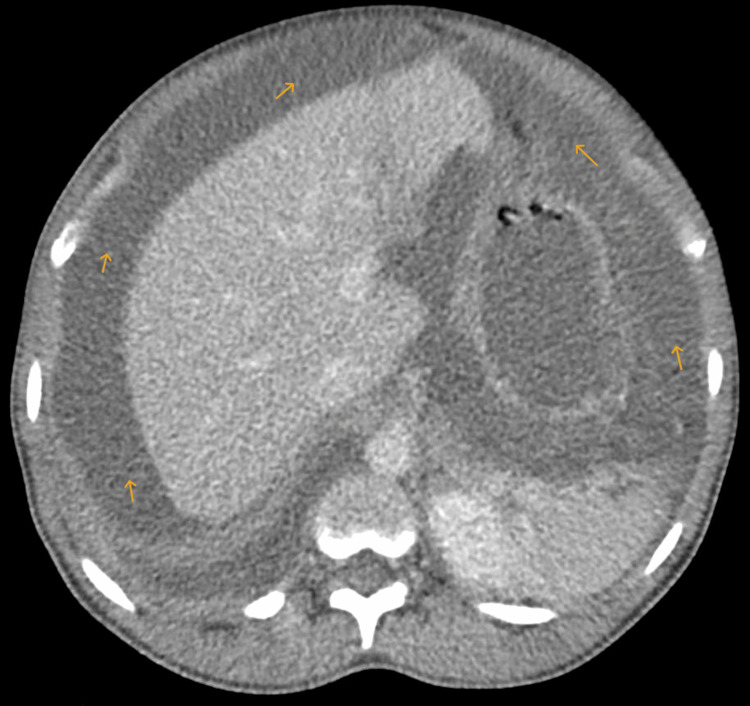 Figure 3
Figure 3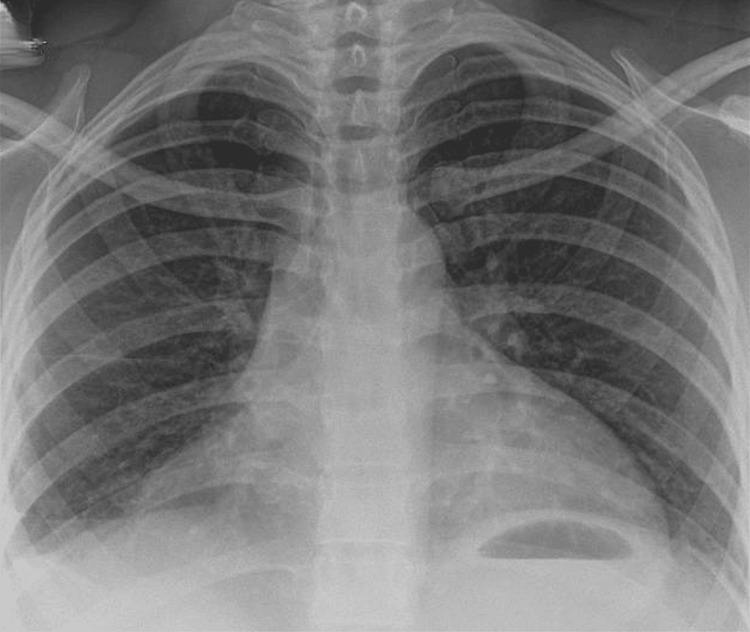 Figure 4
Figure 4| Investigation | Result | Reference value |
| Full blood count - WBC | 6.75 (normal) | 3.00-10.90 x 109/L |
| CRP | 126 (high) | 0-5 mg/L |
| Serum lactate dehydrogenase | 249 (slightly raised) | 125-220 U/L |
| Serum protein | 71 (normal) | 60-80 /L |
| Autoimmune analysis | ||
| ANA | Negative | |
| ANCA | Negative | |
| LKM antibody | Negative | |
| ASMA | Negative | |
| AMA | Negative | |
| Mitochondrial antibody | Negative | |
| Smooth muscle antibody | Negative | |
| Immunoglobulin G | 13.85 | 6.00-16.00 g/L |
| Immunoglobulin A | 1.78 | 0.80-2.80 g/L |
| Immunoglobulin M | 1.5 | 0.50-1.90 g/L |
| dsDNA antibody | <0.6 | 0.6-9.9 IU/ml |
| IgG cardiolipin antibody | 0.9 | 0.5-23.8 GPLU/ml |
| IgM cardiolipin antibody | 2.8 | 0.9-29.9 MPLU/ml |
| Beta2 glycoprotein G | 1 | 0.8-17.7 U/ml |
| Beta2 glycoprotein M | <2.4 | 2.4-5.7 U/ml |
| Complement C3 | 1.58 | 0.75-1.65 g/L |
| Complement C4 | 0.47 | 0.14-0.54 g/L |
| Electrophoresis | No paraprotein band seen | |
| Infectious diseases screen | ||
| HIV 1 and 2 antigen/antibody | Negative | |
| Hepatitis B HBsAg | Negative | |
| Hepatitis C antibody | Negative | |
| T-SPOT TB | Negative | |
| SARS-CoV-2 RNA | Negative | |
| Respiratory syncytial virus RNA | Negative | |
| Influenza A virus RNA | Negative | |
| Influenza B virus RNA | Negative | |
| Parainfluenza virus RNA | Negative | |
| Rhinovirus RNA | Negative | |
| Human metapneumovirus RNA | Negative | |
| Adenovirus DNA | Negative | |
| Blood cultures | Negative | |
| Pleural fluid - exudate | Yes | |
| Pleural fluid - cytology | Normal cytology | |
| Pleural fluid - microbiology | Acinetobacter species (environmental contaminant) | |
| Ascitic fluid - microbiology | No organisms | |
| Fluid albumin | 21 | >11 g/L (depends on SAAG) |
| Fluid LDH | 726 (high) | 225–300 U/L |
| Fluid total protein | 42 (high) | <25 g/L (transudate)/>25 g/L (exudate) |
| Microscopy | Mild prominence of lymphocytes. No malignant cells seen | |
| SAAG | 0.5 | <1.1 g/dL (exudative type) |
| TB analysis | ||
| IGRA testing | Negative | |
| Sputum cultures | Negative | |
| Acid-fast bacilli | Negative | |
| TB-PCR | Negative | |
| Mycobacteria | Negative | |
| Alpha fetoprotein | <1.7 | <7.4 ku/L |
| Imaging analysis | ||
| CT TAP with contrast | Right-sided pleural effusion, gross ascites, bulky uterine fibroids, adnexal mass | |
| PET CT scan | No evidence of malignancy/infection/structural cause for effusions | |
| Echocardiography | Small pericardial effusion, EF 60% | |
| Peritoneal biopsy | No granulomatous inflammation. No TB or malignancy | |
| VATS | Scar tissue, no atypia or malignancy | |
| R413 gene analysis and amyloidosis testing | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Viral Infections and Immunology Research · Eosinophilic Disorders and Syndromes
Introduction
Recurrent serositis, encompassing relapsing pleuritis, pericarditis, or ascites, is a significant diagnostic and therapeutic challenge. As reported by Adler et al., recurrence is particularly well described in pericarditis, affecting 15-30% of patients after an initial episode, with some cohorts reporting rates up to 50% [1]. Its pathophysiology is heterogeneous, which includes infection, malignancy, autoimmune-complex disease, and autoinflammatory syndromes [2]. Familial Mediterranean fever (FMF) and tumour necrosis factor receptor-associated periodic syndrome (TRAPS) illustrate the role of Interleukin-1 (IL-1)-mediated innate immune dysregulation [3,4]. Recent mechanistic insights further substantiate the link between psychological or physiological stress and autoinflammatory flares. Skendros et al. demonstrated that stress-induced upregulation of regulated in development and DNA damage responses 1 (REDD1) activates IL-1β-mediated inflammatory pathways in FMF, promoting autophagy-driven neutrophil extracellular trap formation and precipitating attacks [3]. This provides a biological basis for the observed association between emotional stress and clinical relapses in FMF and related autoinflammatory syndromes.
Diagnosis follows a stepwise approach involving fluid analysis, cytology and cultures, imaging studies, and autoimmune serological testing. As noted by Caterson et al., the diagnosis of autoinflammatory syndromes has become increasingly individualised with the growing accessibility of gene panel testing. [5]. Historically, only a limited number of syndromic diseases were recognised; however, this number has expanded in recent years. The ability to test every suspected case remains limited in most hospitals, with specialist centres being far and few [5]. The main concern, however, is the lack of testing sensitivity. Pleural cytology has a mean sensitivity of ~60% for malignancy detection. Typically, the metastatic carcinoma and TB diagnostics may be inconclusive, necessitating repeat sampling or biopsy when suspicion persists [6,7]. Persistent barriers include delayed recognition, restricted test sensitivity, and limited global access to biologics [5].
Although combined therapy with colchicine and nonsteroidal anti-inflammatory drugs (NSAIDs) is the first-line treatment for Idiopathic recurrent serositis (IRS), previous studies have indicated that colchicine monotherapy may serve as an effective alternative to lower the risk of recurrence [4,6]. In this context, we present a unique case of a patient who, after months of recurrent symptoms and multiple specialist evaluations, was ultimately diagnosed with an autoinflammatory syndrome that responded well to colchicine therapy.
Case presentation
A 32-year-old female with no significant past medical history presented with progressive shortness of breath. She had experienced similar symptoms one year earlier while in Nigeria, where she was empirically treated for a lower respiratory tract infection. Discharge notes from that evaluation provided limited clinical details, noting only a diagnosis of a small pleural effusion, likely secondary to infection. During her admission under our care, the initial chest X-ray showed a massive right-sided pleural effusion (Figure 1), which was aspirated. Investigations of pleural fluid, including microbiology, did not reveal any organisms or growth. The biochemistry findings had confirmed the exudative nature of the fluid, and cytology revealed no malignant cells on the aspirate. TB analysis of the fluid culture and polymerase chain reaction (PCR) tests were negative. Ziehl-Neelsen staining was negative for acid-fast bacilli. She was discharged on antibiotic therapy with a plan to repeat a chest X-ray in six weeks, which reportedly returned normal. She was also scheduled for follow-up at the chest clinic under the care of the Respiratory team.
Chest X-ray on first presentation revealing a massive right-sided pleural effusion resulting in complete opacification of the right hemithorax and leftward mediastinal shift
Eight months later, the patient re-presented with abdominal distension, discomfort, and shifting dullness. She was afebrile and had no orogenital lesions, rashes, or any visual symptoms or signs. Blood tests showed an elevated C-reactive protein (126 mg/L) with otherwise normal renal function and full blood count. Contrast-enhanced CT of the thorax, abdomen, and pelvis (Figures 2, 3) demonstrated the recurrence of a massive right pleural effusion resulting in near complete collapse of the right lung and mediastinal shift, in addition to gross ascites, bulky uterine fibroids, and a left adnexal soft tissue mass with a cystic component.
CT scan showing a large volume right-sided pleural effusion (yellow arrows)CT: computed tomography
CT scan showing accumulation of ascitic fluid in the peritoneal cavity (yellow arrows)CT: computed tomography
Extensive serological testing, including antinuclear antibodies (ANA), antineutrophil cytoplasmic antibodies (ANCA), anti-liver/kidney microsomal (anti-LKM), anti-smooth muscle antibody (ASMA), antimitochondrial antibody (AMA), complement levels, dsDNA, immunoglobulins, electrophoresis, HIV, hepatitis, and extended viral panels, was unremarkable (Table 1). A subsequent positron emission tomography-computed tomography (PET-CT) scan showed no evidence of metabolically active malignancy, infection, or any structural cause for the ascites or pleural effusion. However, moderate uptake was noted in residual thymic tissue, likely representing benign thymic hyperplasia. Overall, these findings raised the possibility of an underlying connective tissue disorder
The pleural fluid profile and cytological findings were identical to those observed during the prior presentation, showing no new diagnostic features. Ascitic fluid analyses confirmed an exudative effusion (serum-ascites albumin gradient (SAAG) <1.1) with lymphocyte predominance and negative cytology. Fluid cultures grew Acinetobacter baumannii and Mycobacterium chimaera, both of which are considered environmental contaminants. Tuberculosis PCR and interferon-gamma release assay (IGRA) were negative. Gynaecological evaluation attributed pelvic findings to benign fibroids, unrelated to the patient's presentation.
Video-assisted thoracoscopic surgery (VATS) pleural biopsies demonstrated nonspecific chronic inflammation without evidence of malignancy or infection. Broad-spectrum antibiotics (clarithromycin and ciprofloxacin) were administered after *Pseudomonas *was isolated from chest drain fluid, although repeat VATS biopsy remained negative on histology and cultures. Despite the persistence of pleural effusion and ascites, the patient remained clinically stable with no systemic symptoms. Her only concerns were abdominal distension causing discomfort and a sense of generalised fatigue. She remained haemodynamically stable. Peritoneal biopsies revealed no malignant cells, granulomatous inflammation, or mycobacterial infection with negative PCR and cultures for tuberculosis.
After a multidisciplinary review, referral to a national amyloidosis and autoinflammatory disease service in London led to a working diagnosis of IRS, and genetic testing for a relevant autoinflammatory mutation was initiated. R413 autoinflammatory disorders testing was negative, alongside a negative screen for hereditary amyloidosis testing.
Colchicine prophylaxis was started at a dose of 500 mcg daily and gradually increased to 1.5-2.0 mg. For acute episodes, ibuprofen 200 mg was prescribed, in line with the approach described by Roy et al. [6]. The patient achieved marked clinical improvement, with complete resolution of ascites and pleural effusion (Figure 4), and has remained symptom-free in sustained remission at follow-up, having returned to her full daily activities.
Chest X-ray showing resolution of pleural effusion following colchicine therapy
Discussion
IRS is characterised by inflammation of the serous membranes without an identifiable underlying trigger [6]. It is generally considered autoinflammatory, arising from dysregulated innate immune responses. The condition presents a significant diagnostic challenge due to nonspecific clinical features and a broad differential, necessitating the exclusion of infectious, malignant, and autoimmune causes [2,4]. In our patient, extensive investigations including imaging, fluid analyses, biopsies, and comprehensive serological testing ruled out secondary aetiologies. As previously reported by Roy et al., persistently elevated inflammatory markers alongside recurrent pleural, pericardial, and peritoneal effusions in a haemodynamically stable patient pointed towards a non-infective, inflammatory process [6].
We conducted a literature review using the databases MEDLINE, Embase, and PubMed to examine the aetiology of serositis and its association with autoinflammatory syndromes. Among more than 20 well-characterised seronegative conditions, serositis is a common feature, occurring in disorders such as FMF, TRAPS, and the rarer adenosine deaminase 2 deficiency (DADA2) and NLRP2 spectrum disorders [3,8]. As reported by Rech et al., the average time to diagnosis was three years in children and adolescents, compared to 14 years in adults [8]. Before the correct diagnosis of an autoinflammatory disease was established, many patients had received multiple misdiagnoses, including psychosomatic disorders [2]. Management typically involves corticosteroids or colchicine, often combined with conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs) and biologics such as adalimumab, anakinra, or tocilizumab [9]. In navigating treatment options for rare rheumatic diseases, clinicians frequently rely on existing literature and available case reports.
In our case, colchicine was initiated and titrated to 1.5-2 mg daily, alongside NSAIDs for acute episodes, resulting in marked clinical improvement and sustained remission [6]. Steroids may be employed to reduce inflammation and prevent effusions; however, prolonged use can lead to substantial side effects. In contrast, colchicine and NSAIDs have proven effective in this case, leading to sustained resolution of symptoms and signs to date. Massaro et al. previously demonstrated that colchicine effectively reduces inflammation, prevents fluid accumulation, and minimises relapses, while avoiding the long-term adverse effects linked to corticosteroid use [4]. Our findings align with the existing literature, supporting the use of colchicine as a first-line therapeutic option in recurrent serositis, even in cases where the genetic confirmation of an autoinflammatory syndrome is unavailable [4-6]. Early consideration of colchicine in patients with unexplained recurrent serositis may reduce unnecessary investigations, shorten the diagnostic journey, and improve outcomes.
Conclusions
IRS poses a considerable diagnostic challenge because of its nonspecific clinical features and wide-ranging differential diagnoses. In addition to excluding infections - both common and rare, such as pneumonia, HIV, and TB - clinicians must remain vigilant to avoid missing an underlying malignancy. A focused history and examination, including travel history, gynaecological history (where relevant), and drug use, is also vital to refine differential diagnoses. This case of recurrent serositis illustrates an inflammatory phenotype where resolution of symptoms occurred only after pharmacological intervention. Such cases are rare and unique and often pose a challenge in establishing a specific diagnosis. Importantly, autoinflammatory and recurrent inflammatory conditions should remain part of the differential when no clear cause is identified. In cases where IRS is considered, colchicine may represent an effective first-line therapeutic option, offering sustained symptom resolution and prevention of relapse. Early initiation of colchicine could therefore improve patient outcomes in similar scenarios.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J Adler Y Charron P Imazio M 292129643620152632011210.1093/eurheartj/ehv 318PMC 7539677 · doi ↗ · pubmed ↗
- 2Causes of polyserositis: a systematic review J Pers Med Stoichitoiu LE Ionescu GD Neatu I Baicus C 4613202310.3390/jpm 13050834 PMC 1022376237241003 · doi ↗ · pubmed ↗
- 3Regulated in development and DNA damage responses 1 (REDD 1) links stress with IL-1β-mediated familial Mediterranean fever attack through autophagy-driven neutrophil extracellular traps J Allergy Clin Immunol Skendros P Chrysanthopoulou A Rousset F 1378138714020172834291510.1016/j.jaci.2017.02.021 · doi ↗ · pubmed ↗
- 4Therapeutic management of idiopathic recurrent serositis: a retrospective study Eur Rev Med Pharmacol Sci Massaro MG Rigante D Sicignano LL Verrecchia E De Vito F Gasbarrini A Manna R 335233592420203227145310.26355/eurrev_202003_20703 · doi ↗ · pubmed ↗
- 5Systemic autoinflammatory disease diagnoses in a single year from a UK national referral centre Rheumatology (Oxford) Caterson HC Papadopoulou C Peet C Lachmann HJ 421842266420254012816910.1093/rheumatology/keaf 165 · doi ↗ · pubmed ↗
- 6Idiopathic recurrent serositis-off the beaten track Respirol Case Rep Roy MT Loh CH Sriranganathan M Takano Pena AM Raghuram J 09202110.1002/rcr 2.859PMC 850625934667614 · doi ↗ · pubmed ↗
- 7The diagnosis of pleural effusions Expert Rev Respir Med Porcel JM Azzopardi M Koegelenberg CF Maldonado F Rahman NM Lee YC 801815920152644932810.1586/17476348.2015.1098535 · doi ↗ · pubmed ↗
- 8Patient experiences and challenges in the management of autoinflammatory diseases-data from the International FMF and AID Global Association J Clin Med Rech J Schett G Tufan A 161813202410.3390/jcm 13051199 PMC 1093182538592017 · doi ↗ · pubmed ↗