A Wolf in Sheep's Clothing: Extensive Musculoskeletal and Cutaneous TB Masquerading as Primary Erythema Nodosum
Tanner Shull, Hemil Gonzalez

TL;DR
A man with a history of TB and a weakened immune system was misdiagnosed with a skin condition for months before being correctly diagnosed with musculoskeletal tuberculosis.
Contribution
Highlights the diagnostic challenges of musculoskeletal TB and the importance of considering TB in immunocompromised patients with atypical symptoms.
Findings
The patient's symptoms were initially misdiagnosed as erythema nodosum and bacterial cellulitis.
MRI and intraoperative cultures confirmed musculoskeletal TB with pan-sensitive M. tuberculosis.
TB should be considered in immunocompromised patients with symptoms unresponsive to standard treatments.
Abstract
Tuberculosis (TB) causes substantial morbidity and mortality globally, with continued endemicity in developing populations. Most cases of primary TB present as pulmonary TB; however, between 10% and 20% include extrapulmonary manifestations. Almost 26% of extrapulmonary manifestations include musculoskeletal TB. The risk of reactivation of latent TB is approximately 10% per year and is most common in those with immunocompromising conditions. Diagnosis of extrapulmonary TB remains elusive because of atypical presentation. We present a case of a 71-year-old man with a history of renal transplantation and previously treated latent TB who presented with worsening left lower extremity pain and swelling over the previous six months. Initially, the patient was unsuccessfully treated for presumed bacterial cellulitis with several rounds of antibiotics. The patient was then seen by Dermatology,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
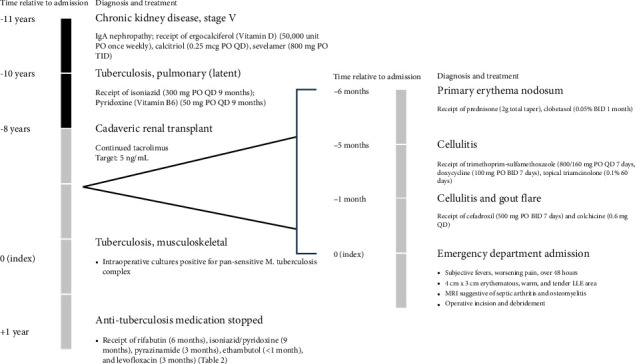 Figure 1
Figure 1 Figure 2
Figure 2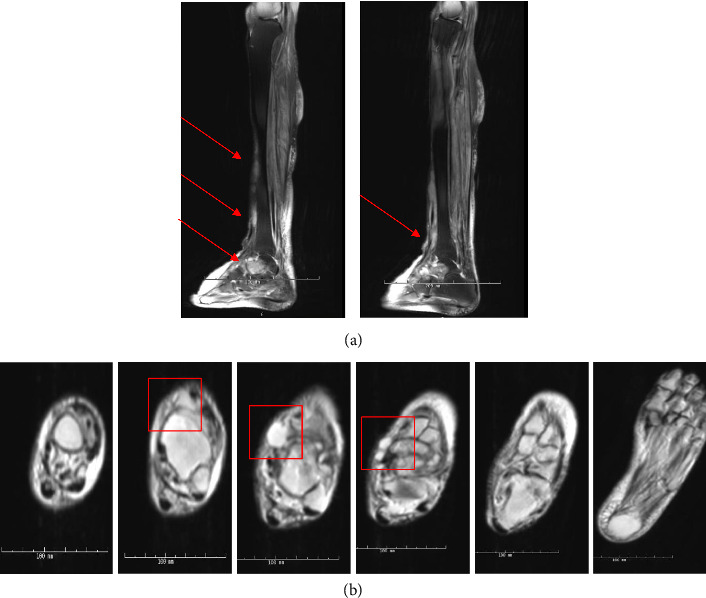 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Dermatological and COVID-19 studies · Drug-Induced Adverse Reactions
Summary
- • Premature closure on left lower extremity erythema nodosum as a primary diagnosis from targeted limb evaluation.
- • Anchoring on the diagnosis of erythema nodosum once lymphangitic spread began to develop.
- • Immunocompromised patient with a high risk of extrapulmonary TB (EPTB) given history of/prior renal transplant and previous history of latent pulmonary TB.
1. Introduction
Tuberculosis (TB) is the most substantial infectious killer from a single pathogen globally [1]. An estimated 1.7 billion people worldwide are latently infected with TB (LTBI) [2]. Among those without immunocompromised conditions, progression to primary TB remains below 10% [3–5]. In 2023, approximately 10.8 million people globally had primary TB, with 1.3 million deaths [1].
Most primary TB cases reported refer to pulmonary manifestations. However, between 10% and 20% of all primary TB may include extrapulmonary manifestations [6–8]. Extrapulmonary TB (EPTB) includes TB manifestations in pleural, lymphatic, musculoskeletal, and other body compartments not associated with the lungs [9]. EPTB prevalence is often underestimated, given underreporting in areas of high incidence [10, 11], limited sampling of extrapulmonary sites [12, 13], and frequent concomitant involvement that is reported as pulmonary TB only [14, 15]. Furthermore, microbiological tests for pulmonary TB, such as PCR and sputum culture, are less predictive of EPTB involvement. In EPTB, samples from debridement may not always be available [16, 17].
We present a case highlighting the importance of a comprehensive evaluation and high index of suspicion of reactivated LTBI in the context of an immunocompromised host.
2. Case
A 71-year-old man originally from a TB-endemic country presents with worsening lower extremity swelling and redness over the previous six months (Figure 1). His past medical history is significant for cadaveric renal transplant 7 years prior. Prior to CRT, he was found to have LTBI and received a 9-month INH/B6 regimen. Upon completion of therapy, his chest X-ray remained unchanged, and he proceeded with CRT. Immediately following CRT, antirejection medications included alemtuzumab (Campath), tacrolimus, mycophenolate, and prednisone. Since CRT, he has maintained serum tacrolimus levels of 5 ng/mL.
Six months before index admission, he presented to clinic with “ill-defined erythematous plaques to the left lateral leg” (Figure 2(a)), which was diagnosed as primary erythema nodosum. He was treated with tapered oral prednisone and topical clobetasol.
The following month, he experienced several episodes of swelling and redness of the limb. He was started on trimethoprim-sulfamethoxazole for cellulitis. His symptoms persisted, however, which prompted a medication switch to doxycycline and topical triamcinolone.
His lesions continued to progress for the next 3 months. He received cefadroxil and colchicine for a suspected gout flare compounded with cellulitis despite neither history of gout nor altered biomarkers. Notably, the patient endorsed improved redness and swelling, but no improvement in pain.
The patient presented to the emergency department one month later with subjective fevers of 101^o^F and worsening left lower extremity swelling, redness, and pain for the previous three days. On exam, the patient was ill-appearing but in no acute distress, with pitting edema to shins bilaterally with a 4 × 3-cm area of warmth, induration, tenderness, and erythema over the anterior shin of the lower left extremity (Figure 2(b)). Initial labs showed elevated inflammation markers (CRP and ESR). Blood count showed acute elevated neutrophils and lymphopenia. The patient was also chronically anemic and thrombocytopenic. An MRI was obtained, which demonstrated septic arthritis of the talonavicular joint, talus and navicular osteomyelitis, and infectious tenosynovitis of the posterior tibial tendon (Figure 3). The patient was scheduled for an operative incision and drainage of tissue.
In the operating room, gross purulence was found in the dorsal talonavicular joint capsule with significant joint synovitis. Upon blunt dissection and debridement, additional purulence was noted tracking to the hindfoot. An accessory incision was made with additional gross purulence along the posterior tibial tendon sheath, which appeared degenerated. A second operation was scheduled and performed, showing further gross purulence and completely lysed talonavicular joint cartilage from the subchondral bone. Samples from each section were obtained and sent for culture (Table 1).
Acid-fast bacilli (AFB) were identified by fluorochrome stain, and M. tuberculosis complex was identified by DNA probe assay. A total of six operating room samples were evaluated (Table 1). Three sputum samples were obtained, with one sample showing M. tuberculosis complex by DNA probe assay, despite a negative fluorochrome stain. The other two samples were negative for M. tuberculosis complex following 8 weeks of incubation. All samples were found to be pan-susceptible M. tuberculosis complex (Table 2).
Anti-TB medication was started with rifabutin instead of rifampin to prevent drug interactions with tacrolimus. Approximately 1 week following initiation, liver function tests (LFTs) were consistently elevated for unclear reasons. The patient was found to have reactivated hepatitis B infection (VL > 6M copies/mL) and was started on entecavir. After 12 months of therapy, the HBV viral load was rechecked and reported as 153 copies/mL.
LFTs were continually monitored, and the patient completed 2 months of intensive RIPE therapy before transitioning to RIF/INH therapy (Table 2). Given pan-susceptibility, ethambutol therapy was discontinued after 1 month. The patient experienced a lapse in treatment during Month 6 because of acute thrombocytopenia. Approximately 1 month later, he was restarted on RIF/INH but quickly discontinued because of concern for rifabutin allergy. The patient finished the remaining 3 months of anti-TB therapy on INH and levofloxacin (Table 2).
Approximately 1 year after treatment initiation and upon receipt of 9 months of anti-TB therapy, the patient's anti-TB medications were stopped. He continues to do well without any relapse.
3. Discussion
We present a case of a patient born in a TB-endemic country with a past medical history significant for CRT and LTBI currently receiving immunosuppressive therapy. He had been experiencing chronic lymphocutaneous abnormalities in his lower extremities without significant systemic symptoms. Notably, his symptoms had neither responded to typical antibacterial therapies nor corticosteroids as he was being managed alternatively for bacterial as well as primary inflammatory processes. By index admission, he had systemic symptoms including fevers, malaise, and new onset pain localized to joints and other musculoskeletal structures of his lower extremities. Intraoperative cultures grew pan-susceptible M. tuberculosis complex.
This case highlights heuristic pitfalls physicians may experience when evaluating patients with clinically evident, albeit undiagnosed TB.
Prioritizing primary inflammatory causes versus infectious causes in our immunocompromised patient resulted in missed diagnostic evaluations for opportunistic infections. An erythematous, inflamed plaque in a transplant patient should be considered infectious until diagnostically proven otherwise. Transplant patients are a high-risk group due to antirejection therapies. In antirejection therapies, lymphocytes are primary targets, which permit the reactivation of latent TB [18]. Tacrolimus specifically inhibits inflammatory processes involving IL-2 transcription, degranulation of immune cells, and T-cell proliferation [19]. Each predisposes LTBI to activation and secondary infection.
False reassurance due to prior therapy represents another heuristic error. Given its long duration of treatment and side effect profile, completion rates of LTBI therapy remain low [20]. Furthermore, this patient presented with a classic syndrome of erythema nodosum, which has been associated with TB [21, 22]. Traditionally, erythema nodosum presents as bilateral and symmetric multinodular foci. Despite our patient's atypical appearance of erythema nodosum, providers did not investigate secondary causes of erythema nodosum or obtain a skin biopsy, which incorrectly adjudicated symptoms to a primary inflammatory etiology rather than an infectious one. Glucocorticoids give the appearance of improvement even in infectious conditions by reducing inflammation. Deeper tissues such as tendons, joints, and bones were still affected in our patient. Despite worsening clinical presentation, providers continued to treat for primary erythema nodosum, until his index emergency department admission.
In conclusion, LTBI reactivation in immunosuppressed patients can be prevented with judicious use of additional immunosuppressive medications and establishing a comprehensive differential diagnostic evaluation for patients from TB-endemic regions with significant past medical and surgical history. Physicians can further suspect LTBI reactivation in worsening inflammatory and immune processes not responsive to other refractory anti-inflammatory and antibiotic therapies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Global Tuberculosis Report 20242024 https://www.who.int/publications/i/item/9789240101531
- 2Houben R. M. G. J. Dodd P. J. The Global Burden of Latent Tuberculosis Infection: A Re-Estimation Using Mathematical Modelling P Lo S Medicine 20161310 p. e 100215210.1371/journal.pmed.10021522-s 2.0-84994259668 PMC 507958527780211 · doi ↗ · pubmed ↗
- 3Comstock G. Livesay V. Woolpert S. The Prognosis of a Positive Tuberculin Reaction in Childhood and Adolescence American Journal of Epidemiology 197499213113810.1093/oxfordjournals.aje.a 1215932-s 2.0-00159513134810628 · doi ↗ · pubmed ↗
- 4Shea K. M. Kammerer J. S. Winston C. A. Navin T. R. Horsburgh C. Robert Jr. Estimated Rate of Reactivation of Latent Tuberculosis Infection in the United States, Overall and by Population Subgroup American Journal of Epidemiology 2014179221622510.1093/aje/kwt 2462-s 2.0-8489151550124142915 PMC 5547435 · doi ↗ · pubmed ↗
- 5Vynnycky E. Fine P. E. M. Lifetime Risks, Incubation Period, and Serial Interval of Tuberculosis American Journal of Epidemiology 2000152324726310.1093/aje/152.3.2472-s 2.0-003425554710933272 · doi ↗ · pubmed ↗
- 6Ilgazli A. Boyaci H. Basyigitİ. Yildiz F. Extrapulmonary Tuberculosis: Clinical and Epidemiologic Spectrum of 636 Cases Archives of Medical Research 200435543544110.1016/j.arcmed.2004.05.0082-s 2.0-1094426938715610915 · doi ↗ · pubmed ↗
- 7Lin J. N. Lai C. H. Chen Y. H. Risk Factors for Extra-Pulmonary Tuberculosis Compared to Pulmonary Tuberculosis International Journal of Tuberculosis & Lung Disease: The Official Journal of the International Union Against Tuberculosis and Lung Disease 200913562062519383196 · pubmed ↗
- 8Rieder H. L. Snider D. E. Cauthen G. M. Extrapulmonary Tuberculosis in the United States American Review of Respiratory Disease 1990141234735110.1164/ajrccm/141.2.3472-s 2.0-00251259082301852 · doi ↗ · pubmed ↗