Unveiling a Hidden Threat: Wellens Syndrome as a Manifestation of Critical In-Stent Restenosis
John M Sousou, Ty J Merry, Christopher Marsalisi, Abhinav Karan, Pramod Reddy

TL;DR
This paper reports a rare case where Wellens syndrome, a heart condition, was caused by a blockage in a previously placed artery stent.
Contribution
The novelty is demonstrating Wellens syndrome as a manifestation of in-stent restenosis rather than atherosclerotic plaque rupture.
Findings
A patient with Wellens syndrome had 80% in-stent restenosis in a previously implanted mid-LAD stent.
ECG changes consistent with Wellens syndrome type A were observed despite lack of chest pain and normal troponin levels.
The case highlights the importance of recognizing Wellens syndrome in patients with prior stent placement.
Abstract
Wellens syndrome is defined by characteristic T-wave changes seen on an electrocardiogram (ECG), indicating critical stenosis of the proximal or middle left anterior descending artery (LAD). Diagnosis is challenging, as patients often lack chest pain during ECG recording and have normal or mildly elevated troponin levels. Wellens syndrome classically arises de novo from a rupture of an atherosclerotic plaque, causing arterial obstruction. Although rare, some studies have reported Wellens syndrome secondary to in-stent restenosis (ISR). We present a case of Wellens syndrome caused by ISR of a previously implanted mid-LAD stent. The patient exhibited concerning ECG changes with new biphasic T-waves in leads V1 to V3, consistent with Wellens syndrome type A. Left heart catheterization revealed 80% ISR of his mid-LAD stent. We aim to highlight the critical importance of promptly recognizing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
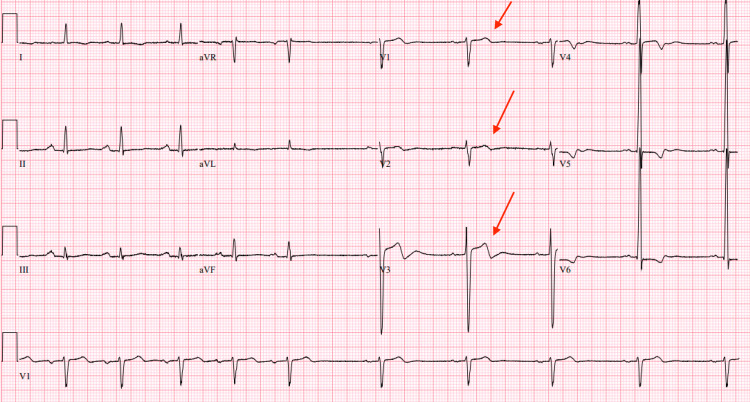 Figure 1
Figure 1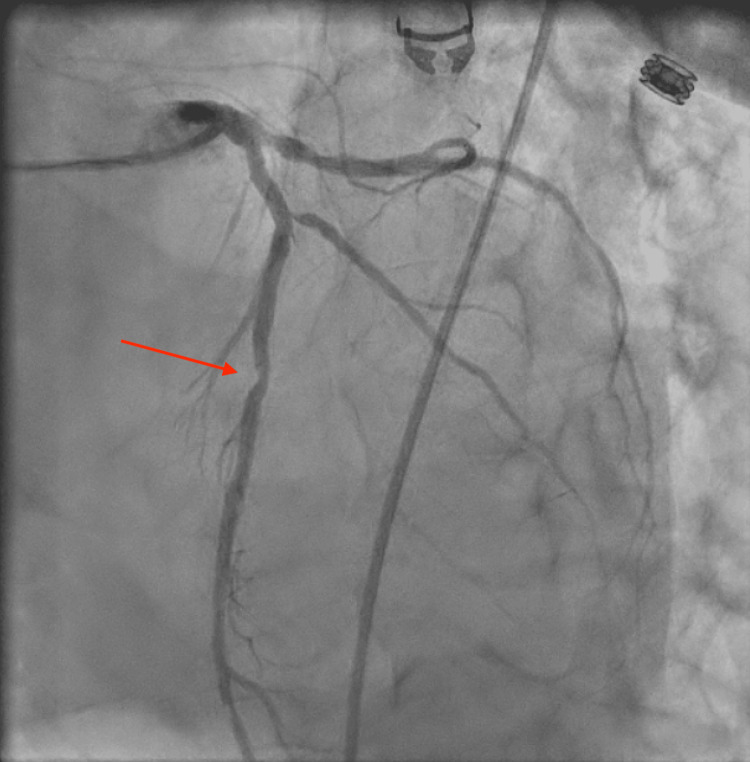 Figure 2
Figure 2| Diagnostic Criteria for Wellens Syndrome |
| Type A: Biphasic T-waves in precordial leads (most commonly V2 and V3) OR Type B: Deep symmetric inverted T-waves in the precordial leads (typically V2 and V3) |
| Minimal or no ST segment elevation |
| Minimal of no elevation in cardiac enzymes |
| Prior history of angina but no chest pain during ECG |
| Sustained R-wave progression |
| Absence of pathological Q-waves |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Acute Myocardial Infarction Research · Cardiac Imaging and Diagnostics
Introduction
Coronary artery disease (CAD) is the leading cause of death in the United States and is often referred to as a silent killer, as it can progress asymptomatically in many adults until the onset of acute coronary syndrome, a feared complication [1]. Wellens syndrome, also known as acute coronary T-wave syndrome, is the epitome of this reference as it may be “silent” to both patients and medical providers. Wellens syndrome is characterized by a distinct ECG pattern that typically occurs without other signs of ischemia, such as ST-segment elevations or pathological Q-waves, and often presents without the classic symptoms or ECG features of acute coronary syndrome.
Wellens syndrome can be classified as type A or type B based on ECG findings. Type A, observed in approximately 24% of cases, features biphasic T waves in the precordial leads V2 and V3. Type B, seen in about 76% of patients, is characterized by deeply inverted symmetric T-waves primarily seen in leads V2 and V3 [2]. Studies have shown that the appearance of the Wellens pattern had a high specificity (89%) and positive predictive value (86%) for severe stenosis of the left anterior descending artery (LAD) [3]. Wellens syndrome can present with ECG changes that overlap with those seen in other conditions, making accurate diagnosis and careful ECG interpretation crucial. For instance, coronary artery spasm, sometimes referred to as pseudo-Wellens syndrome, can mimic these ECG changes without the presence of significant atherosclerotic stenosis [2]. Additionally, myocardial bridging can produce similar ECG findings, especially during periods of increased myocardial oxygen demand [4].
As with other acute coronary syndromes, the timely recognition and therapeutic approach of Wellens syndrome is integral in the appropriate management of this condition, as it can indicate critical stenosis of the LAD. We describe the case of an asymptomatic patient with ECG changes consistent with Wellens syndrome who was found to have critical in-stent restenosis (ISR) of the mid-LAD.
Case presentation
The patient is an 83-year-old man with a history of heart failure with reduced ejection fraction secondary to ischemic cardiomyopathy status-post percutaneous coronary intervention (PCI) to the mid-left anterior descending artery (LAD) four years prior, hypertension, and chronic obstructive pulmonary disease (COPD). The patient initially presented for worsening dyspnea with reported substernal chest pain on exertion and was admitted to the hospital for a COPD exacerbation. During his admission, an ECG was noted to have new biphasic T-waves in leads V1 to V3, consistent with Wellens syndrome type A (Figure 1). His troponin levels taken at hours zero, one, and three were all negative.
ECG showing biphasic T-waves with initial positivity and terminal negativity in leads V1, V2, and V3, consistent with Wellens syndrome type A (red arrows).
The patient denied any chest pain throughout his hospital course but reported periods of angina prior to admission, specifically on exertion. He was ultimately taken for a left heart catheterization (LHC), which revealed 80% ISR of his previously placed stent in the mid-segment of the LAD (Figure 2). The patient underwent PCI with successful stenting of the mid-segment of the LAD at the bifurcation with the first diagonal artery (D1) using a 3.0 x 15mm Onyx Frontier drug-eluting stent (DES). The new stent was deployed in an overlapped fashion with the existing stent in the mid-LAD, and the existing stent was post-dilated using a balloon. Following PCI, the patient was initiated on triple therapy with aspirin, clopidogrel, and heparin, which was continued for three days until discharge. At the time of discharge, he was transitioned to dual antiplatelet therapy (DAPT) with aspirin and clopidogrel for a planned duration of one year.
Coronary angiography revealing 80% ISR at the mid-segment of the LAD (red arrow).
Our patient underwent initial follow-up with his primary care doctor and cardiologist within 14 days of hospital discharge, then routinely every six months. He remained adherent to DAPT through his one-year follow-up, at which point clopidogrel was discontinued. He has since continued to adhere to planned lifelong aspirin monotherapy. The patient has a higher chance of target lesion revascularization (TLS) after five years per the SORT OUT studies, which compared major adverse cardiac events and TLS [5]. Continuation of monitoring and routine EKG would be recommended in the outpatient setting to capture potential complications in the future.
Discussion
Wellens syndrome represents a critical warning sign of severe proximal or mid-LAD stenosis, often signaling a pre-infarction state that requires prompt intervention. Like other forms of ACS, it shares common cardiovascular risk factors such as hypertension, diabetes mellitus, hyperlipidemia, tobacco smoking, and obesity [6]. Typically, the underlying pathophysiology involves rupture of an atherosclerotic plaque leading to abrupt arterial narrowing and impending myocardial infarction. In our case, however, the patient’s Wellens pattern was attributable to ISR, highlighting an important but less frequently discussed cause of LAD obstruction. Although Wellens syndrome is primarily linked to de novo stenosis of the LAD, there is evidence that it may, on rare occasions, arise from restenosis of a previously implanted stent [7]. There are several differences in the pathophysiology of Wellens between de novo coronary artery disease vs ISR. ISR is associated with biological and mechanical factors that promote stenosis or plaque rupture [8]. Exaggerated homeostatic healing in response to the arterial wall damage during stent implantation is a common biological response, whereas malposition or stent fracture is associated with mechanical pathology [8]. Based on the timeframe of our patient’s initial PCI, it could be theorized that the mechanism behind his ISR would be a malpositioned stent that may not have completely revascularized the site of the previous occlusion. ISR remains a clinically significant concern even years after PCI. Despite advancements in DES technology, restenosis rates persist, particularly among patients with complex lesions, diabetes mellitus, or a history of prior myocardial infarction. In our patient, the four-year interval between stent placement and ISR reflects the ongoing risk for restenosis even in patients seemingly stable on optimal medical therapy.
Our patient’s ECG displayed biphasic T-waves in leads V1 to V3, consistent with Wellens syndrome type A, where T-waves initially deflect positively before terminal negativity. Our patient met each of the criteria for Wellens syndrome, as shown in Table 1.
Although Wellens syndrome type A primarily presents with biphasic T-waves in leads V2 and V3, studies have shown that biphasic T-waves may also be observed in leads V1 and V4 [9]. Similarly, the deep inverted T-waves seen in Wellens syndrome type B can occasionally extend from leads V1 to V4 [9]. Recognizing these patterns across a broader range of precordial leads can aid in the early detection and management of this high-risk condition. Additionally, Wellens syndrome is typically identified during asymptomatic periods or in patients with resolved chest pain. In our case, the patient denied active chest pain during ECG acquisition but reported occasional exertional angina prior to admission. This temporal dissociation between symptoms and ECG changes is another diagnostic hallmark noted in Wellens syndrome.
The patient’s ECG changes and clinical picture prompted us to pursue further ischemic workup with an LHC, given his cardiac history and prior PCI. The LHC revealed 80% stenosis of his previously placed stent in the mid-LAD, necessitating repeat PCI with stent placement. Management involves strict adherence to DAPT with aspirin and a P2Y12 inhibitor (such as clopidogrel) to reduce the risk of stent thrombosis and restenosis. Despite medical therapy, late ISR remains a threat, reinforcing the importance of timely follow-up care and continued risk factor modification for these patients.
Conclusions
Patients with new T-wave changes consistent with Wellens syndrome should undergo prompt ischemic evaluation, as this pattern indicates critical LAD stenosis. While literature on Wellens syndrome arising from de novo coronary lesions has been documented in various contexts, research on Wellens syndrome as a manifestation of ISR remains extremely sparse. Our goal is to elevate awareness and recognition among providers of the rare but possible presentation of Wellens syndrome in patients with a history of stent placement.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review J Epidemiol Glob Health Ralapanawa U Sivakanesan R 1691771120213360511110.2991/jegh.k.201217.001PMC 8242111 · doi ↗ · pubmed ↗
- 2A classic pattern of Wellens syndrome on ECG: a case report J Community Hosp Intern Med Perspect Romero J Jesani S Romero AL Elkattawy S Sookdeo J Khandait H 596213202310.55729/2000-9666.1160 PMC 1016621637168067 · doi ↗ · pubmed ↗
- 3Characteristics of Wellens' syndrome in the current PCI era: a single-center retrospective study Emerg Med Int Zhou L Gong X Chen H Dong T Cui HH Li H 8865553202320233700875710.1155/2023/8865553 PMC 10065856 · doi ↗ · pubmed ↗
- 4Wellens syndrome Stat Pearls Miner B Grigg WS Hart EH Treasure Island, FL Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 482490/29494097 · pubmed ↗
- 5Comparison of outcome after percutaneous coronary intervention for de novo and in-stent restenosis indications Am J Cardiol Jakobsen L Christiansen EH Freeman P 1823520253946140110.1016/j.amjcard.2024.10.019 · doi ↗ · pubmed ↗
- 6Repeat Wellens' syndrome: case report of critical proximal left anterior descending artery restenosis J Emerg Med Nisbet BC Zlupko G 3053083920101839484710.1016/j.jemermed.2007.10.043 · doi ↗ · pubmed ↗
- 7Wellens’ syndrome: a bad omen Cardiology Coutinho Cruz M Luiz I Ferreira L Cruz Ferreira R 10010313720172819635810.1159/000455911 · doi ↗ · pubmed ↗
- 8SCAI expert consensus statement on management of in-stent restenosis and stent thrombosis J Soc Cardiovasc Angiogr Interv Klein LW Nathan S Maehara A 10097122023 https://doi.org/10.1016/j.jscai.2023.1009713913165510.1016/j.jscai.2023.100971 PMC 11308135 · doi ↗ · pubmed ↗