N-Methyl-D-Aspartate (NMDA) Receptor Encephalitis Without Electroencephalogram Abnormalities or Cerebrospinal Fluid Pleocytosis Associated With a Tiny Ovarian Teratoma: A Case Report
Akihiro Miyashita, Kensuke Takaoka, Jatinder Lachar

TL;DR
A rare case of NMDA receptor encephalitis is reported in a woman with a tiny ovarian teratoma, despite normal EEG and CSF results.
Contribution
Highlights the importance of NMDA receptor antibody testing even when typical diagnostic markers are absent.
Findings
NMDA receptor encephalitis was diagnosed in a patient with normal EEG and no CSF pleocytosis.
A 7 mm ovarian teratoma was identified as the associated tumor.
The case emphasizes the need for antibody testing in atypical presentations.
Abstract
N-methyl-D-aspartate (NMDA) receptor encephalitis is one of the autoimmune disorders characterized by neuropsychiatric symptoms, most commonly associated with ovarian teratoma. While detection of NMDA receptor antibody in cerebrospinal fluid (CSF) is the diagnostic standard, it is often limited by a delayed turnaround time. Abnormal electroencephalogram (EEG) findings and pleocytosis in CSF analysis are frequently observed, and computed tomography (CT) can aid in identifying an underlying ovarian teratoma. Here we report the case of a 36-year-old female who presented with acute psychosis, had a normal EEG and no CSF pleocytosis, and was later diagnosed with NMDA receptor encephalitis associated with a 7 mm ovarian teratoma. This case underscores the diagnostic challenges in the setting of a normal EEG and no CSF pleocytosis, which emphasizes the importance of NMDA receptor antibody…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
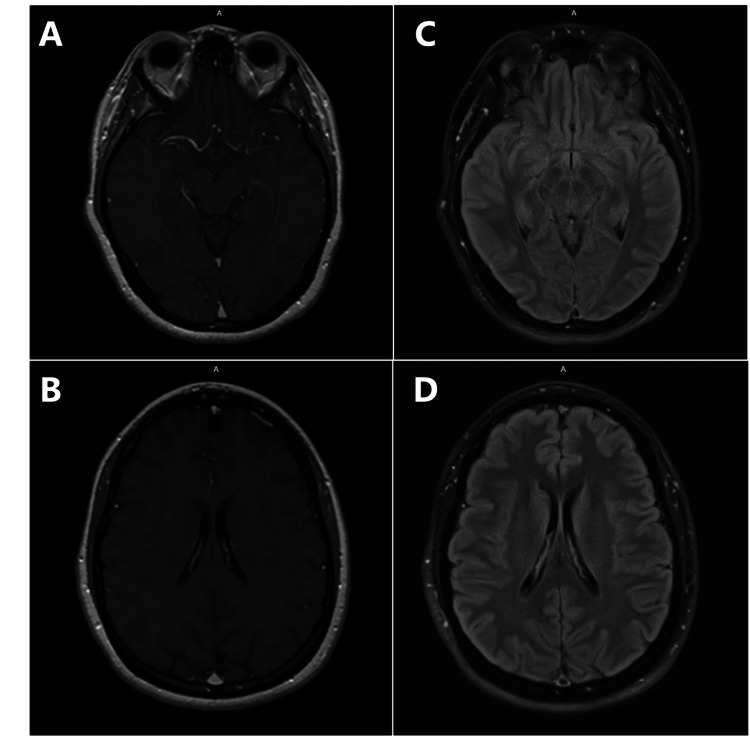 Figure 1
Figure 1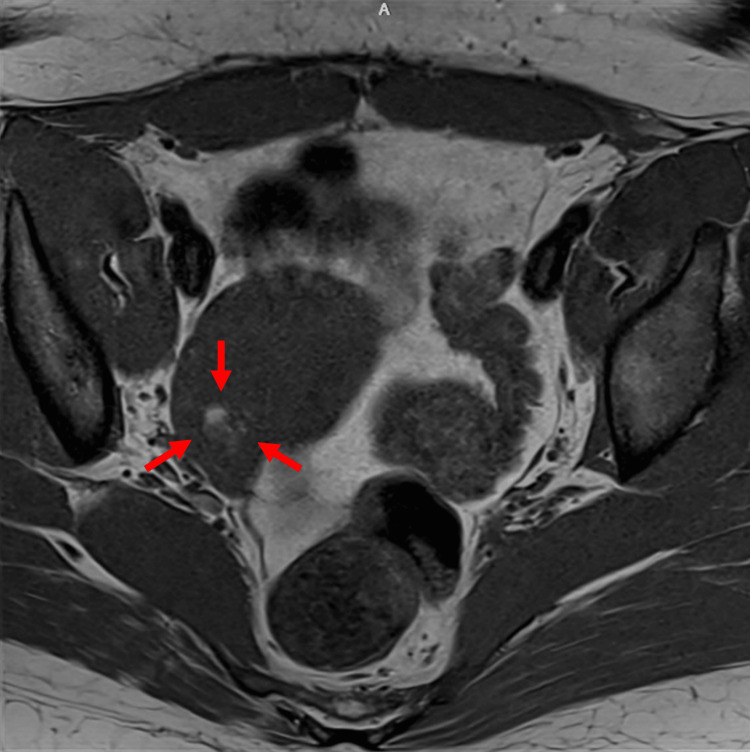 Figure 2
Figure 2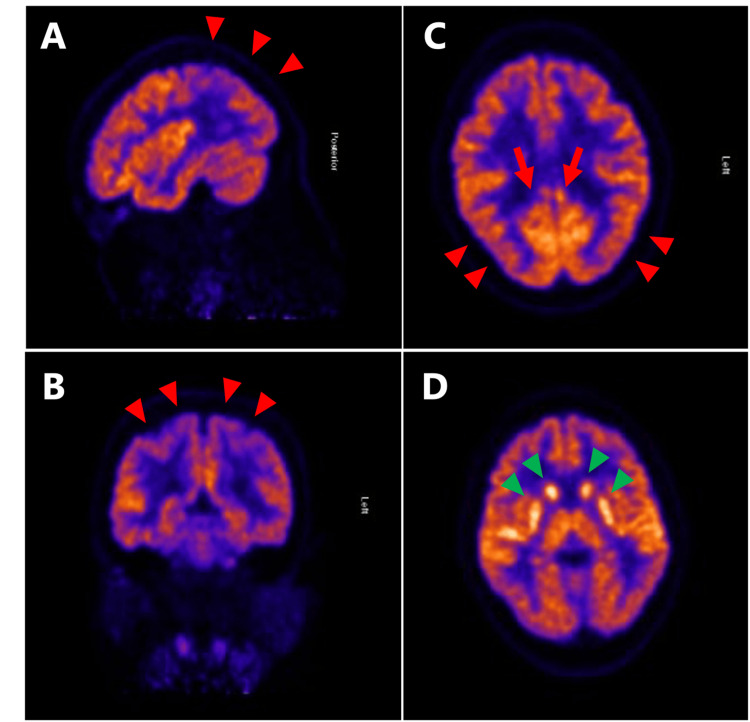 Figure 3
Figure 3| Serum laboratory analysis | Result |
| AMPA-R | Negative |
| Amphiphysin | Negative |
| Anti-Glial Nuclear Ab, Type 1 | Negative |
| Anti-Neuronal Nuclear Ab, Type 1 | Negative |
| Anti-Neuronal Nuclear Ab, Type 2 | Negative |
| Anti-Neuronal Nuclear Ab, Type 3 | Negative |
| CASPR2-IgG | Negative |
| GABA-B-R Ab | Negative |
| GAD65 Ab | Negative |
| GFAP IFA | Negative |
| LGI1-IgG | Negative |
| mGluR1 Ab | Negative |
| NIF IFA | Negative |
| NMDA-R Ab | Positive |
| Purkinje Cell Cytoplas. Ab, Type 1 | Negative |
| Purkinje Cell Cytoplas. Ab, Type 2 | Negative |
| Purkinje Cell Cytoplas. Ab, Type Tr | Negative |
| CRMP-5-IgG | Negative |
| Neurochondrin IFA | Negative |
| Septin-7 IFA | Negative |
| DPPX Ab CBA | Negative |
| IGLON5 CBA | Negative |
| PDE10A Ab IFA | Negative |
| TRIM46 Ab IFA | Negative |
| CSF laboratory analysis | Result |
| AMPA-R Ab | Negative |
| Amphiphysin | Negative |
| AGNA-1 | Negative |
| ANNA-1 | Negative |
| ANNA-2 | Negative |
| ANNA-3 | Negative |
| CASPR2-IgG | Negative |
| CRMP-5 | Negative |
| GABA-B-R Ab | Negative |
| GAD65 Ab | Negative |
| GFAP IFA | Negative |
| LGI1-IgG | Negative |
| mGluR1 AB IFA | Negative |
| NIF IFA | Negative |
| NMDA-R Ab | Positive |
| Purkinje Type Tr | Negative |
| PCA-1 | Negative |
| PCA-2 | Negative |
| Neurochondrin IFA | Negative |
| Septin-7 IFA | Negative |
| DPPX Ab CBA | Negative |
| IGLON5 CBA | Negative |
| PDE10A Ab IFA | Negative |
| TRIM46 Ab IFA | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Neurological Disorders and Treatments · Genetics and Neurodevelopmental Disorders · Polyomavirus and related diseases
Introduction
N-methyl-D-aspartate (NMDA) receptor encephalitis is a rare autoimmune disorder caused by IgG1 antibodies leading to internalization and functional disruption of synaptic NMDA receptors. This results in decreased receptor density and subsequent neuropsychiatric symptoms [1,2]. It predominantly affects children and young female adults, and most cases are associated with ovarian teratoma [3]. Clinical presentation is characterized by a prodrome of fever, headache, or malaise followed by psychiatric symptoms, memory deficits, seizures, and decreased consciousness [4,5]. While the gold standard for diagnosis is the detection of NMDA-receptor antibody in cerebrospinal fluid (CSF), the results often take time to return [3]. Typical electroencephalogram (EEG) features seen in patients with NMDA receptor encephalitis are diffuse or focal slowing of background activity, and a normal EEG finding is rarely observed [6,7]. Furthermore, CSF analysis typically shows mild to moderate lymphocytic pleocytosis. In this report, we present a rare case of NMDA receptor encephalitis associated with a tiny ovarian teratoma, notably characterized by normal EEG findings and no CSF pleocytosis.
Case presentation
A 36-year-old female with a history of left ovarian dermoid status post left oophorectomy presented with an acute onset of psychosis. Her symptoms were characterized by fluctuating psychosis with agitation and memory deficits. The laboratory results, including complete blood count, electrolytes, renal and liver function tests, vitamin B12, folate, ammonia, HIV, syphilis, and thyroid function, were unremarkable. Urine drug screens were negative except for the positive result for tetrahydrocannabinol. The patient was initially admitted to the psychiatry unit and treated with valproate, lorazepam, and ziprasidone for a presumed primary psychiatric disorder, but there was no significant improvement. Therefore, the patient was transferred to the internal medicine unit for neurological workup. EEG showed a normal background associated with one episode of psychogenic non-epileptic seizure. Computed tomography (CT) of the head and magnetic resonance imaging (MRI) of the brain showed no acute abnormalities (Figure 1).
Radiological findings of the brain.Magnetic resonance imaging on T1 (A and B) and fluid-attenuated inversion recovery (FLAIR) (C and D) showed no acute infarct, hemorrhage, or mass lesion. The ventricles, cisterns, and sulci were not effaced.
CSF analysis demonstrated no white blood cells, glucose of 53 mg/dL, protein of 51 mg/dL (normal range: 15-45 mg/dL), and negative results on the meningitis PCR panel for E. coli K1, Haemophilus influenzae, Listeria, Neisseria, Streptococcus agalactiae, Streptococcus pneumoniae, cytomegalovirus, enterovirus, herpes simplex virus types 1 and 2, human herpesvirus 6, varicella, human parechovirus, and Cryptococcus. Serum autoimmune screening showed positive NMDA-receptor antibody (Table 1), whereas serum NMDA-receptor antibody titer was negative (less than 1:240). Vaginal ultrasound showed a 10 mm echogenic nodule in the right ovary. CT of the chest, abdomen, and pelvis revealed no evidence of malignancy, including an ovarian mass. The patient was empirically treated with a five-day course of intravenous immunoglobulin (0.4 mg/kg/day) and electroconvulsive therapy, leading to partial improvement of her symptoms. Subsequently, the CSF paraneoplastic panel came back positive for NMDA-receptor antibody (Table 2).
An MRI pelvis scan detected a possible 7 mm fatty lesion within the central right ovary without enhancement, representing a small dermoid lesion (Figure 2). Fluorodeoxyglucose positron emission tomography (FDG-PET) did not show evidence of malignancy. Additionally, FDG-PET of the brain (Figure 3) demonstrated significantly reduced glucose metabolism in the parietal lobes with extension into the occipital lobes, sparing the visual cortex, and in the lateral frontal lobes bilaterally. There was also hypermetabolic activity in the caudate, putamen, thalamus, and superior temporal cortices. These observations aligned with NMDA-receptor encephalitis. The patient had a right salpingo-oophorectomy, followed by rituximab therapy. The pathology result was consistent with an ovary with a mature cystic teratoma. Patient’s symptoms gradually improved after these treatments.
Radiological findings of ovarian teratoma.Magnetic resonance imaging showed a small fatty lesion within the central right ovary without enhancement (red arrow).
Fluorodeoxyglucose positron emission tomography (FDG-PET) findings of the brain.There is significantly reduced glucose metabolism in the parietal lobes (A, B, and C, red arrowheads), extending into the occipital lobes while sparing the visual cortex (C, red arrow). There is increased metabolism in the caudate, putamen, and thalamus (D, green arrowheads).
Discussion
We reviewed a case of NMDA receptor encephalitis without EEG abnormalities or CSF pleocytosis, associated with a 7 mm ovarian teratoma. NMDA receptor encephalitis is a rare autoimmune encephalitis, commonly associated with ovarian teratoma [1]. Fundamental treatment includes surgical removal of the detected tumor and immunosuppressive therapy, including high-dose corticosteroids, intravenous immunoglobulin (IVIG), or plasma exchange [3]. In our case, surgical removal and immunosuppressive therapy, including IVIG and rituximab, improved the symptoms.
Diagnosis of NMDA receptor encephalitis can sometimes be challenging. In this case, the patient’s psychosis was initially attributed to a primary psychiatric disorder. However, because her agitation and memory deficits failed to improve with psychiatric management, we proceeded with an expanded diagnostic workup. EEG is abnormal in most cases, typically showing non-specific, slow, and disorganized activity with electrographic seizures [3], and a normal EEG is reported in only about 4% of cases [7]. This case showed a normal EEG with one episode of psychogenic non-epileptic seizure, which made the diagnosis difficult. The reason for the normal EEG is unclear, but one possible explanation is that it was obtained during the early phase of the disease. One retrospective analysis reported that 20% of patients had normal EEGs within the first 14 days of symptom onset [6]. However, this analysis included only 10 patients at the early stage, underscoring the need for further investigation into EEG findings during the initial phase of the disease.
While detection of NMDA-receptor antibody in CSF is the gold standard for diagnosis and has a higher sensitivity (99%) compared to serum (68%), it often requires a prolonged turnaround time [8]. Although some studies suggested that antibody titers may correlate with disease severity, the presence of antibody is a key diagnostic clue even at low titers [9]. In our case, the NMDA-receptor antibody was detected in the serum, but the titer was negative, initially raising concern for a false-positive result. Furthermore, CSF analysis typically shows mild to moderate lymphocytic pleocytosis ranging from 10 to 100 cells/microL, especially in the early stages of the disease [10-13]. Additionally, mild elevation of CSF protein is also observed in 60% of patients [12]. These CSF abnormalities occur in 91%-94% of cases, while they might be normal early in the disease course [2,13]. In the present case, low titers of serum NMDA-receptor antibody and the absence of pleocytosis in CSF further complicated the diagnostic process.
In NMDA receptor encephalitis, brain FDG-PET typically shows relative hypermetabolism in the frontal and temporal cortices, marked hypometabolism in the parietal and occipital lobes, and hypermetabolism in the basal ganglia, with these patterns correlating with disease severity [14,15]. In our case, hypermetabolism of the frontal lobes was not seen, but hypometabolism in the parietal and occipital lobes, with increased metabolism of the basal ganglia, was consistent with NMDA receptor encephalitis. The basal ganglia play a crucial role in emotional regulation, and dysfunction in this region may have contributed to the development of paranoia in this case. In general, FDG-PET can provide results relatively quickly and may serve as a useful diagnostic tool to guide empiric treatment, particularly when symptoms are too severe to be managed with supportive care alone. Therefore, these FDG-PET findings may also become an important diagnostic tool, especially when other modalities such as CSF or EEG are inconclusive.
Conclusions
In conclusion, we present a rare case of NMDA receptor encephalitis with normal EEG and no pleocytosis, possibly caused by a tiny ovarian teratoma. Further research is warranted to clarify the relationship between ovarian teratoma and encephalitis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Antibody-mediated encephalitis N Engl J Med Dalmau J Graus F 84085137820182949018110.1056/NEJ Mra 1708712 · doi ↗ · pubmed ↗
- 2Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies Lancet Neurol Dalmau J Gleichman AJ Hughes EG 10911098720081885192810.1016/S 1474-4422(08)70224-2PMC 2607118 · doi ↗ · pubmed ↗
- 3Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis Lancet Neurol Dalmau J Lancaster E Martinez-Hernandez E Rosenfeld MR Balice-Gordon R 63741020112116344510.1016/S 1474-4422(10)70253-2PMC 3158385 · doi ↗ · pubmed ↗
- 4Anti-N-methyl-D-aspartate receptor encephalitis: characteristics and rapid diagnostic approach in the emergency department BMC Neurol Xu J Zhao N Guan H Walline JH Zhu H Yu X 2242220223571716210.1186/s 12883-022-02752-9PMC 9206331 · doi ↗ · pubmed ↗
- 5Frequency and temporal sequence of clinical features in adults with anti-NMDA receptor encephalitis presenting with psychiatric symptoms Psychol Med Gurrera RJ 270927164920193056074510.1017/S 0033291718003665 · doi ↗ · pubmed ↗
- 6Analysis of electroencephalogram characteristics of anti-NMDA receptor encephalitis patients in China Clin Neurophysiol Zhang Y Liu G Jiang MD Li LP Su YY 1227123312820172852738710.1016/j.clinph.2017.04.015 · doi ↗ · pubmed ↗
- 7Predictive value of electroencephalography in anti-NMDA receptor encephalitis J Neurol Neurosurg Psychiatry Sonderen AV Arends S Tavy DL 110111068920183013518710.1136/jnnp-2018-318376 · doi ↗ · pubmed ↗
- 8Anti-NMDA receptor encephalitis in the Netherlands, focusing on late-onset patients and antibody test accuracy Neurol Neuroimmunol Neuroinflamm Bastiaansen AE de Bruijn MA Schuller SL 9202210.1212/NXI.0000000000001127 PMC 869655334937737 · doi ↗ · pubmed ↗